Download presentation
Presentation is loading. Please wait.

1
HIGH FREQUENCY OSCILLATORY VENTILATION
Michael Gordon

2
What is HFOV? A ventilator that delivers more than 150 breaths per minute Delivers a small tidal volume, usually less than or equal to anatomical dead space Uses diaphragm (acoustic speaker) to produce oscillatory gas flows within the airway Active inspiratory and expiratory phase
 to produce oscillatory gas flows within the airway. Active inspiratory and expiratory phase.")
3
Types of high frequency ventilation
High Frequency Positive Pressure Ventilation – conventional ventilation at fast rates, not a true HFV. Conventional ventilation provides rates of 1 – 120 and volumes of 4 – 20ml/kg High Frequency Oscillatory Ventilation – delivers rates of 120 – 1200, with volumes equivalent to or less than anatomical dead space (0.1 – 2 ml/kg). Has active inspiration and expiration.
. Has active inspiration and expiration.")
4
Terminology Dead space –the air in the nose, mouth, larynx, trachea, bronchi and bronchioles. Frequency – measure in Hertz (Hz), 1 Hz = 1 cycle/sec = 60 bpm Mean Airway Pressure – continuous distending pressure (cmH2O) Oscillation Amplitude - peak to trough of pressure waveform = delta P (cmH2O). This is the measure of pressure the ventilator uses to push air into the circuit.
, 1 Hz = 1 cycle/sec = 60 bpm. Mean Airway Pressure – continuous distending pressure (cmH2O) Oscillation Amplitude - peak to trough of pressure waveform = delta P (cmH2O). This is the measure of pressure the ventilator uses to push air into the circuit.")
5
History high frequency ventilation
In Henderson et al found that panting dogs maintained an adequate gas exchange with tidal volumes less than anatomical dead space. In 1964 it was recognised that low frequency, high tidal volume (>15ml/kg) caused lung injury. Low frequency, high tidal volumes could cause loss of surfactant activity and decreased compliance in otherwise normal lungs. Barotrauma (pressures) and Volutrauma (volumes) implicated in lung damage as well. In 1994 Clark found that large tidal volumes caused more lung damage than high airway pressure. Volutrauma causes - epithelial and endothelial cell injury, pulmonary oedema, surfactant dysfunction, decreased compliance, hyaline membrane formation and impaired gas exchange Therefore High Frequency Ventilation
 caused lung injury. Low frequency, high tidal volumes could cause loss of surfactant activity and decreased compliance in otherwise normal lungs. Barotrauma (pressures) and Volutrauma (volumes) implicated in lung damage as well. In 1994 Clark found that large tidal volumes caused more lung damage than high airway pressure. Volutrauma causes - epithelial and endothelial cell injury, pulmonary oedema, surfactant dysfunction, decreased compliance, hyaline membrane formation and impaired gas exchange. Therefore High Frequency Ventilation.")
6
Method of gas transport
It is thought that gas transport in HFOV is accomplished by the following methods. Direct Alveolar ventilation Pendulluft effect Convective streaming Augmented (Taylor) dispersion Cardiogenic mixing Molecular diffusion
 dispersion. Cardiogenic mixing. Molecular diffusion.")
7
Direct alveolar ventilation
Small part of proximal alveoli is ventilated directly. Gaseous exchange takes place the same as in CMV.

8
Pendulluft effect Neighbouring alveoli with different time constraints (different compliance and resistance) are ventilated out of phase, filling and emptying at different rates. Due to this asynchrony these alveoli can mutually exchange gas. By this mechanism even very small fresh gas can reach large numbers of alveoli and regions.
 are ventilated out of phase, filling and emptying at different rates. Due to this asynchrony these alveoli can mutually exchange gas. By this mechanism even very small fresh gas can reach large numbers of alveoli and regions.")
9
Convective streaming Describes lateral transport of gas in the airways. Gas flows through a tube in layers which travel at different velocity. Velocity of each layer increases towards centre of tube Particles at outer edge of tube are more effected by viscious resistance and travel at slower velocities Assymetric velocity profiles cause bidirectional flow of gas to and from peripheral airways

10
Augmented (Taylor) dispersion
Describe radial transport of gases due to turbulence A plane boundary surface between two gases develops into a pike shaped profile as the velocity of one of the gases increases. Gases exchange occurs at the boundry surface through lateral diffusion(pic)
")
11
Augmented (Taylor) dispersion
The amount of gas transport depends on the effective longitudinal diffusivity, and is inversely proportional to molecular diffusivity. At airways bends or bifurcations secondary gas movements occur. (pic)
")
12
Cardiogenic mixing The heart is a natural oscillator

13
Molecular diffusion Passive movement of molecules along a concentration gradient due to random thermal oscillation of molecules Diffusion across membrane

14
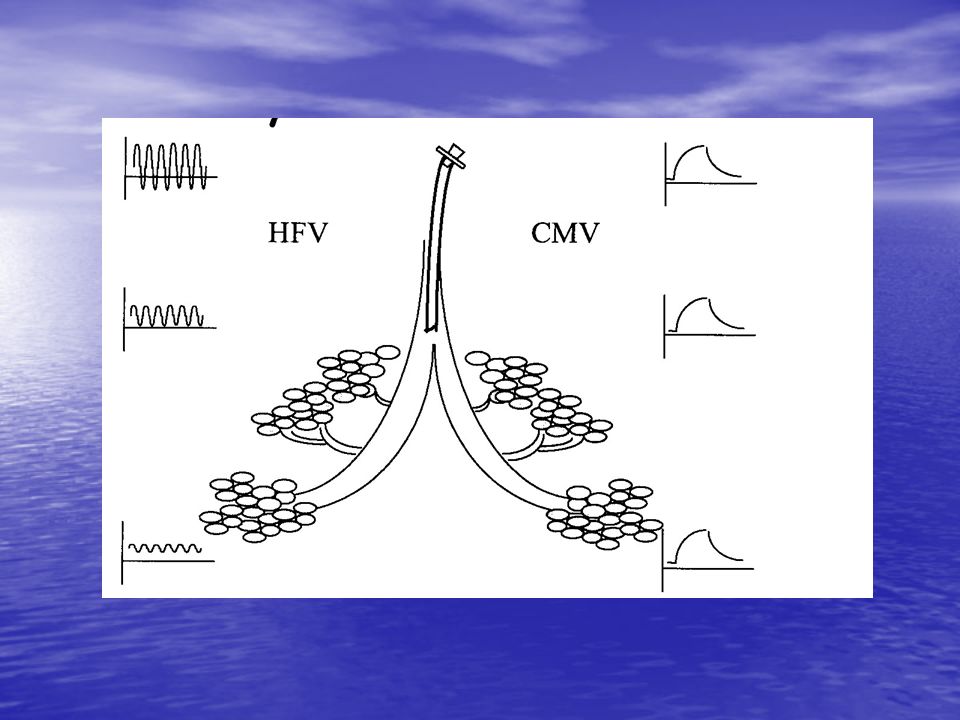
HFOV vs CMV waveform

15
HFOV Waveform

16
During HFV only approximately 10% of the delta P delivered at the patient wye is transmitted to the alveoli and terminal bronchioles. During CMV >90% of the PIP delivered at the patient wye is transmitted to the alveoli and terminal bronchioles. During HFV alveoli are kept open and not subjected to large pressure and volume swings in order to maintain gas transfer. During CMV alveoli close and open on every breath, large pressure swings are required to move large volumes (in comparison to HFV) to maintain gas transfer.
 to maintain gas transfer.")
18
HFOV Oxygenation and CO2 removal
Controlled by – optimal MAP that promotes lung recruitment and FiO2 CO2 removal Controlled by – increasing Delta P (which increases tidal volumes) and decreasing frequency which increases tidal volumes A lower frequency results in larger tidal volumes also because there is diminished effect of flow dependant ETT resistance, and there is increased time available for flow.
 and decreasing frequency which increases tidal volumes. A lower frequency results in larger tidal volumes also because there is diminished effect of flow dependant ETT resistance, and there is increased time available for flow.")
19
Optimal ventilation strategy
From all this an optimal ventilation strategy was developed. This entailed the following limited FiO2 small tidal volumes minimal PIP high Frequency sufficient PEEP to proximate normal functional residual capacity (FRC)
")
20
Optimal ventilation strategy
Critical opening point/critical closing point The problem is determining WHEN you are at this point.

21
Indications for HFOV Neonatal Respiratory Distress Syndrome
Persistent Pulmonary Hypertension of the Newborn (PPHN) Neonatal Meconium Aspiration Syndrome Congenital Diaphragmatic Hernia Neonatal Air Leak Syndrome with PIE Pneumonia Pulmonary Haemorrhage Lung Hypoplasia
 Neonatal Meconium Aspiration Syndrome. Congenital Diaphragmatic Hernia. Neonatal Air Leak Syndrome with PIE. Pneumonia. Pulmonary Haemorrhage. Lung Hypoplasia.")
22
Advantages of HFOV over CMV
Does not cause large alveolar pressure and volume swings to produce adequate gas exchange May reduce haemodynamic effects of ventilation – depends on MAP Produces more uniform lung inflation and normalises lung structure Lung recruitment on HFV allows more uniform dispersal of surfactant and Nitric Oxide May reduce lung inflammatory response Patients can breath as if on CPAP

23
Advantages of HFOV over ECMO
Less invasive, does not require anticoagulants Less expensive, can be used in non ECMO centres Can be used as a bridge to ECMO when CMV has failed Can be used on newborns <2kg ECMO centres now using HFOV report 30 – 50% decrease in need for ECMO to treat respiratory failure Easier to transport on HFV than ECMO ( HFJV runs on batteries)
")
25
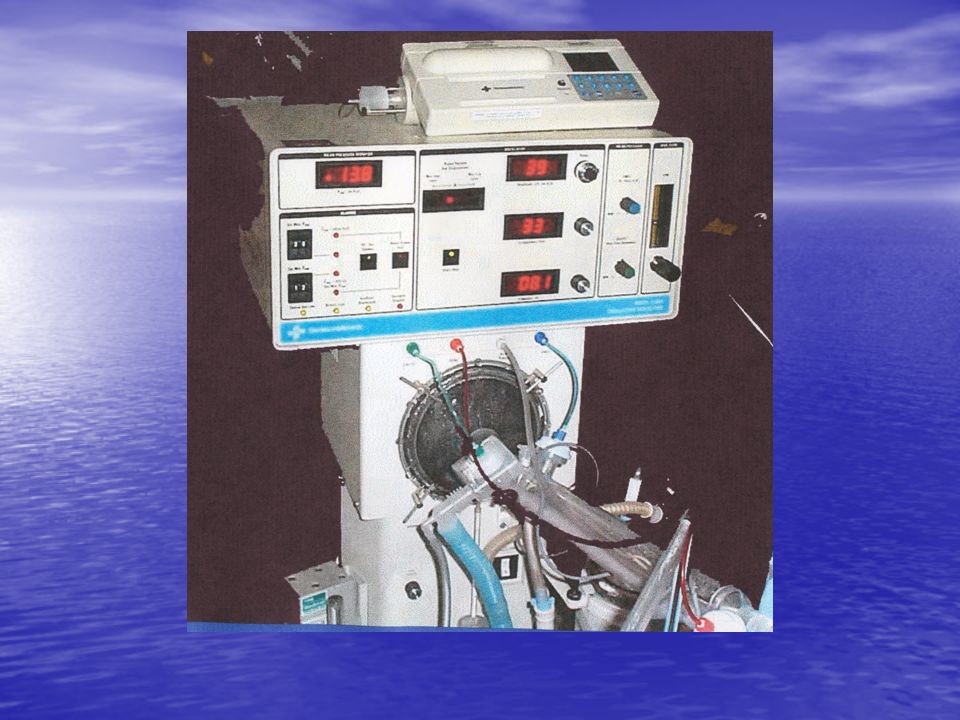
Sensormedics 3100A Type – electromagnetic flow generator
Specifications – Paw range 3-45 cm H20 Weight range - up to 35kg Amplitude 0-90 cm H20 Frequency range 5-15 Hz I:E ratio adjustable between 1:2:3 and 1:1 (30% and 50%) Sigh breaths - no
 Sigh breaths - no.")
26
MAP - PEEP ΔP (amplitude) Frequency inflate alveoli oxygenation
- distance piston travels - shake alveoli - chest wiggle - pressure above and below MAP - ↑ ΔP = ↑ tidal volume = ↑ CO2 removal Frequency - 1kHz = 60bpm - speed of piston - ↓ frequency = ↑ tidal volume = ↑ CO2 removal

28
Babylog 8000plus Type – oscillating expiratory valve with venturi assisted expiration Specifications Paw range 3-30cm H20 Weight range – up to 4kg (but realistically 2 kg) Amplitude arbitrary scale 0 – 100% (100% amplitude = 60 Paw) Frequency range 5-20cm Hz I:E ratio – automatically adjusted between 1:5 and 1:1 Sigh breaths- yes
 Amplitude arbitrary scale 0 – 100% (100% amplitude = 60 Paw) Frequency range 5-20cm Hz. I:E ratio – automatically adjusted between 1:5 and 1:1. Sigh breaths- yes.")
29
Frequency - ↓ frequency = ↑ tidal volume = ↑ CO2 removal
MAP - PEEP - inflate alveoli - oxygenation Frequency - ↓ frequency = ↑ tidal volume = ↑ CO2 removal - (changing freq. has more effect on tidal volume) - (numbers ≤ 10 are better because better flow rates) ΔP (amplitude) - relative scale 0-100% (0% = MAP) - % of difference of 60 minus the MAP - shake alveoli - chest wiggle - pressure above and below MAP - ↑ ΔP = ↑ tidal volume = ↑ CO2 removal - (amplitude ≥ 60% has little effect on tidal volume) DCO2 - gas transport coefficient - represents CO2 likely to be removed - VT2 x f - ↑ DCO2 = ↑ CO2 removal
 - (numbers ≤ 10 are better because better flow rates) ΔP (amplitude) - relative scale 0-100% (0% = MAP) - % of difference of 60 minus the MAP. - shake alveoli. - chest wiggle. - pressure above and below MAP. - ↑ ΔP = ↑ tidal volume = ↑ CO2 removal. - (amplitude ≥ 60% has little effect on tidal volume) DCO2 - gas transport coefficient. - represents CO2 likely to be removed. - VT2 x f. - ↑ DCO2 = ↑ CO2 removal.")
30
Set Up Sensormedics - Practical Points
Space in the unit and around the bedside Care with hoses and power cords Always ensure brakes are applied Refer to policy and procedures (9W )
")
31
Set Up Drager – Practical Points
Appropriate tubing (non disposable) Care with power cords
 Care with power cords.")
32
Prior to use adjust settings for patient (off patient)
- as ordered by medical officer: Set the ordered bias flow (usually remains set at 25 LPM (centre of ball)). Set the ordered frequency (Hz). Inspiratory time to remain set at 33%. Set the mean pressure limit: return the MEAN PRESSURE ADJUST control knob to maximum then rotate the MEAN PRESSURE LIMIT knob anti-clockwise until the Paw reading is 10cm above the ordered (treatment) MAP.
). Set the ordered frequency (Hz). Inspiratory time to remain set at 33%. Set the mean pressure limit: return the MEAN PRESSURE ADJUST control knob to maximum. then rotate the MEAN PRESSURE LIMIT knob anti-clockwise until the Paw reading is 10cm above the ordered (treatment) MAP.")
33
Going onto HFOV Set the MAP 2 – 4 cmH2O over the Map on the CMV
Set the amplitude to see a “wiggle” from the nipple line to the umbilicus Set the Hertz to an appropriate rate Set the FiO2 according to CMV FiO2 Ensure appropriate alarm limits set Obtain a chest X-ray Ensure the rib expansion on x-ray is 8 –9 ribs Obtain frequent arterial blood gases to monitor progress

34
Nursing Considerations
Observations - How are they different to CMV? Respiratory assessment Cardiac monitoring ?pneumothorax Care of the ETT Positioning, pressure care Parent – caretaker interactions

35
Potential complications
Hypotension due to impaired cardiac function IVH Lung over distension and Air Leak Syndrome Unplanned extubation

36
Potential operating issues
Alarm settings High and low Paw must be set appropriately Problems? If set to close to operating Paw and patient is spontaneously breathing the oscillator alarms are triggered frequently If alarms set to far from operating Paw circuit may not pressurise and re-start after disconnection

37
Potential operating issues
Unable to decrease Paw as oscillator being weaned Paw is bias flow dependent – set as 25l/min at NICU RWH, therefore may be to high as Paw being weaned Solution – reduce bias flow

38
Potential operating issues
Unable to increase Paw when oscillator in use Check Paw LIMIT knob not set too low

39
Potential operating issues
Unable to calibrate circuit mean pressure 39-43cm Check length of circuit for air leaks Ensure water trap T piece is turned off Ensure all balloon diaphragms are fitted snuggly and not punctured Check temperature probe site for snug fit Increase biasis flow*

Similar presentations