Download presentation
Presentation is loading. Please wait.

1
Brandon Haynes Seattle Children’s Hospital May 17, 2012

2
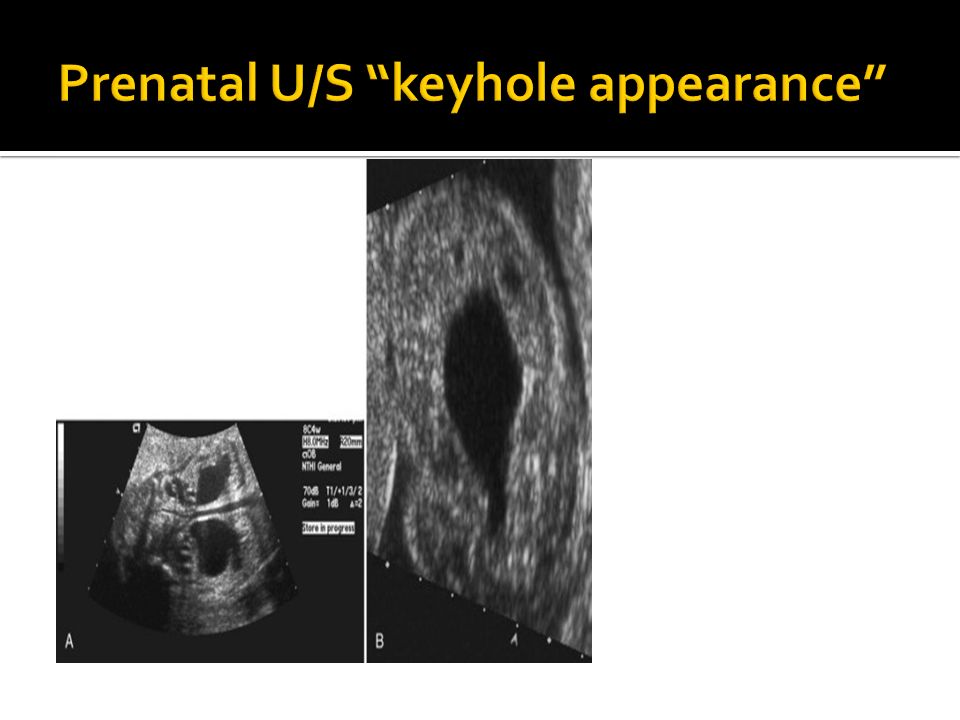
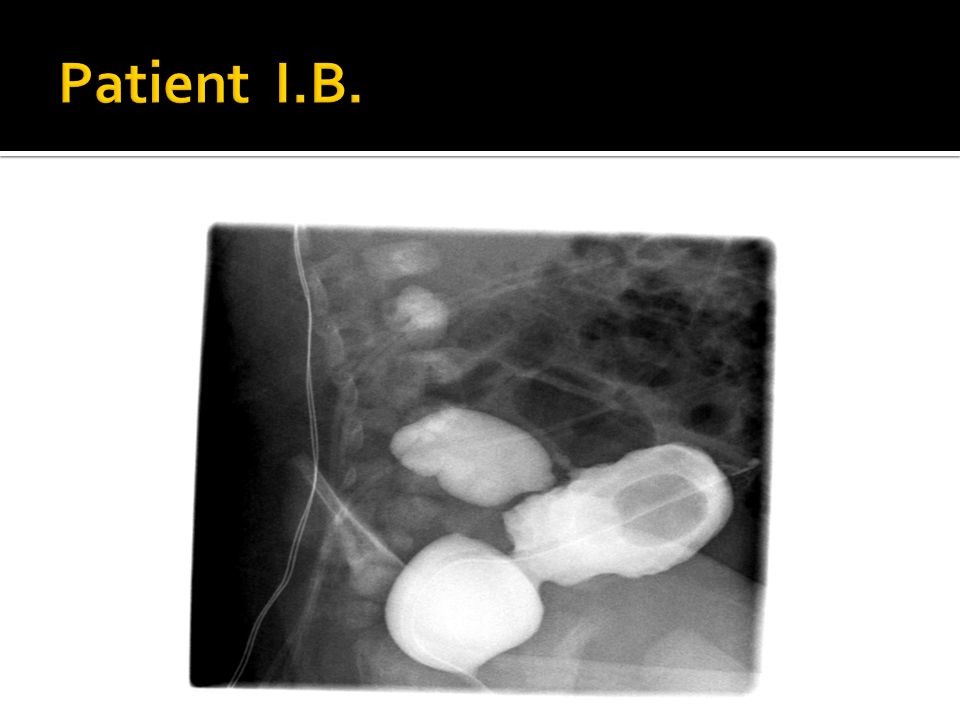
Prenatal U/S showed distended bladder, bilateral ureterohydronephrosis, oligohydramnios, and concern for pulmonary hypoplasia Admitted to NICU with respiratory distress at birth Day of Life #1 Cr 1.7 VCUG and renal U/S performed on DOL #2 confirming diagnosis of posterior urethral valve Day of life #6 peritoneal dialysis catheter placement by Dr. Riehle Cr 7.1 at time of surgery

5
Obstructing membranous folds within the lumen of the posterior urethra Most common etiology of urinary tract obstruction in the newborn male Most common cause of chronic renal disease due to urinary tract obstruction in children 1:5000 – 8000 male births

6
Obstructing membranous folds within the lumen of the posterior urethra Most common etiology of urinary tract obstruction in the newborn male Most common cause of chronic renal disease due to urinary tract obstruction in children 1:5000 – 8000 male births

7
Most detected antenatally via ultrasound Bilateral hydronephrosis Distended and thickened bladder (> 3mm) Dilated posterior urethra Oligohydramnios Renal dysplasia increased echogenicity and cortical cysts Urinary ascites or perinephric urinoma
 Dilated posterior urethra Oligohydramnios Renal dysplasia increased echogenicity and cortical cysts Urinary ascites or perinephric urinoma")
8
Neonates: - respiratory distress due to lung hypoplasia - abdominal distention - Difficulty voiding - Poor urinary stream Infants: Failure to thrive Urosepsis Poor urinary stream Straining while voiding Older Boys: Urinary tract infections Enuresis Frequency straining during voiding poor urinary stream large volume voids

9
Goal is to prevent or lessen the sequelae: Chronic Kidney Disease Renal dysplasia seen in up to 60% of infants 15-20% progress to ESRD Vesicoureteral Reflex Disease Present in about 50% of cases Bladder dysfunction obstruction causes hypertrophy, collagen deposition, poor compliance and uninhibited contractions

10
Bladder decompression Remove obstruction Optimize renal function Treat/ Prevent infection Bladder rehabilitation

11
Perform catheter drainage even if diagnosis isn’t confirmed Use pediatric feeding tube in small neonates confirm accurate placement with imaging

12
- goal is to incise and disrupt integrity, not to remove - performed endoscopically or open using bugbee electrode or resectoscope with hook or cold knife

13
- temporary measure for very small or very ill infants - allows for valve incision/ablation at later date - allows for “bladder cycling”

14
-initial management in the past -provides quick upper tract decompression and control of infection -difficult urinary reconstructive problems later -prevents bladder cycling -reserved for cases of failed bladder drainage

15
Renal insufficiency is caused in utero and is largely permanent No difference in renal function following initial ablation vs. upper tract diversion The bladder is capable of rehabilitation after obstruction is relieved

16
Michael Mitchell, MD of UW Pediatric Urology coined term “valve bladder” Observed a series of 23 boys treated with initial valve ablation 85% had significant reduction of bladder trabeculation within one year better success with potty-training during follow-up vs. upper tract diversion His conclusion : Bladder healing is dependent on bladder filling and emptying (cycling) with low outflow resistance. Maximum recovery of renal function will depend on preventing the development of a hostile bladder. Early valve ablation may best achieve both goals of maximum bladder and renal functional recovery.
 with low outflow resistance. Maximum recovery of renal function will depend on preventing the development of a hostile bladder. Early valve ablation may best achieve both goals of maximum bladder and renal functional recovery..")
17
2000 Univ. of Toronto retrospective review 50 consecutive patients divided into 3 groups Group 1: normal renal function and radiologically normal upper tracts, 22 patients Group 2: normal renal function with hydronephrosis and/or reflux, 13 patients Group 3: azotemia with hydronephrosis or reflux, 15 patients

18
Group 1: normal renal function and no evidence of upper tract deterioration after valve ablation at average 32 month F/U Group 2: saw resolution of radiologic abnormalities (hydronephrosis, reflux) in 50% of cases at average 28 month F/U. Group 3: 7 valve ablation vs. 8 urinary diversion* Renal function was normal 6/7 who underwent valve ablation and 3/8 renal function who underwent urinary diversion. Radiologically, the severity of the hydronephrosis and reflux was decreased after valve ablation but not in the diverted group. * performed in patients with renal deterioration and severe hydronephrosis and/or high-grade reflux CONCLUSIONS: “Valve ablation is the mainstay of treatment for patients with posterior urethral valves. Prenatal and postnatal factors, such as renal dysplasia and urinary tract infection, respectively, rather than the posterior valve treatment dictate the long-term renal and radiologic outcomes.”

19
Prenatal intervention vesicoamniotic shunt to prevent lung hypoplasia and reduce back pressure Risk of fetal and maternal morbidity without proven benefit for long-term renal outcome Consider if high risk of in utero/neonatal death due to midtrimester severe oligohydramnios and evidence of good renal function based on fetal urinary evaluation

20
Immediate catheter drainage if PUV is suspected Primary valve ablation is the preferred initial surgical approach Vesicostomy if patient is too small or ill, as a temporary measure Initial management of reflux is valve ablation with observation and antibiotic prophylaxis Bladder and renal function often remain unstable after relief of obstruction so lifelong monitoring is required.

Similar presentations













 Incidence: 1:188 Approximately 50% of antenatal scans are normal postnatally Posterior urethral.>")





