Download presentation
Presentation is loading. Please wait.

1
Celiac Disease Ben Thomas, D.O. Gastroenterology Specialty Medicine Care, Beavercreek, OH

2
38 y.o. female new patient with biopsy and serology confirmed celiac disease. She has been on a strict gluten free diet for 5 years and doing well. She visits your office for a recent increase in symptoms. What is most likely causing her symptoms? A- Small Bowel Lymphoma B- Inadvertent Gluten Ingestion*** C- Irritable Bowel Syndrome D- Type 2 Refractory Celiac Disease

3
38 y.o. female new patient with biopsy and serology confirmed celiac disease. She has been on a strict gluten free diet for 5 years and doing well. She visits your office for a recent increase in symptoms. What is most likely causing her symptoms? A.Small Bowel Lymphoma B.Inadvertent Gluten Ingestion C.Irritable Bowel Syndrome D.Type 2 Refractory Celiac Disease 10

4
21 y.o. male with Type 1 diabetes. New bloating and diarrhea. Mild iron deficiency anemia. You suspect celiac disease. What is the best initial evaluation? A.Initiate gluten free diet and assess for response B.Order upper endoscopy with gastric biopsies C.HLA testing D.TTG IgA antibody testing with serum IgA level 10

5
You’ve been asked to evaluate a 35 y.o. female who is concerned that she may have celiac disease. Her friend told her to start a gluten free diet. She feels a little better on the diet. How would you test her today to rule out celiac disease? A.Upper endoscopy with biopsy B.Anti-TTG IgA C.HLA testing D.D-xylose testing 10

6
First described by Samuel Gee in 1888, “On the Coeliac Affection” Cause was unexplained until Dutch physician during WWII noticed patient symptoms change during food shortages/rationing wheat, barley, rye, and oats Lesions in the small bowel were not identified until 1954

7
One of the most common causes of chronic malabsorption injury to the small intestine with loss of absorptive surface area, reduction of digestive enzymes, and impaired absorption net secretion of fluid

8
Epidemiology primarily in whites of northern European ancestry 1:70 to 1:300 individuals affected strong family history 1:22 first degree relatives

9
Underdiagnosed in the United States prevalence in dyspepsia (1%)- mucosal biopsies should be considered in patients with dyspepsia first degree relative increases risk (5-10%) testing asymptomatic patients? type 1 diabetes mellitus (3-10%)
.")
10
Risk of malignancy non-hodgkin’s lymphoma increased risk of all-cause mortality

11
Genetic factors immune disorder triggered by an environmental agent (gliadin) HLA DQ2 and/or DQ8 Serum autoantibodies ELISA for IgA antibodies to gliadin immunofluorescence for IgA antibodies to endomysium tissue transglutaminase IgG antibody deaminated gliadin
 HLA DQ2 and/or DQ8 Serum autoantibodies ELISA for IgA antibodies to gliadin immunofluorescence for IgA antibodies to endomysium tissue transglutaminase IgG antibody deaminated gliadin")
12
Presentation Classic Celiac Disease villous atrophy symptoms of malabsorption resolution of mucosal lesions and symptoms upon withdrawal of gluten-containing foods Typically present with diarrhea, weight loss, or malabsorption and have antibodies against gliadin (TTG)
")
13
Atypical celiac disease- anemia, dental enamel defects, osteoporosis, arthritis, elevated liver enzymes, infertility Silent Celiac Disease- incidental finding with minor symptoms that resolve on gluten free diet

14
presents often between the ages of 10 and 40 years diarrhea with bulky, foul-smelling, floating stools, flatulence growth failure in children, weight loss, anemia, deficiencies in B vitamins, and osteopenia

15
Subclinical disease fatigue, mild iron deficiency, mild elevation in transaminases, or asymptomatic still at risk for malignancy, nutritional deficiencies, low birth weights, and other autoimmune diseases

16
Non-GI manifestations Neuropsychiatric disease- headache, neuropathy, ataxia, depression Iron deficiency- Metabolic bone disease- malabsorption, vitamin D deficiency Fertility

17
Anemia common manifestation impaired iron or folate absorption from proximal intestine hyposplenism, thrombocytosis, deformed erythrocytes

18
Osteopenia common manifestation in older patients impaired calcium absorption and vitamin D deficiency unclear whether untreated celiac disease leads to increase in fractures

19
Neurologic symptoms poorly understood progressive gait and limb ataxia immunologic damage to the cerebellum, spinal cord, and peripheral nerves epilepsy and seizures

20
Fertility problems common in women with untreated celiac disease amenorrhea infertility sperm abnormalities

21
Dermatitis herpetiformis papulovesicular lesion that occur symmetrically over extensor surfaces of extremities and buttocks, trunk, neck, and scalp immunofluorescence of speckled IgA deposits can have patchy erythema in intestine unrelated to celiac disease HLA-DQ2 association

23
Diabetes mellitus closely associated with type 1 diabetes and autoimmune thyroiditis shared genetic loci- HLA DR3, DQ2 (DQ8) Down Syndrome- 20 fold increase risk of celiac disease Liver disease- non-specific mild chronic elevation in AST/ALT
 Down Syndrome- 20 fold increase risk of celiac disease Liver disease- non-specific mild chronic elevation in AST/ALT")
24
Diagnosis Who should be tested? chronic or recurrent diarrhea, malabsorption, weight loss, abdominal distention or bloating iron deficiency anemia, folate, or B12 deficiency, elevated liver enzymes, neuropathies, or recurrent headaches type 1 diabetes and first degree relatives with celiac disease; Down syndrome

25
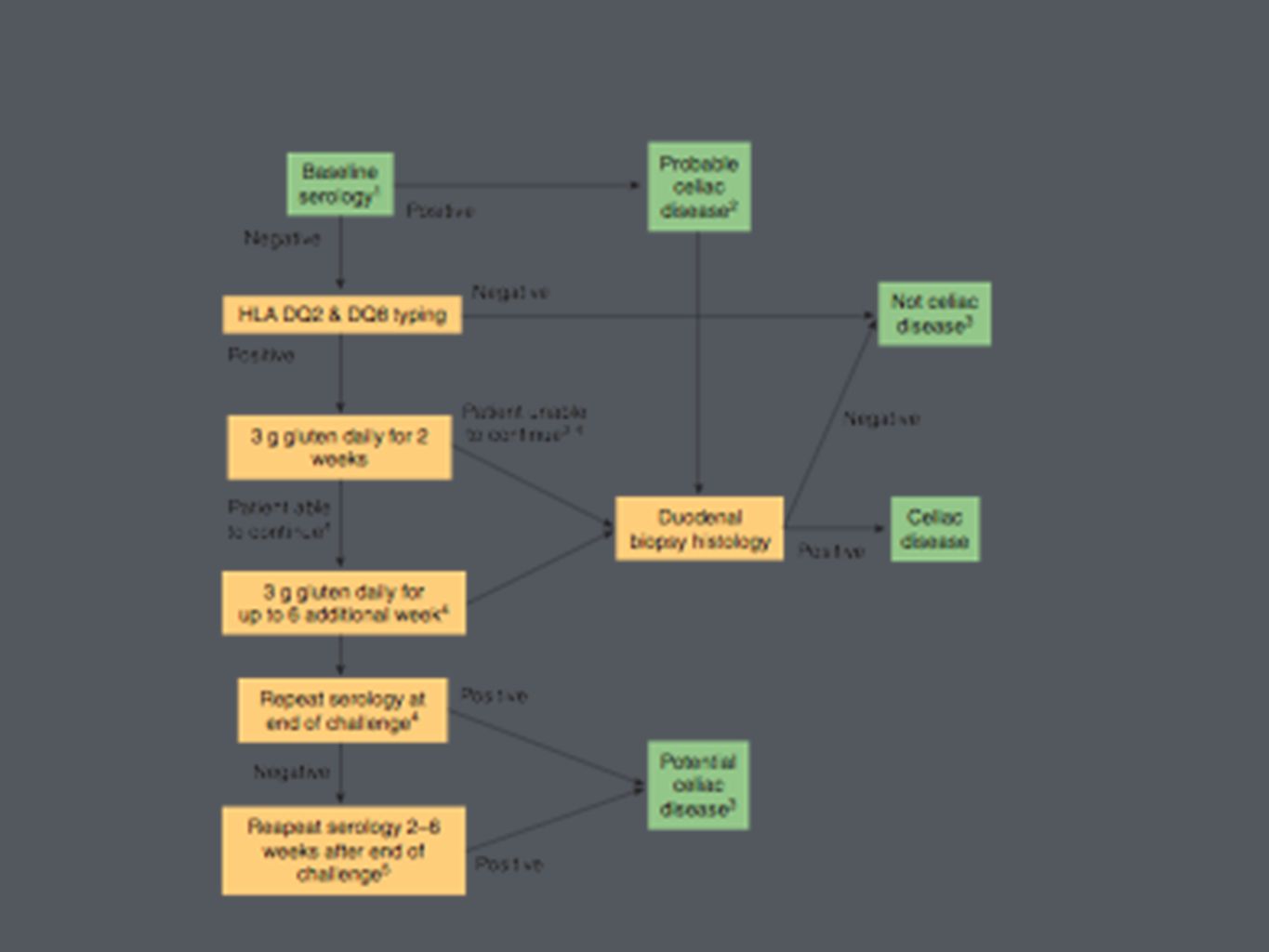
Most important genetic risk factor for celiac disease HLA-DQ2 and DQ8 negative testing makes celiac disease very unlikely

26
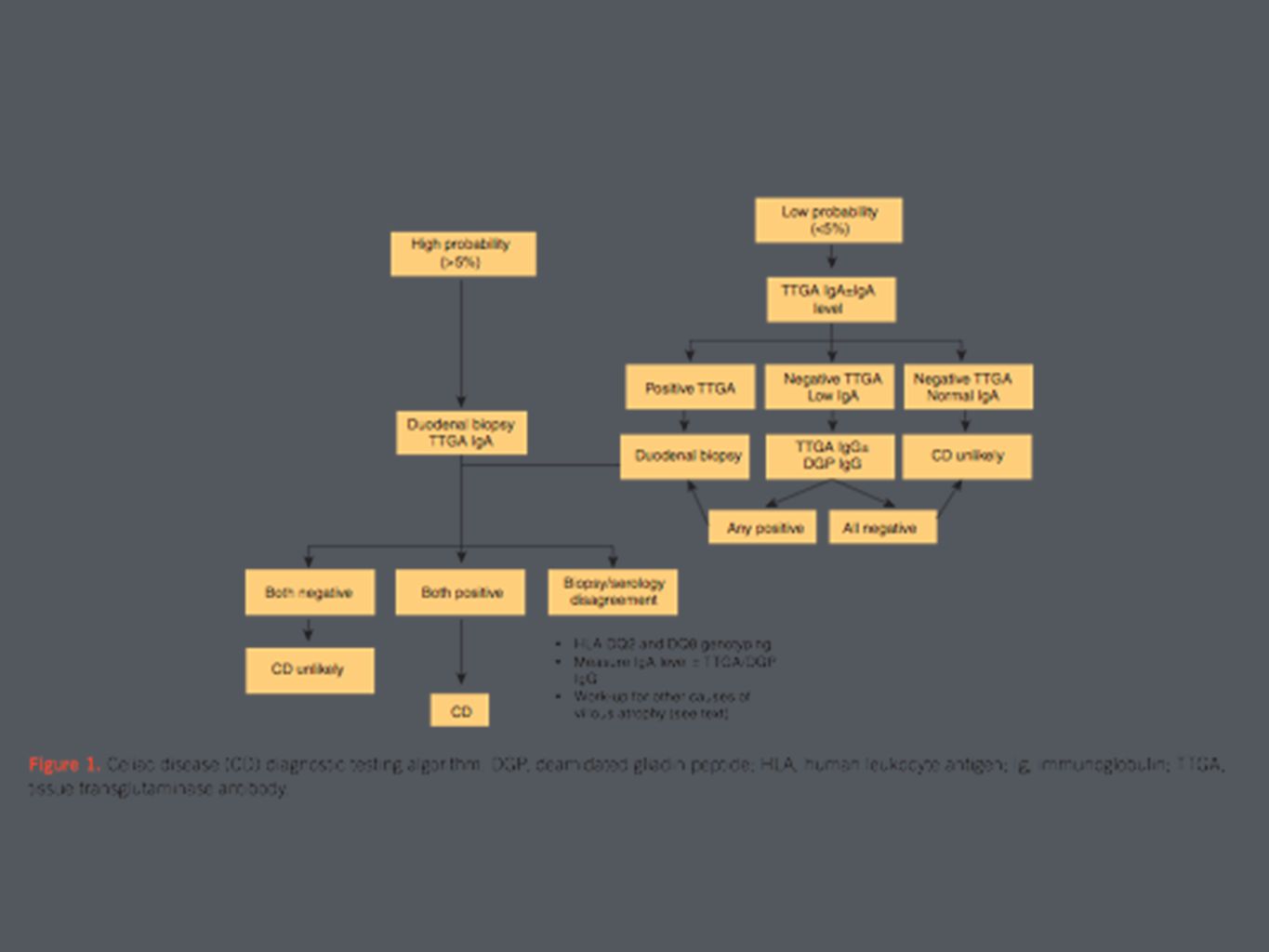
Serology IgA anti-tissue transglutaminase IgG-deaminated gliadin important for testing to be performed without gluten withdrawal DQ2/DQ8 testing

27
IgA endomysial assay bind to connective tissue surrounding smooth muscle cells positive or negative test target antigen is tissue transglutaminase moderately sensitive and highly specific

28
Antigliadin antibody assay component of wheat storage protein gluten not recommended due to low positive predictive value second generation testing against deaminated gliadin more sensitive and specific

29
Anti-tissue transglutaminase (TTG) antibody improvement upon anti-gliadin, reticulin, and endomysium antibody based testing IgA deficiency IgG based TTG or IgG DGP
 antibody improvement upon anti-gliadin, reticulin, and endomysium antibody based testing IgA deficiency IgG based TTG or IgG DGP")
30
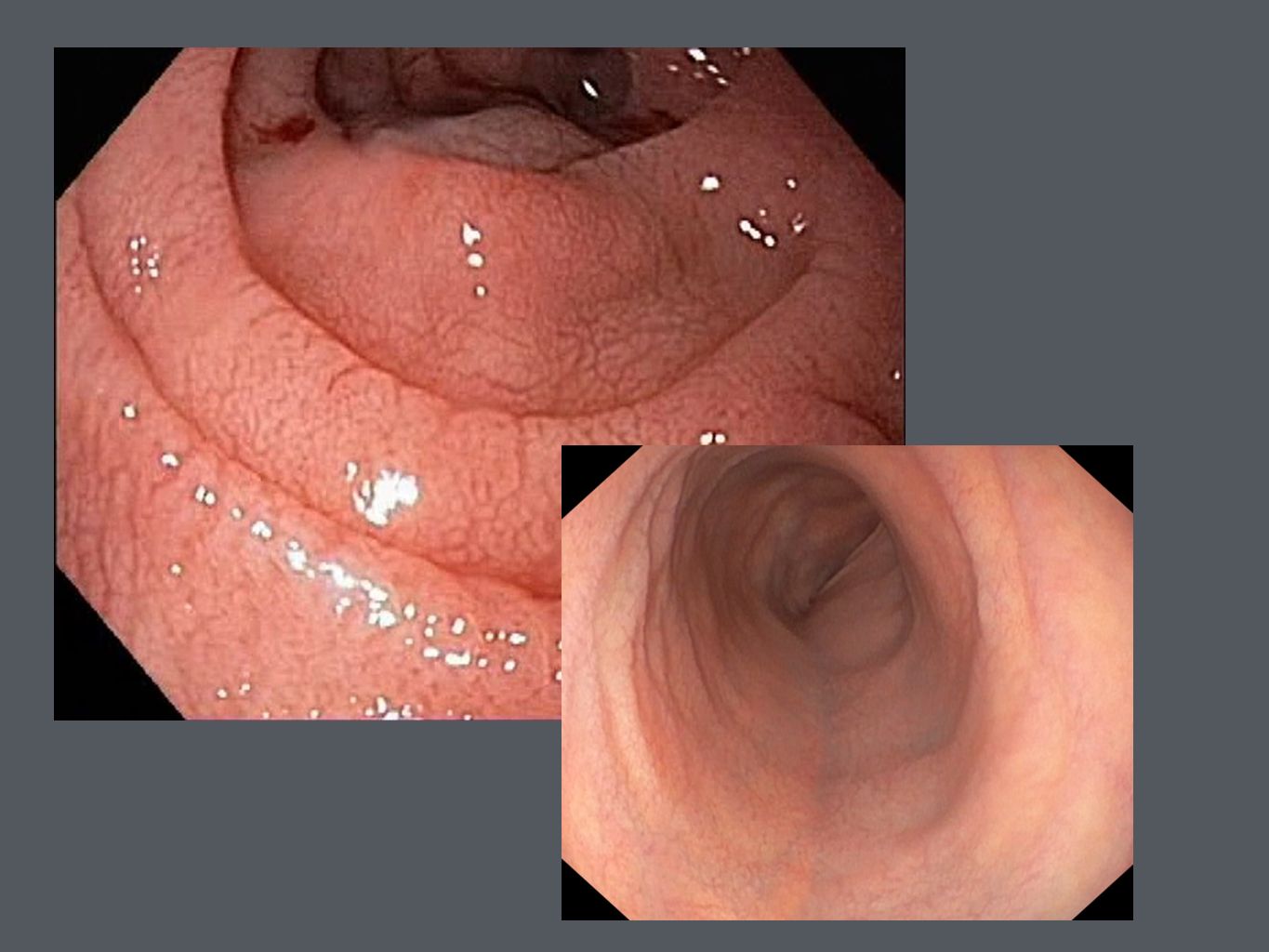
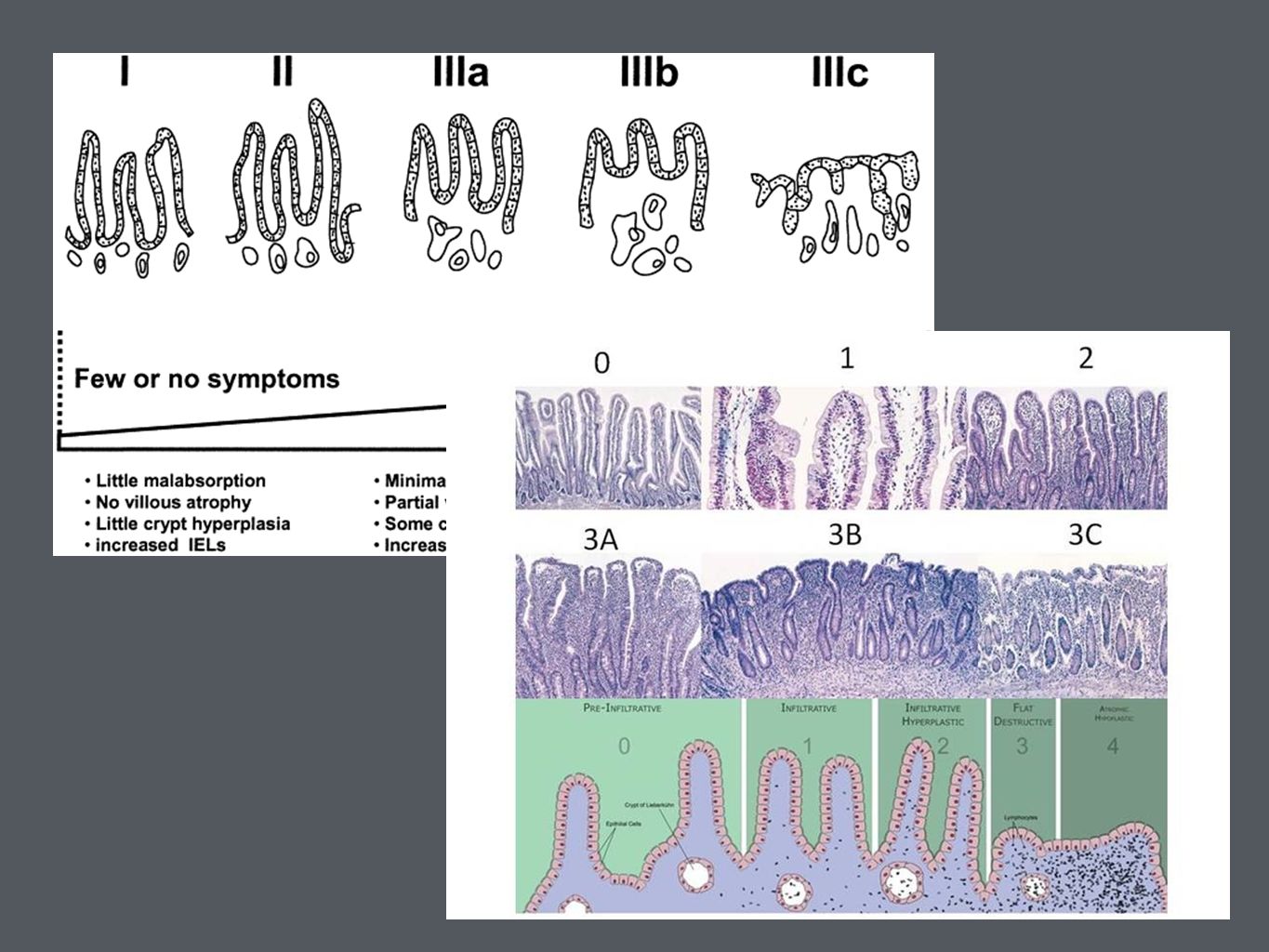
Small bowel biopsy upper endoscopy with small bowel biopsies duodenal mucosa appears atrophic with loss of folds, visible fissures, nodular appearance, or scalloping of the folds histologic features include loss of villi, increased intraepithelial lymphocytes, mucosal atrophy, and crypt hyperplasia

33
Biopsies are recommended 2 from duodenal bulb and at least 4 from beyond the duodenal bulb Marsh Classification

37
Clinical features without positive serologic testing IgA deficiency low gluten diet false negative testing non-celiac disease- wheat allergy or non-celiac gluten sensitivity

38
Positive Serologies but Negative Biopsies repeat IgA based TTG testing gluten challenge (6-12 weeks)
")
40
Confirmation of diagnosis symptoms alone cannot differentiate 20-50% of patients with celiac disease met Rome criteria for IBS ingestion of gluten can cause GI symptoms regardless of celiac disease

41
Other testing capsule endoscopy CT enterography (MR) D-xylose measurement
 D-xylose measurement")
42
Treatment Dietary Counseling gluten free diet recommended in patients with celiac disease referral to a registered dietitian knowledgeable about celiac disease

43
lifelong gluten free diet is the only effective treatment for celiac disease decreases risk for malignancies associated with celiac disease improves nutritional parameters

44
principle sources of dietary gluten wheat rye barley oats?? read labels carefully, especially additives

45
distilled alcohol and wine dairy products may not be well tolerated oats should be introduced with caution and intake be limited

46
Response to gluten free diet 70% have noticeable clinical improvement within 2 weeks symptoms improve much faster than histology repeat lab testing 4-6 weeks after gluten free diet

47
Should we stay on a gluten free diet? micronutrient deficiencies increased overall mortality and risk of lymphoproliferative disease and GI cancers development of other autoimmune disorders

48
Repeat serologic testing IgA anti tissue transglutaminase or IgA deaminated gliadin peptide should be used to monitor response to gluten-free diet normal levels do not correlate with histology persistently high levels usually reflect continued exposure to dietary gluten

49
Repeat small bowel biopsy upper endoscopy should be repeated in patients who fail to respond to a gluten-free diet or have relapse of symptoms on a gluten-free diet

50
if duration of gluten free diet less than 1 month traditional testing/serology often are still abnormal DQ2 and DQ8 testing are not influenced by diet gluten challenge

51
Non-responders persistent symptoms or serologic/histologic abnormalities after two years on a gluten free diet Often due to: poor compliance or inadvertent gluten ingestions features that overlap with celiac disease other disorders refractory sprue ulcerative jejunitis or intestinal lymphoma

52
Poor compliance most common reason for lack of response recommend meticulous dietary history should be obtained and dietary counseling Other diagnosis lactose intolerance, irritable bowel disease, small bowel bacterial overgrowth, pancreatic insufficiency, microscopic colitis

53
Attention must be paid to hidden sources of gluten in commercially prepared foods Registered dietitians are trained to evaluate and counsel patients on how to maintain a strict gluten free diet Academy of Nutrition and Dietetics long term monitoring for compliance

54
Non-celiac gluten sensitivity no diagnostic features of celiac disease but develop celiac-like symptoms upon exposure to dietary gluten

55
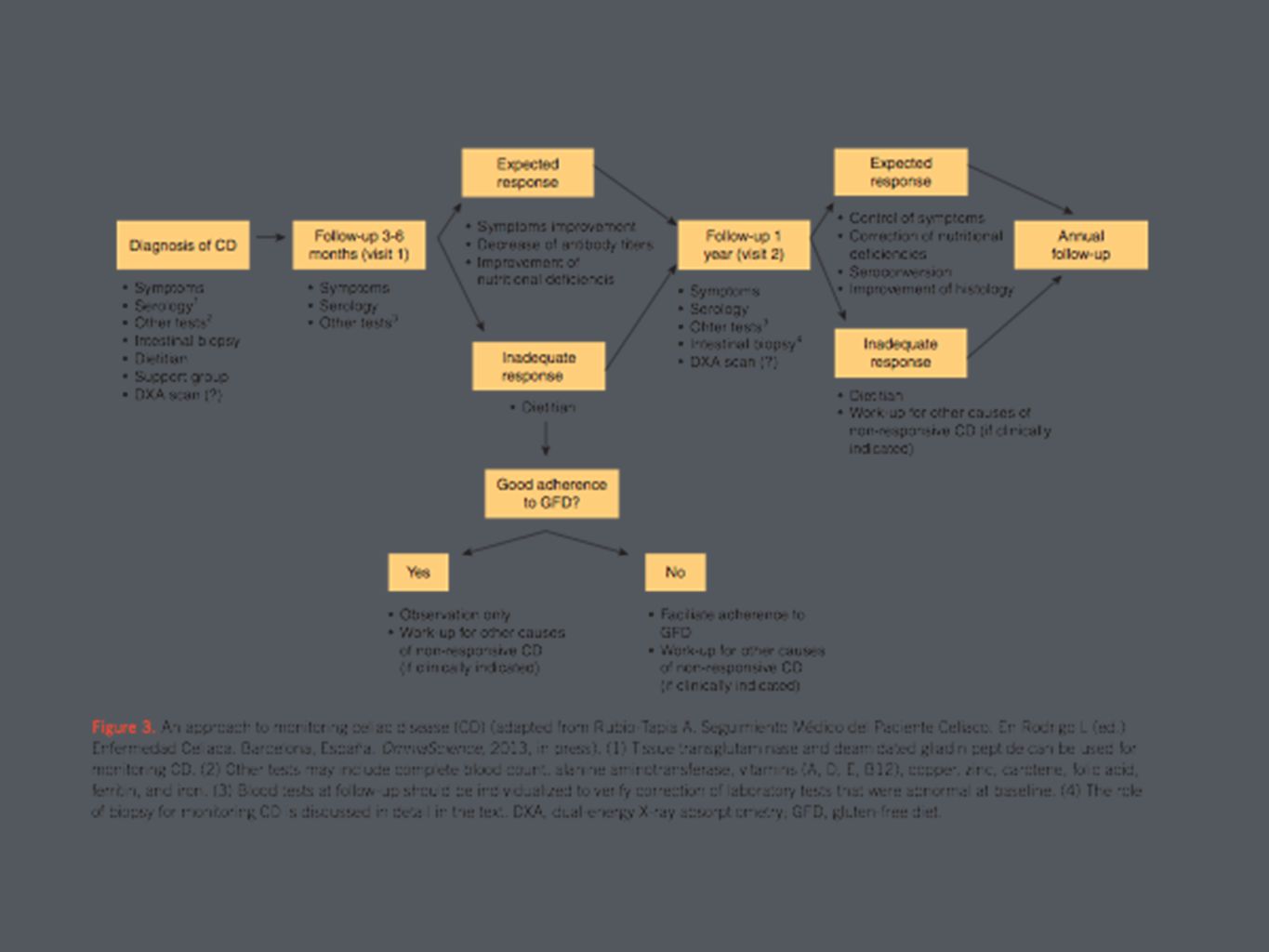
Long term follow up is recommended annual follow up with serology is associated with increased rate of seroconversion of TTG antibody gold standard for monitoring adherence to diet is consultation with dietitian median time from onset of gluten free diet to mucosal healing was 3 years

57
Non-responsive or Refractory Celiac Disease persistent symptoms, signs, and lab abnormalities typical of celiac disease despite 6-12 months of dietary gluten avoidance most commonly inadvertent gluten ingestion if dietary causes have been excluded, repeat endoscopy with biopsy is recommended

58
Ulcerative jujunoileitis rare complication of celiac disease ulceration and strictures of the small intestine suspect in celiac disease with weight loss, abdominal pain, and diarrhea that do not respond enteroscopy, capsule endoscopy, or small bowel studies

59
Refractory celiac disease is persistent or recurrent symptoms and signs of malabsorption with small bowel villous atrophy despite strict GFD for more than 12 months type 1: lymphocyte infiltration of small bowel mucosa type 2: CD3-positive intraepithelial T cells with abnormal immunophenotype

60
Type 1 RCD excluding gluten exposure treatment for nutrition deficiencies symptomatic treatment systemic steroid therapy; azathioprine

61
Type II RCD same as Type I RCD but less likely to respond profound malnutrition requiring parenteral nutrition support 5 year survival 44% compared to 93% with Type I transformation to enteropathy-associated T- cell lymphoma is prominent risk

62
Questions??

63
Resources American College of Gastroenterology Guidelines (ACG)- Diagnosis and Management of Celiac Disease American Gastroenterological Association (AGA) Institute Technical Review on the Diagnosis and Management of Celiac Disease Google Images Sleisenger and Fordtran’s Gastrointestinal and Liver Disease (Ninth Edition) UpToDate
- Diagnosis and Management of Celiac Disease American Gastroenterological Association (AGA) Institute Technical Review on the Diagnosis and Management of Celiac Disease Google Images Sleisenger and Fordtran’s Gastrointestinal and Liver Disease (Ninth Edition) UpToDate")
Similar presentations















>")






