Download presentation
Presentation is loading. Please wait.

1
Moshe Phillip, M.D., Tadej Battelino, M.D., Eran Atlas, M.Sc., Olga Kordonouri, M.D., Natasa Bratina, M.D., Shahar Miller, B.Sc., Torben Biester, M.D., Magdalena Avbelj Stefanija, M.D., Ido Muller, B.Sc., Revital Nimri, M.D., and Thomas Danne, M.D N Engl J Med 2013; 368:824-833 R1 정수웅 / R3 변종규 / Prof. 우정택 1 Introduction - Prof. 우정택 History of Artificial pancreas Background - R3 변종규 Methods & Results - R1 정수웅 Discussion & Conclusion - R3 변종규

2
The goal of the artificial pancreas To improve insulin replacement therapy To avoidance of the complications of hyper-hypoglycemia To ease the burden of therapy for the insulin-dependent 2

3
Approaches Medical equipment Insulin pump Bioengineering Bio-artificial pancreas Implant bioengineered tissue containing islet cells Gene therapy DNA change of intestinal cells to become insulin-producing cells 3

4
First insulin pump in 1964 - Dr. Arnold Kadish Continuous subcutaneous insulin infusion (CSII) in 1970s First portable drug infusion pump In 1973 - Dean Kamen First marketable insulin pump in 1983 Sensor-augmented insulin pump 4
 in 1970s First portable drug infusion pump In Dean Kamen First marketable insulin pump in 1983 Sensor-augmented insulin pump 4.")
5
► First introduced in the 1960’s by a Los Angeles Physician, Dr. Arnold Kadish.

6
1974

7
First commercially available portable insulin pump called the Autosyringe “Big Blue Brick” in 1978

8
1983

9
ACCU-CHEK SPIRIT – ROCHE AMIGO – NIPRO CORPORATION DANA DIABECARE 11S – SOAIL DEVELOPMENT MINIMED PARADIGM REVEL – MEDTRONIC OMNIPOD – INSULET CORPORATION ONE TOUCH PING – ANIMAS CORPORATION

10
10

11
11

12
12 Indication for insulin pump Tx in a T1DM Continued elevated HbA1C despite MDI Continued disabling hypoglycemia despite MDI Among children, elevated HbA1C level and disabling hypoglycemia In the first trimester of pregnancy or before conception Target HbA1C levels cannot be achieved. MDI. - multiple daily insulin injections *

13
13

14
Infuses rapid-acting insulin at a slow basal rate, 24 hours a day, patient-activated insulin boosts (boluses) administered at mealtimes Improve glycemic control in patients with type 1 DM reduce the within-day and between-day glycemic variability Mean glycated hemoglobin levels are significantly lower about 0.3 to 0.6% between treatments accompanied by a 10 to 20% reduction in the dose of insulin Severe hypoglycemia was significantly lower than MDI (rate ratio, 4.19; 95% CI, 2.86 to 6.13) 14
 administered at mealtimes Improve glycemic control in patients with type 1 DM reduce the within-day and between-day glycemic variability Mean glycated hemoglobin levels are significantly lower about 0.3 to 0.6% between treatments accompanied by a 10 to 20% reduction in the dose of insulin Severe hypoglycemia was significantly lower than MDI (rate ratio, 4.19; 95% CI, 2.86 to 6.13) 14")
15
15

16
16

17
17

18
18

19
Full closed-loop system insulin is administered according to the glucose readings in a fully automated manner Includes the patient's physical characteristics, insulin delivery regimen, insulin pharmacodynamic parameters Insulin pump can communicate in real time with a personal computer, conducted using the Artificial Pancreas Software (APS) MDLAP system is a promising tool for individualized glucose control of patients with type 1 diabetes 19
 MDLAP system is a promising tool for individualized glucose control of patients with type 1 diabetes 19")
20
20

21
Intensive insulin therapy is considered to be the standard treatment for type 1 diabetes Insulin pumps, glucose sensors, or a combination of the two devices (sensor- augmented pump) However, the risk of hypoglycemia is still present with the use of all currently available therapies. Maintenance of nocturnal euglycemia is extremely important and is challenging, since most cases of severe hypoglycemia occur at night. 75% of total hypoglycemic seizures in children and 6% of deaths in patients under the age of 40 years who have type 1 diabetes. 21

22
Fully automated artificial-pancreas systems have been suggested as a means to control nocturnal glucose levels. Such systems can improve glucose control and reduce the risk of nocturnal hypoglycemia in hospital setting Diabetes Wireless Artificial Pancreas Consortium (DREAM) was established to test the MD-Logic Artificial Pancreas system in settings outside the hospital under real-life conditions. The objective of the study was to evaluate the safety and efficacy of the artificial-pancreas system in young persons with type 1 diabetes, in a youth- camp setting. 22
 was established to test the MD-Logic Artificial Pancreas system in settings outside the hospital under real-life conditions. The objective of the study was to evaluate the safety and efficacy of the artificial-pancreas system in young persons with type 1 diabetes, in a youth- camp setting. 22.")
23
23

24
24

25
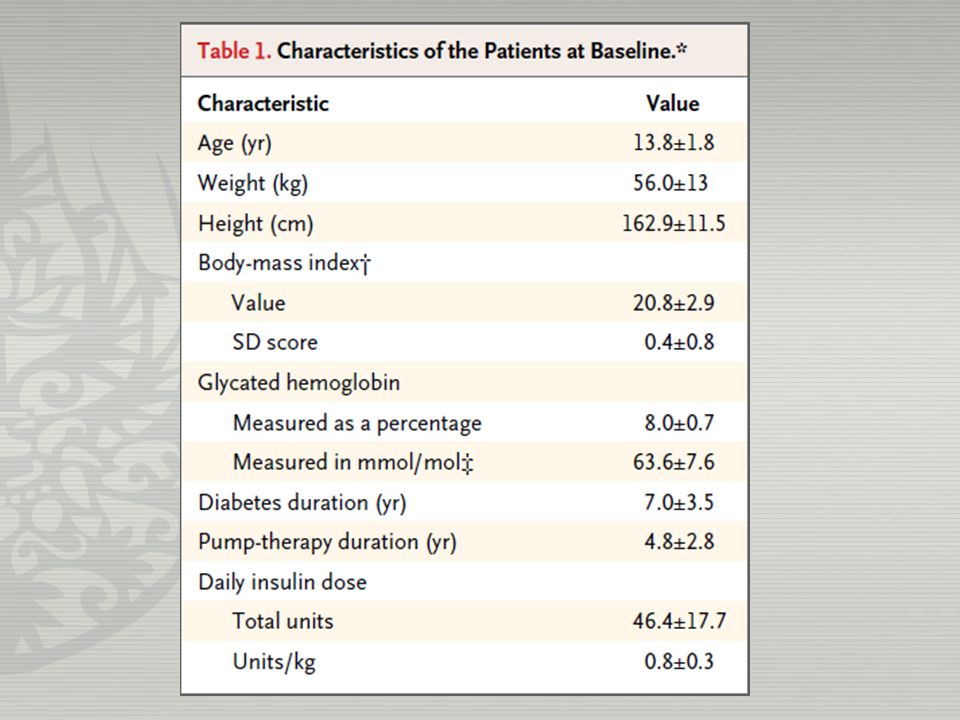
Study participants 10 to 18 years of age at least a 1 year history of type 1 diabetes insulin pump therapy for at least 3 months A glycated hemoglobin level of 7 and 10 % A body mass index below the 97 th percentile for the patient’s age 25

26
Main exclusion criteria A concomitant disease Participation in another study Pregnancy A history of diabetic ketoacidosis or severe hypoglycemia within the past month 26

27
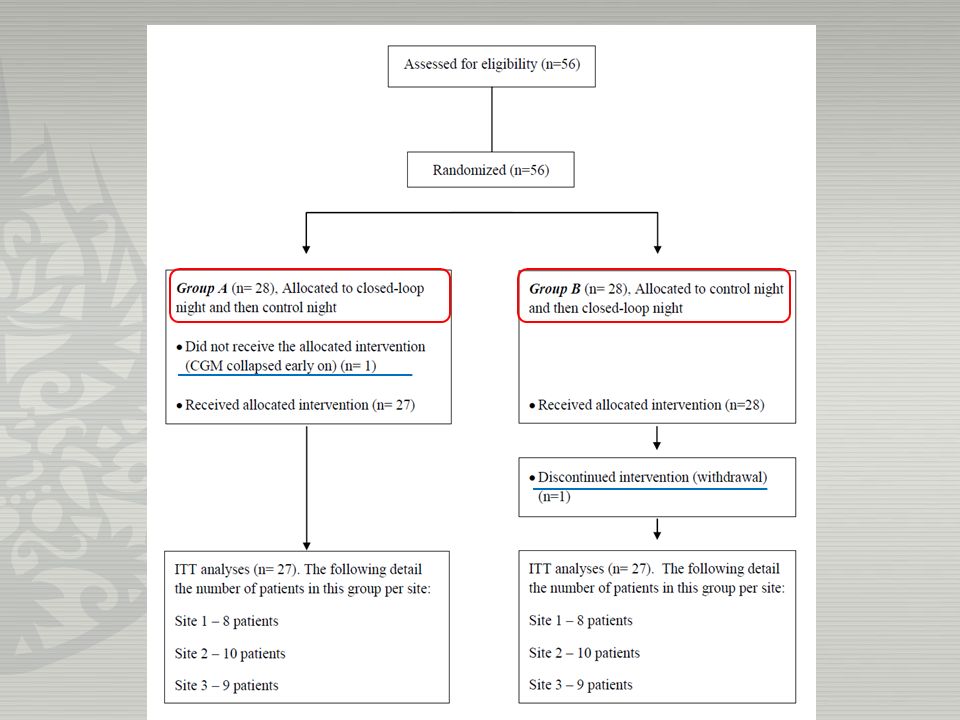
artificial pancreas sensor-augmented insulin pump artificial pancreas Group A Group B 1 st night 2 nd night

28
28

29
29 The first trial with Artificial Pancreas at diabetes camp

30
Primary end point Total number of episodes of glucose levels < 63mg/dL Time that glucose level was < 60mg/dL Overnight glucose level 30

31
Secondary end point overnight glucose control overnight glucose variability 31

32
32

35
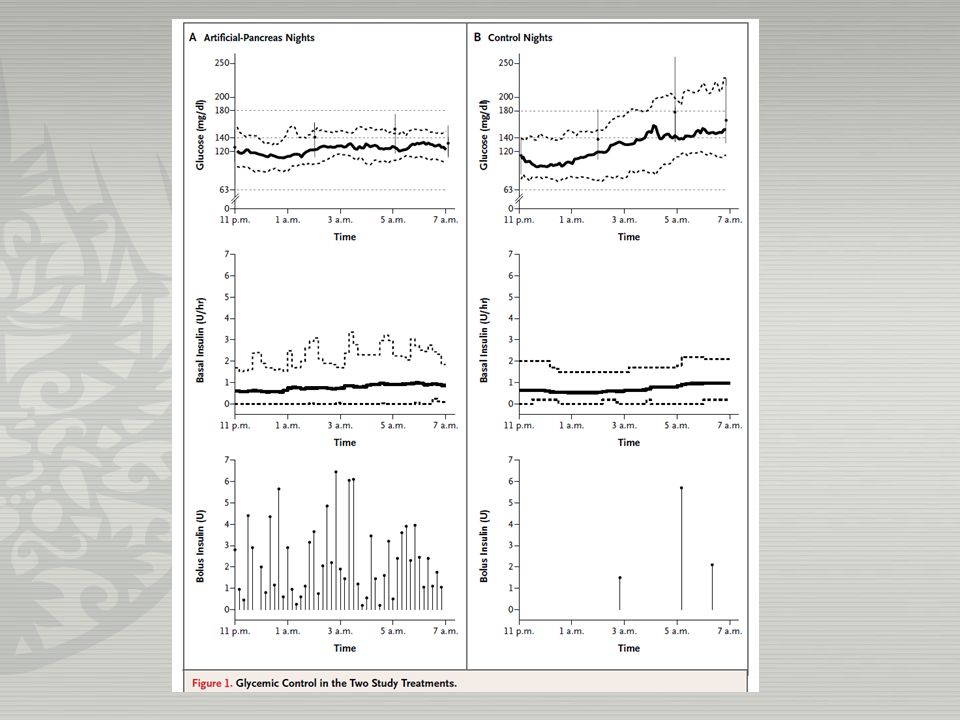
P value = 0.02 P value = 0.003 No significance

36
36

37
37

39
The MD-Logic Artificial Pancreas system reduced risk of hypoglycemia in young persons at an overnight camp. The combined effect of amount of insulin provided, timing of insulin delivery, the presence of an alarm module The early-alert system for the artificial pancreas 39

40
Each treatment was evaluated in a one-night session, may be different in a multinight design Crossover studies have an intrinsic limitation, since the order in which treatments are administered may affect the outcome Glucose-level data were based on sensor readings Every 3 hours, the assigned medical personnel evaluated capillary blood glucose levels. 40

41
The use of an artificial-pancreas system resulted in less hypoglycemia and tighter control of nocturnal glucose levels than did a sensor-augmented pump system in a youth-camp setting. 41

Similar presentations



>")















