Download presentation
Presentation is loading. Please wait.

1
Tuesday August 23, 2011 Nancy L Jones, MD

2
Normal substance produced at normal or increased rate with inadequate removal Normal or abnormal endogenous substance in face of genetic or acquired defect in folding, packaging, transport or secretion Inherited defect in an enzyme leading to failure to degrade a metabolite Abnormal exogenous substance deposited and accumulates in cell that lacks ability to degrade or transport the substance

3
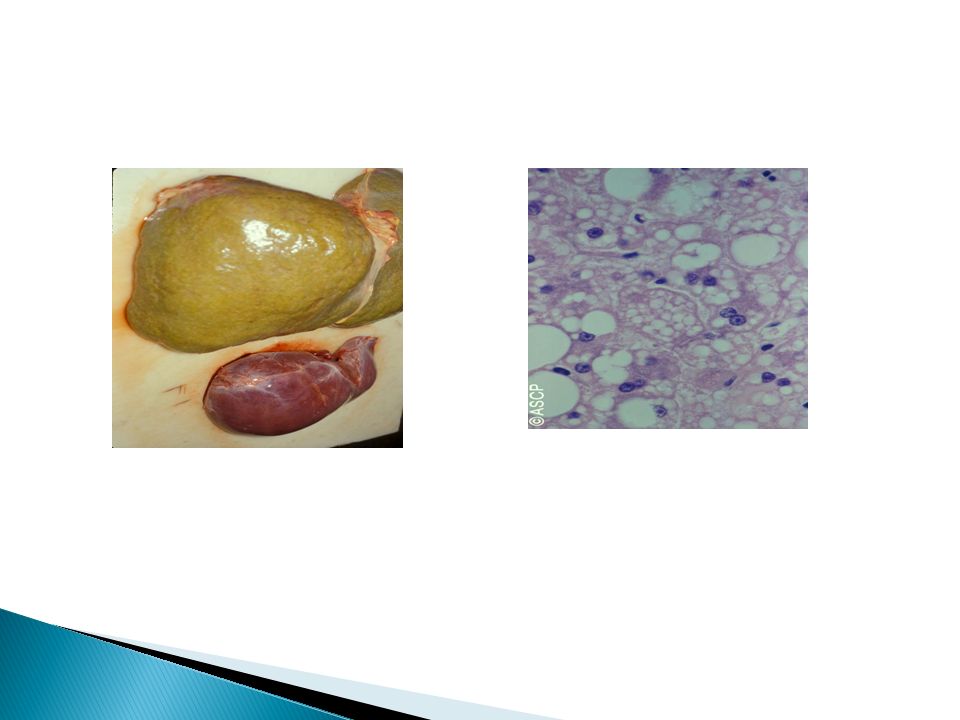
Fatty change of the liver ◦ Accumulation of triglycerides within hepatocytes, myocytes, skeletal muscle, kidney and other organs ◦ Steatosis ◦ Caused by toxins, protein malnutrition, DM, obesity and anoxia. ◦ Ethanol and obesity most common causes

4
Free fatty acids go into liver cells from adipose tissue or ingested food ◦ Esterified to triglycerides ◦ Converted to cholesterol or phospholipids ◦ Oxidized to ketone bodies ◦ Fatty acids may be synthesized from acetate within liver cell

5
Triglycerides complex with apoproteins to form lipoproteins to get out into circulation ◦ Defects: Hepatotoxins alter mitochondrial and SER function and inhibit oxidation CCL 4 and protein malnutrition decrease synthesis of apoproteins Anoxia inhibits oxidation Starvation increases fatty acid mobilization

6
Significance dependent on cause and severity ◦ Mild no effect on cell function ◦ Severe may transiently impair cell function ◦ Irreversible impairment may be caused by exposure to CCL 4 ◦ Most fatty change to liver is reversible ◦ May progress to cell death or represent early lesion of nonalcoholic steatohepatitis

8
Cellular cholesterol metabolism tightly regulated for normal cell membrane synthesis Phagocytes may accumulate more lipids than they can metabolize in some disease states ◦ Foam cells result of membrane-bound vacuoles from debris of necrotic cells or abnormal oxidized forms of lipoproteins ◦ Atherosclerosis result of smooth muscle cell and macrophage filling with lipid vacuoles containing cholesterol and cholesterol esters which impart yellow color and contribute to pathogenesis of lesion

9
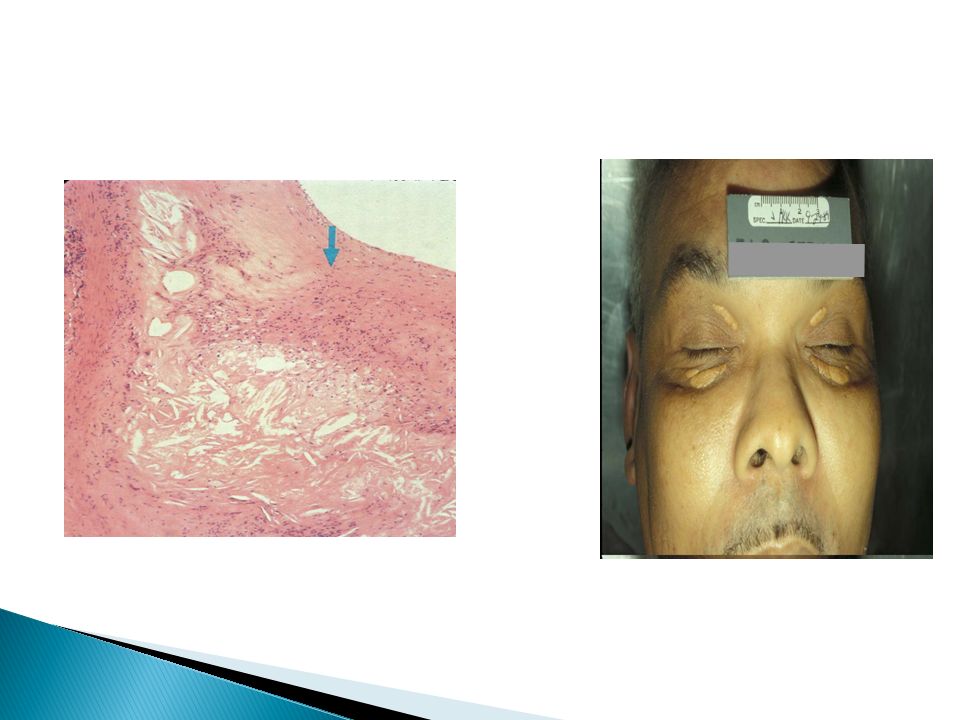
Inherited or acquired hyperlipidemic syndromes may lead to formation of xanthomas, cholesterol filled macrophages found in subepithelial connective tissue of skin or tendons

11
Less common than lipid accumulations Too much presented to cell or cell synthesizes excessive amounts Pinocytosis in proximal convoluted tubules in nephrotic syndrome results in greater reabsorption of albumin. Pinocytotic vesicles fuse with lysosomes leading to histologic appearance of pink, hyaline cytoplasmic droplets. Reversible if nephrotic syndrome is treated.

12
Immunoglobulins accumulate on RER of plasma cells forming Russell bodies

14
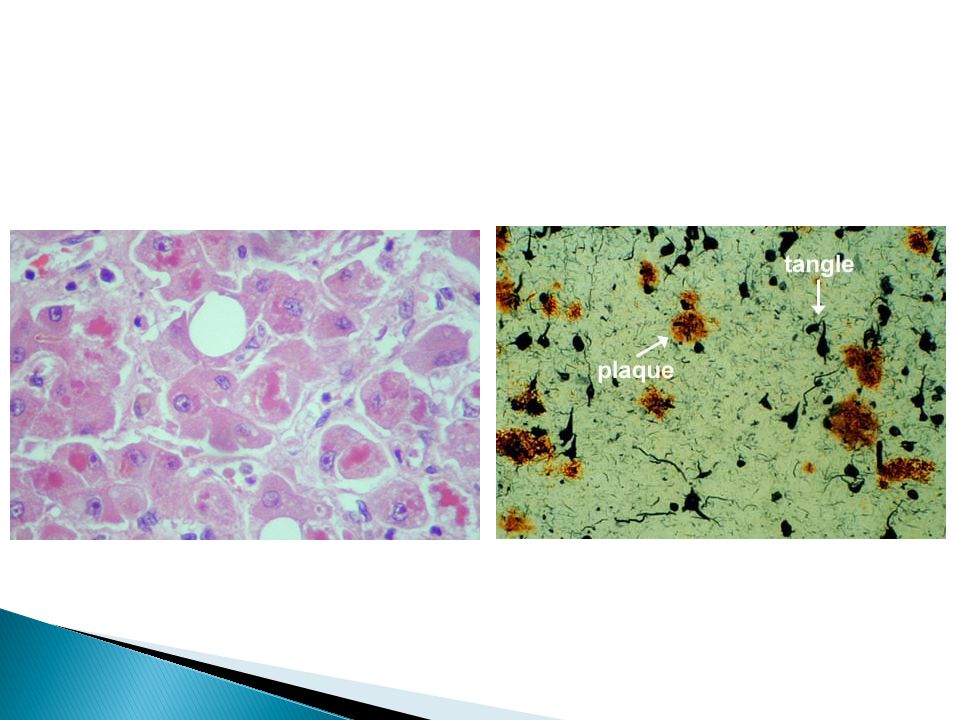
Mallory body, alcoholic hyaline, composed of aggregated intermediate filaments resistant to degradation and are highly characteristic of alcoholic liver disease. Neurofibrillary tangles of Alzheimer disease are aggregates that contain microtubule- associated proteins and neurofilaments due to disruption of neuronal cytoskeleton formation

16
Result from abnormal glucose or glycogen metabolism In diabetes mellitus, glycogen accumulates in renal tubular epithelium, myocardial cells and β cells of the islets of Langerhans. Glycogen storage disease or glycogenoses result of enzymatic defects

17
von Gierke’s Disease

18
Colored endogenous or exogenous substances ◦ Carbon particles most common exogenous substance breathed in to lung called anthracosis found in regional lymphatics and nodes and in lung parenchyma. Heavy exposure may lead to coal workers pneumoconiosis or induce emphysema

20
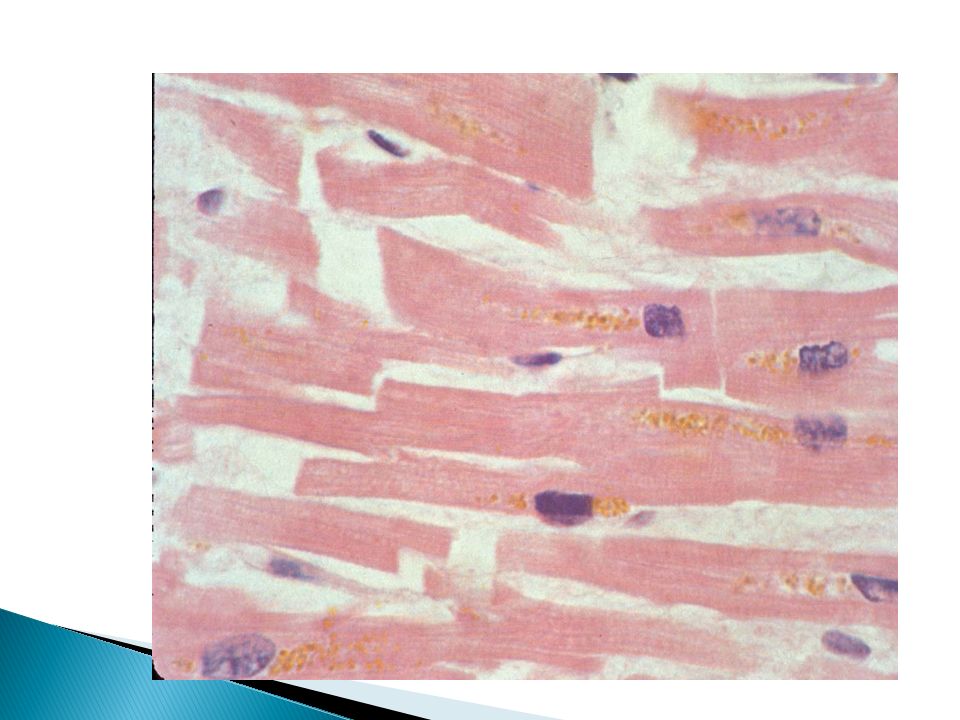
Endogenous pigments include lipofuchsin, melanin and derivatives of hemoglobin Lipofuchsin “wear and tear” pigment is insoluble brownish yellow granular intracellular material accumulates in heart, liver, brain as a function of age or atrophy and is a marker of past free radical injury Result of free radical catalyzed peroxidation of polyunsaturated lipids of subcellular membranes

21
Figure 1-40 Lipofuscin granules in a cardiac myocyte as shown by A, light microscopy (deposits indicated by arrows), and B, electron microscopy (note the perinuclear, intralysosomal location). Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 17 February 2005 01:49 PM) © 2005 Elsevier
 © 2005 Elsevier.")
22
Melanin is a brown-black pigment produced in melaocytes following tyrosinase catalyzed oxidation of tryosine to dihydroxyphenylalanine and is a screen against UV radiation. Can accumulate in basal keratinocytes (freckles) or in dermal macrophages
 or in dermal macrophages.")
24
Hemosiderin is a golden yellow to brown hemoglobin derived aggregate of ferritin micelles, found in tissue when there is a local or systemic excess of iron Iron normally stored in cell associated with apoferritin as ferritin micelles. Prussian blue stain used to identify hemosiderin Result of local hemorrhage as in bruises

25
Pancreas H & E stain Iron Stain Gross microscopic Prussian Blue

26
Hemosiderosis is accumulation of hemosiderin due to iron excess with non injurious deposition in macrophages of liver, bone marrow, spleen, lymph nodes and other organs but can accumulate in parenchymal cells of the liver, pancreas, heart and endocrine organs ◦ Increased absorption of dietary iron ◦ Impaired utilization of iron ◦ Hemolytic anemias ◦ Transfusions

27
Hemochromatosis is a hereditary disease with extensive accumulation of iron in liver, pancreas and heart leading to fibrosis, heart failure and diabetes mellitus

28
Abnormal deposition of calcium salts, iron, magnesium and other minerals Dystrophic calcification found in dead or dying tissue with normal calcium levels Metastatic calcification is found in normal tissue associated with hypercalcemia usually due to parathyroid hormone excess

29
Pathogenesis involves initiation and propagation with end product of crystalline calcium phosphate Extracellular initiation involves matrix vesicles where calcium concentrates due to its affinity for membrane phospholipids and phosphate accumulates due to membrane bound phosphatases Intracellular initiation involves mitochondria

31
Calcification in the interstitial tissue of vessels, kidneys, lungs and gastric mucosa due to one of the following ◦ Increased secretion of parathyroid hormone ◦ Destruction of bone ◦ Vitamin D related disorders ◦ Renal failure with secondary hyperparathyroidism

33
Results from combination of cell damage by free radicals, replicative senescence ( reduced capacity of cells to divide due to decreasing amounts of telomerase and progressive shortening of telomeres) and reduced repair of damaged DNA Cummulative DNA damage results from defective repair mechanisms. Calorie restriction has been shown to activate DNA repair Accumulation of metabolic damage and possible role of growth factors which promote aging

34
A reversible change in the number, size, phenotype, metabolic activity or functions of cells in response to change in their environment Physiologic adaptation ◦ Hormones or endogenous chemical mediators Pathologic adaptation ◦ Response to stress that allow cell to escape injury

35
Increase in cell size leading to increase in organ size Physiologic ◦ Increased functional demand ◦ Hormonal stimulation Pathologic ◦ Hypertension ◦ Aortic valve disease

36
Cells which can not divide Cardiac hypertrophy involves mechanical triggers (stretch) and trophic triggers (activation of α adrenergic receptors) Turn on signal transduction pathways leading to improved performance Switch of contractile proteins from adult to fetal or neonatal forms ◦ Β-myosin heavy chain replaces the α-myosin heavy chain as it has slower more energy economical contraction.
 and trophic triggers (activation of α adrenergic receptors) Turn on signal transduction pathways leading to improved performance Switch of contractile proteins from adult to fetal or neonatal forms ◦ Β-myosin heavy chain replaces the α-myosin heavy chain as it has slower more energy economical contraction.")
38
There is a limit past which the enlargement of cells and increase in cell components will exceed the cells ability to adapt and ultimately lead to failure. The process is incompletely understood but may include fragmentation of fibers, lack of adequate blood supply or inadequate ATP, leading to failure is stress is not relieved.

39
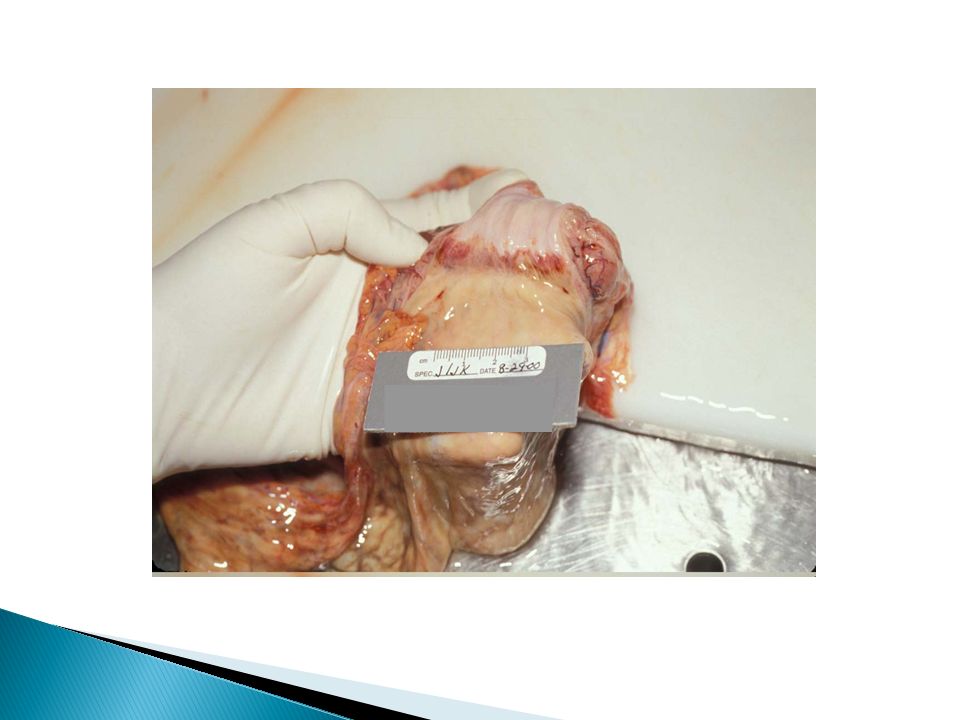
Figure 1-3 Physiologic hypertrophy of the uterus during pregnancy. A, Gross appearance of a normal uterus (right) and a gravid uterus (removed for postpartum bleeding) (left). B, Small spindle-shaped uterine smooth muscle cells from a normal uterus (left) compared with large plump cells in gravid uterus (right). Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 17 February 2005 01:49 PM) © 2005 Elsevier
 and a gravid uterus (removed for postpartum bleeding) (left). B, Small spindle-shaped uterine smooth muscle cells from a normal uterus (left) compared with large plump cells in gravid uterus (right). Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 17 February :49 PM) © 2005 Elsevier.")
40
Increase in cell number in cell populations capable of replication Physiologic ◦ Hormonal hyperplasia i.e. breast tissue ◦ Compensatory hyperplasia i.e. liver Pathologic ◦ Excessive hormonal or growth factor stimulation ◦ Excessive menstrual bleeding ◦ Keloid scars ◦ Warts ◦ Possible malignant transformation

42
Shrinkage in size of the cell by loss of cell substance leading to diminished function ◦ Decreased work load ◦ Loss of innervation ◦ Diminished blood supply ◦ Inadequate nutrition ◦ Loss of endocrine stimulation ◦ Aging

43
Decreased protein synthesis and increased protein degradation Protein degradation occurs by ubiquitin- proteosome pathway where small ubiquitin peptides attach to proteins which are then degraded in proteosomes Cachexia of malignancies Increased numbers of autophagic vacuoles Increased amounts of lipofuchsin may be seen

47
Reversible change of one adult cell type by another adult cell type in the epithelium or in mesenchymal cells, a change in phenotype Genetic “reprogramming” of stem cells not transdifferentiation of already differentiated cells Squamous metaplasia of respiratory epithelium in smokers Gastric metaplasia of squamous epithelium in esophagus

49
New cell type may survive but there is a loss of protective mechanisms May predispose to malignant transformation In mesenchymal cells, there may be bone formation in a area of injury

50
Figure 1-6 Metaplasia. A, Schematic diagram of columnar to squamous metaplasia. B, Metaplastic transformation of esophageal stratified squamous epithelium (left) to mature columnar epithelium (so-called Barrett metaplasia). Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 17 February 2005 01:49 PM) © 2005 Elsevier
 to mature columnar epithelium (so-called Barrett metaplasia). Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 17 February :49 PM) © 2005 Elsevier.")
52
Hypertrophy in cells which cannot divide increased cell and organ size response to increased work by mechanical stretch and growth factors Hyperplasia increased cell numbers in response to hormones and other growth factors in tissue capable of cell division Atrophy decreased cell size and organ size as a result of decreased nutrients or disuse; decreased synthesis and increased proteolytic breakdown of cellular organelles Metaplasia change in phenotype of differentiated cells in response to irritation by altered differentiation pathway of tissue stem cells leads to lost functions and increased risk of malignancy

53
Nancy L Jones, MD

Similar presentations

















: Fatty Change (Steatosis): Abnormal accumulation of triglycerides within parenchymal cells seen in.>")









 state>")

>")