Download presentation
Presentation is loading. Please wait.

1
بسم الله الرحمن الرحيم

2
ANAESTHETIC MANAGEMENT OF AORTIC ARCH SURGERY

3
Aortic arch surgery Still one of the risky and complicated operations.
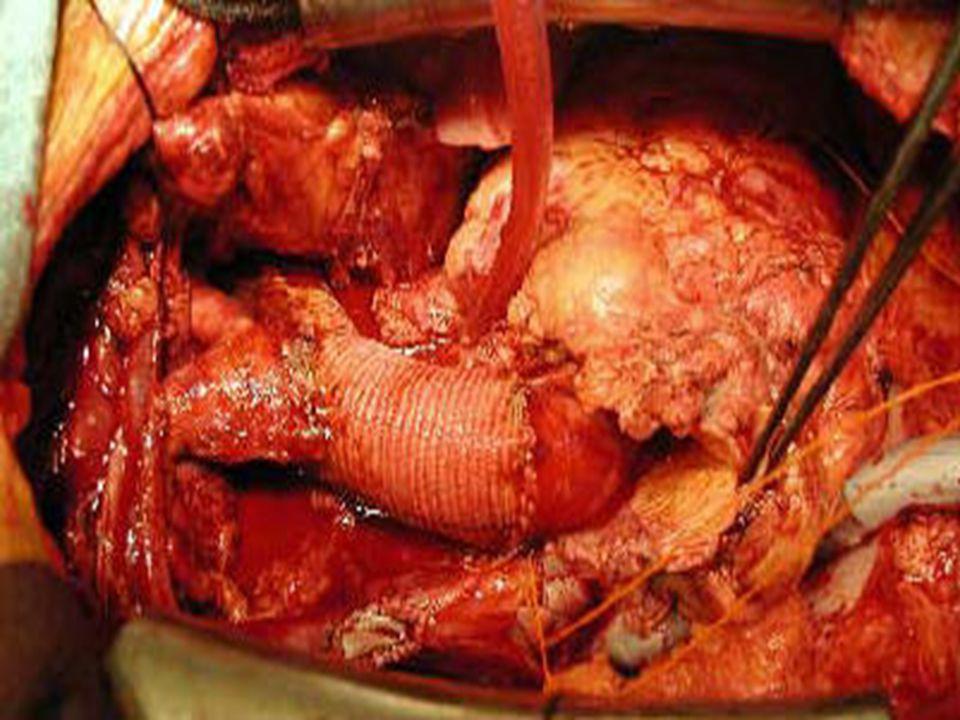
In spite of advanced surgical techniques. In spite of advance in anaesthetic techniques. The traditional two anastomosis reconstruction (Figure 1)
")
5
Usually, the dilated arch is accompanied by an ascending (Figure 2) or descending (Figure 3) aortic aneurysm, or a combination of all three areas (Figure 4).
 or descending (Figure 3) aortic aneurysm, or a combination of all three areas (Figure 4).")
6
INDICATION Urgent indications Rupture of an atherosclerotic aneurysm.
Rupture of false lumen of a type A aortic dissection. Type A dissection with extensive intimal tears in the arch. Mycotic aneurysms

7
INDICATION Elective indications Arch aneurysms greater than 6cm .
Saccular aneurysms with rapid enlargement (1/cm/y) or presence of symptoms.
 or presence of symptoms.")
8
Preoperative evaluation:
Elderly >60 y. Diabetic. Atherosclerotic diseases. Hypertension, ischemic heart diseases. Have peripheral vascular disease. Proper assessment of pulmonary function is done.

9
Preoperative investigation
Routine laboratory investigation as blood picture, Kidney, liver functions tests and coagulation profile. Chest X ray. ECG. Echocardiography: to assess LT. ventricular function and exclude valvular diseases.

10
Diagnosis and evaluation of the AA aneurysm
CT scan of the entire aorta. MRI which is the preferred modality for imaging. Coronary angiograph. With visualization of the brachiocephalic vessels especially in patients with aneurysm of the ascending aorta in whom Bentall; procedure may be required.

11
Its very important Management of CAD should be done preoperative either medically using antiischemic measures or even coronary artery bypass surgery or angiogplasty is considered. Proper neurological examination should be done preoperatively and a carotid and vertebral duplex ultrasound is requested if there is a history of transient ischemic attacks or strokes. A history of a focal cerebral insult is not a contraindication to surgery. CT scan in theses patients is carried out.

12
Intraoperative management:
Anaesthesia for AA repair is no different from that for conventional open heart surgery. Selective ventilation of the right lung to help substantial dissection and mobilization of the descending thoracic aortic.

13
MONITORING Basic haemodynamic monitoring is routinely used.
Pulmonary artery catheterization. Transoesophageal. Cerebral oximetry confirm the adequacy of cerebral perfusion and oxygenation. Transcranial Dopper is so more sensitive in detecting embolic events and confirming cerebral blood flow.

14
Femoral vessels are still commonly used for cannulation.
Cannulation sites Right axillary artery Usually soft and rarely involved in the generalized atherosclerotic process. Lower risk of turbulent flow. Useful for selective antegrade cerebral perfusion during arch reconstruction. prefer to use a size 22 or 24 Fr. angled cannula Femoral vessels are still commonly used for cannulation.

15
Perfusion The routine perfusion protocol for intracardiac operations is also utilized for repair of arch aneurysm. The axillary artery perfusion is begun and slowly watching for retrograde dissection and adequacy of flow.

16
Cooling and rewarming COOLING
The perfusate temperature is lowered to 10C. REWARMING. During rewarming, we never raise blood temperature above 36C. Oesophageal reaches 35C. bladder temperature of 30C or 32C.

17
Myocardial protection
Cardioplegia of the coronary ostia are readily accessible. Retrograde perfusion, or 60mEq of potassium is infused into the pump over 1 to 2 minutes just prior to circulatory arrest. Total body hypothermia supplemented with antegrade and retrograde blood cardioplegia and topical cooling on the heart for myocardial protection.

18
Spinal cord protection and prevention of paraplegia
paraplegia is not common with AA surgery More common with surgery involving the thoracic and thoracoabdominal aorta. measures to prevent paraplegia total body hypothermia, cerebrospinal fluid drainage, regional hypothermia and magnesium or corticosteroids. Somatosensory Evoked Potential (SSEP), Motor Evoked Potentials (MEPs). Monitoring is continued until the patient exits the operation room.
, Motor Evoked Potentials (MEPs). Monitoring is continued until the patient exits the operation room.")
19
Cerebral protection techniques
Hypothermic circulatory arrest (HCA) HCA protects the brain by profound inhibition of cerebral metabolism with lowering brain temperature. HCA prolonged more than 25 minutes: postoperative EEG changes are observed with neurological dysfunction as confusion, agitation or transient parkinsonism, memory deficits. High dose methylprednisolone given at 2 and 8 hours before CPB.
 HCA protects the brain by profound inhibition of cerebral metabolism with lowering brain temperature. HCA prolonged more than 25 minutes: postoperative EEG changes are observed with neurological dysfunction as confusion, agitation or transient parkinsonism, memory deficits. High dose methylprednisolone given at 2 and 8 hours before CPB.")
20
Its important Now selective hypothermic cerebral perfusion is carried out by perfusion of the innominate and left carotid arteries with blood between 6 and 12C (flow 250 to 350 ml/min) it shows good outcomes. Retrograde cerebral perfusion is also used now and it can reduce neurological insult. it can worsen neurological outcome by inducing cerebral edema, so it is not routinely used.
 it shows good outcomes. Retrograde cerebral perfusion is also used now and it can reduce neurological insult. it can worsen neurological outcome by inducing cerebral edema, so it is not routinely used.")
21
Some special techniques
Bentall procedure: Ascending aortic aneurysm extending into the underside of the aortic arch. Bentall reconstruction, in done of the aortic root with open resection of the hemi arch. Perfusion is done via the right axillary artery.

22
Postoperative care The patient is transferred to the intensive care unit mechanically ventilated. These patients require special attention for: Coagulopathy. Cardiac and cerebral complication. End organ complications. Patients should be carefully monitored. All preoperative medication restored again especially Beta-blockers. regular imaging at 6-12 months intervals. Medical therapy includes control of hypertension, B blocker are continued.

23
Thank you Dr. Eman Abou-Sief

Similar presentations


 ・ In 1998, we developed a modified elephant trunk (ET) technique using a single four-branched arch graft with a sewing “collar” and “long.>")
















