Download presentation
Presentation is loading. Please wait.

1
CLINICAL ASPECT OF GRADING AND STAGING Hanggoro Tri Rinonce, MD, PhD Department of Anatomical Pathology Faculty of Medicine, Gadjah Mada University

2
INTRODUCTION Methods to quantify the probable clinical aggressiveness of a given neoplasm and its apparent extent and spread in the individual patient are necessary – Making an accurate prognosis – Comparing end results of various treatment protocols.

3
GRADING The grading of a cancer attempts to establish some estimate of its aggressiveness or level of malignancy based on the cytologic differentiation of tumor cells and the number of mitoses within the tumor. The cancer may be classified as grade I, II, III, or IV, in order of increasing anaplasia. Criteria for the individual grades vary with each form of neoplasia and are not detailed here. Difficulties in establishing clear-cut criteria have led in some instances to descriptive characterizations (e.g., “well- differentiated adenocarcinoma with no evidence of vascular or lymphatic invasion” or “highly anaplastic sarcoma with extensive vascular invasion”).
..")
4
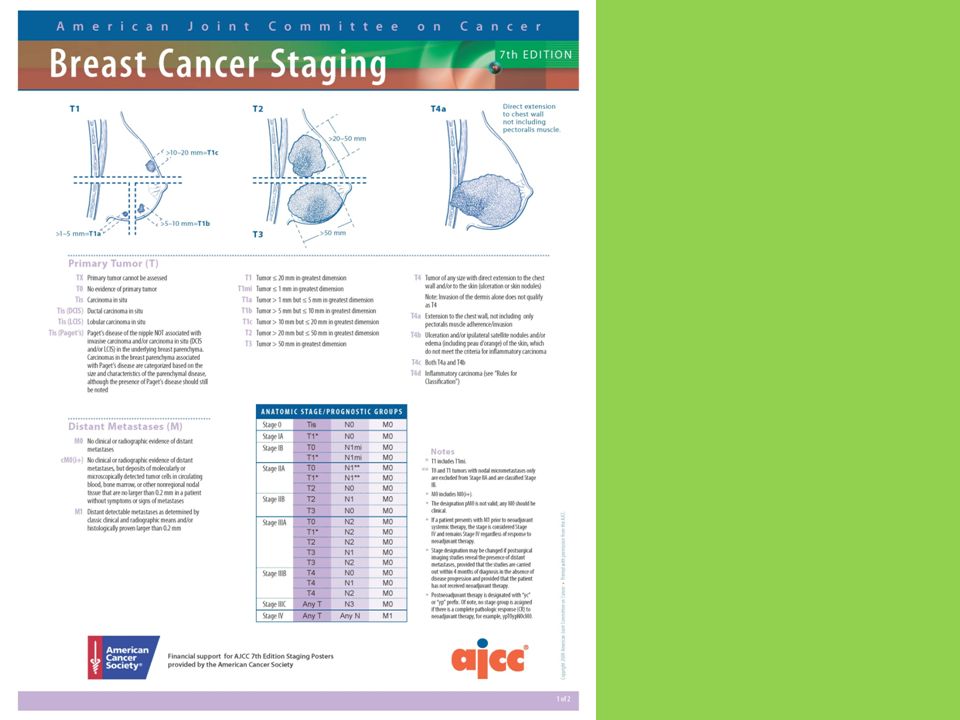
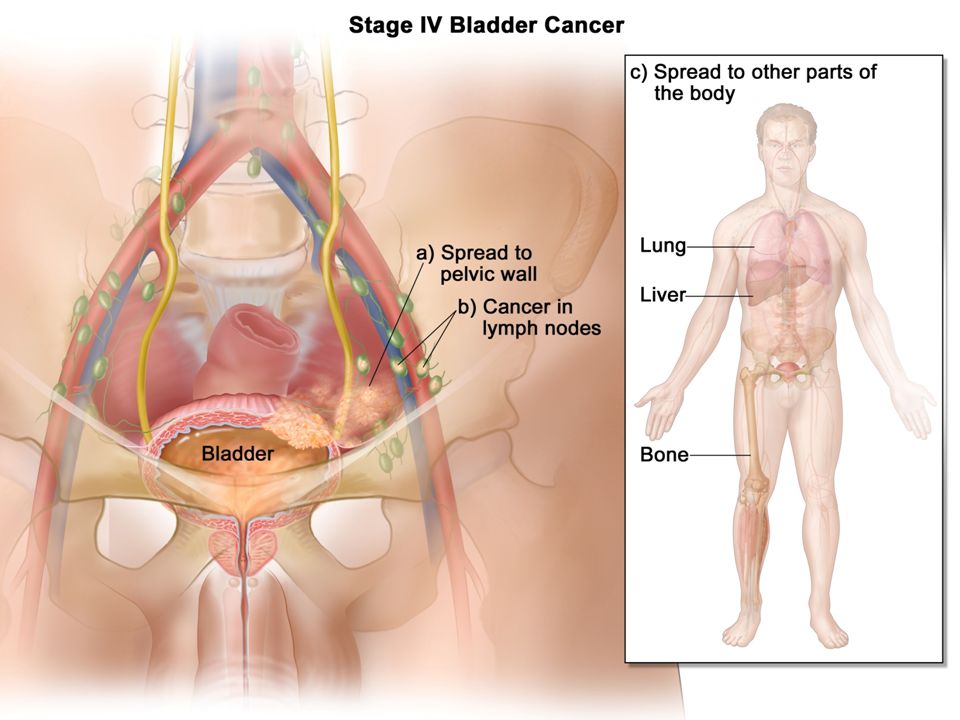
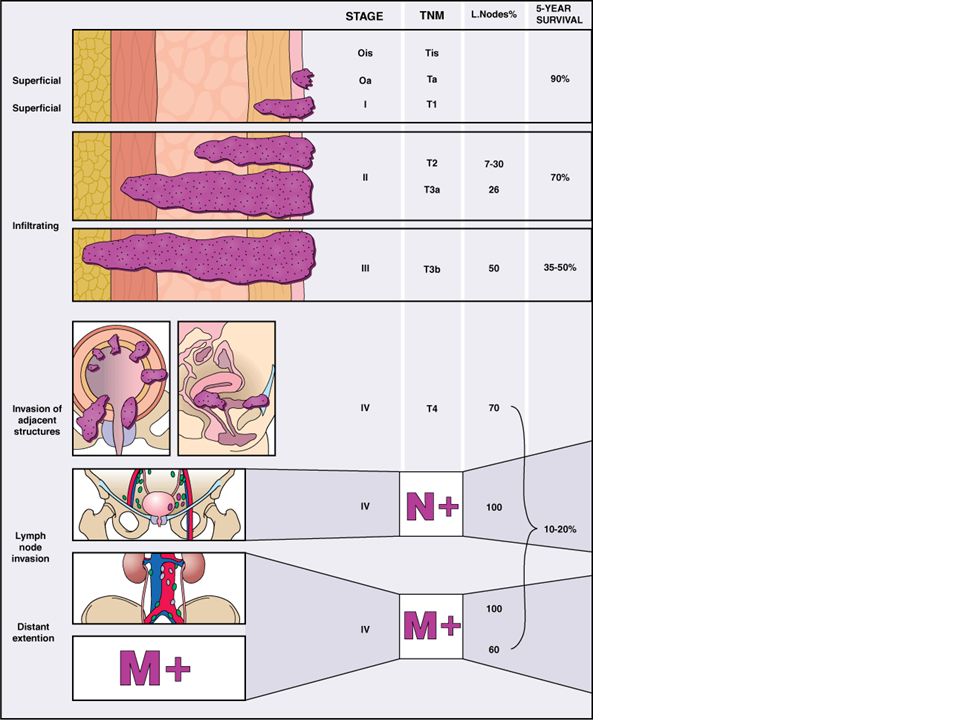
STAGING Staging of cancers is based on – size of the primary lesion – its extent of spread to regional lymph nodes – presence or absence of metastases This assessment usually is based on clinical and radiographic examination (computed tomography and magnetic resonance imaging) and in some cases surgical exploration. Two methods of staging – TNM system (T, primary tumor; N, regional lymph node involvement; M, metastases) – AJC (American Joint Committee) system. TNM system – T1, T2, T3, and T4 increasing size of the primary lesion; – N0, N1, N2, and N3 progressively advancing node involvement – M0 and M1 absence and presence of distant metastases. AJC method – divided into stages 0 to IV incorporating the size of primary lesions and the presence of nodal spread and of distant metastases. When compared with grading, staging has proved to be of greater clinical value.
 – AJC (American Joint Committee) system. TNM system – T1, T2, T3, and T4 increasing size of the primary lesion; – N0, N1, N2, and N3 progressively advancing node involvement – M0 and M1 absence and presence of distant metastases. AJC method – divided into stages 0 to IV incorporating the size of primary lesions and the presence of nodal spread and of distant metastases. When compared with grading, staging has proved to be of greater clinical value..")
5
Grading of Adenocarcinoma, NOS

6
Grading of Squamous Cell Carcinoma, NOS

7
Elston Grading of Infiltrating Breast Cancer

9
Grading of Phyllodes Tumor

10
Gleason Grading of Prostate Cancer

11
Fuhrman Nuclear Grading of Renal Cell Carcinoma

12
Staging Overview and Five-Year Survival Rates for Renal Cancer (Cohen et al, 2005, N Engl J Med 353;23)
")
13
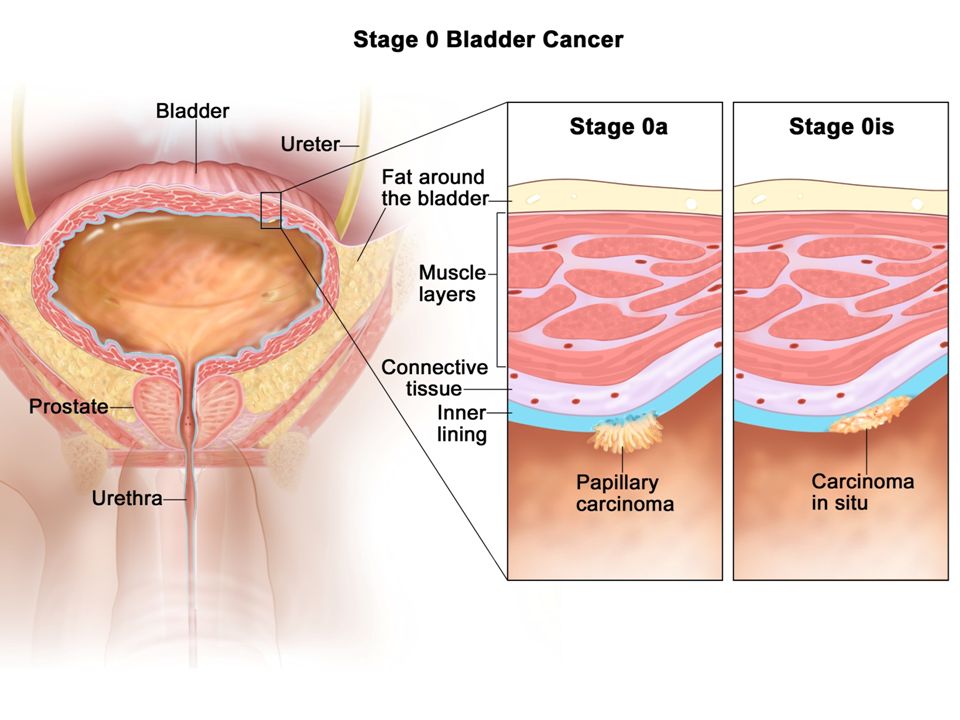
The WHO/ISUP Consensus Classification of Non- invasive (In Situ) Papillary Urothelial Neoplasms
 Papillary Urothelial Neoplasms")
20
Terima kasih

Similar presentations







>")


 tumor and whether.>")









