Download presentation
Presentation is loading. Please wait.

1
Clostridium difficile Prevention Strategies

2
Objectives: Identify Seriousness of Clostridium difficile infection. Surveillance strategies. Prevention bundles.

3
Clostridium difficile infection is a potentially life threatening infection of the lower gastrointestinal tract.

4
Clostridium difficile infection is at epidemic levels in the United States! Any listed dx. Primary dx. National Estimates of US Short-Stay Hospital Discharges From McDonald LC, et al. Emerg Infect Dis. 2006;12:409-415; McDonald LC, et al. Clostridium difficile infection in patients discharged from US short-stay hospitals, 1996 to 2003. Emerg Infect Dis. 2006;12:409-415.*

5
C. diff It has two forms… 1.An active form…vegetative Survives in our bodies…produces the toxins Cannot survive in the aerobic environment very long…24 hours

6
C. diff 2.Inactive form, called a spore Can survive in the aerobic environment for up to 5 months* Allows for transmission! *William Rutala TV APIC Conference March 2008.

7
C. diff Pathogenic strains release 2 toxins: Toxin A and Toxin B, The toxins are what cause the problem! Attach to the colon lining and cause damage!

8
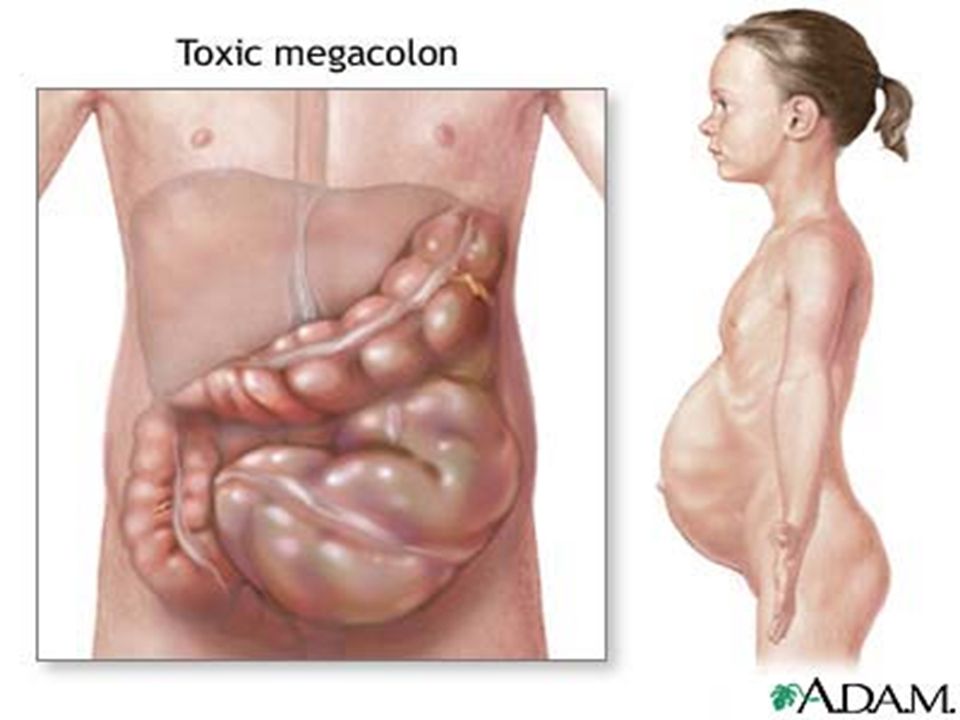
CDI Severity Mild diarrhea Pseudomembranous colitis Toxic megacolon Perforations of the colon Sepsis Death

9
Colonization Does C diff colonization put patients at increased risk? NO!

10
Asymptomatic colonization CDI higher in non-colonized patients than in colonized patients. 1,2,3,4. 1. Muto C, Pokrywka M, Shutt K, et al. Infect Control Hosp epidemiol.2005;26:273-280. 2. Walbrown MA, Aspinall SL,Bayliss NK et, al. J Manag Care Pharm. 2008;14:34-40. 3. Shim JK, Johnson S, Samore MH, Bliss DZ, Gerding DN. Lancet. 1988;351:633-636. 4. Poutanen SM, Simor,AE. CMAJ. 2004;171:51-58.

11
Antibody levels are high in asymptomatic carriers of C. difficile

12
NEW ACQUISITION!

13
Adapted from Clostridium difficile-Associated Disease: Clinical Aspects Dale N. Gerding, MD From Johnson S, Gerding DN. Clin Infect Dis. 1998;26:1027-1036 NEW Non-toxigenic strain Antibodies present Healthy colonic flora Toxigenic strain No Antibodies present Disrupted flora

14
Where is it in Healthcare? Healthcare workers hands Environmental contamination

15
How does it get in us?

16
CDI Once the spores are swallowed… Pass into the large intestine to multiply...Pass into the large intestine to multiply... Two toxins attack the colon …Two toxins attack the colon … Cause cell death of the lining…Cause cell death of the lining…

17
CDI Fluids rapidly pass through and exit as diarrhea…Fluids rapidly pass through and exit as diarrhea… Lots of it!Lots of it!

18
Normal colonappearance Normal colon appearance

19
Pseudomembranous colitis

21
Is CDI increasing? Yes! Incidence of CDI is increasing in the U.S. And There is an epidemic strain…much stronger!

22
CDI About 500,000 cases per year estimated Thought to be about 39,000 deaths per year. Mcdonald, C. 2010 Decennial Conf. Atlanta GA

23
CDI HO-HCFA 165,000 cases 9,000 deaths annually 1.3 billion costs CO-HCFA 50,000 cases 3,000 deaths 0.3 billion costs Nursing home onset 236,000 cases 16,500 deaths 2.2 billion in costs Mcdonald, C. 2010 Decennial Conf. Atlanta GA

24
Clostridium difficile National Prevalence Study One day “snapshot” May 7-August 29, 2008

25
National Prevalence Study 2008 648 facilities took part… C diff rates for the last 3 years. 82% of the organizations are unable to decrease these infections! Improving… only 18%

26
CDI deaths Mortality rate 6.9% at 30 days after diagnosis 16.7% at 1 year. 3,4,9 Outbreak mortality can be much higher! 3. Loo VG, Poirier L, Miller MA, et al. A predominantly clonal multiinstitutional outbreak of Clostridium difficile- associated diarrhea with high morbidity and mortality. N Engl J Med 2005; 353:2442-2449. 4. Pepin J, Valiquette L, Cossette B. Mortality attributable to nosocomial Clostridium difficile-associated disease during an epidemic caused by a hypervirulent strain in Quebec. CMAJ 2005; 173:1037-1042. 9. Dubberke ER, Reske KA, Butler AM, et al. Attributable outcomes of Clostridium difficile-associated disease in non-surgical patients. EmergInfect Dis (in press).
..")
27
Yearly Clostridium difficile–related deaths by Listing on Death Certificates, United States, 1999–2004. From Redelings MD, et al. Emerg Infect Dis. 2007;13:1417-1419. Deaths per million population *Picture added *

28
Risk factors Advanced age Antibiotics (disrupted flora) Prolonged hospital stay Proton Pump Inhibitors?
 Prolonged hospital stay Proton Pump Inhibitors")
29
Specimen Collection Testing … Should be performed only on diarrhea (unformed) stool… Unless ileus due to CDI is suspected. Testing of stools of asymptomatic patients is not clinically useful. It is not recommended.

30
Diagnosis of CDI Clinical presentation Laboratory tests Diagnostic imaging –Colonoscopy –Abdominal CT scan

31
Treatment Discontinue the implicated antibiotic (25% response) Supportive measures… fluids, electrolytes… Anti-peristaltic’s contraindicated Antimicrobial therapy
 Supportive measures… fluids, electrolytes… Anti-peristaltic’s contraindicated Antimicrobial therapy")
32
Treatment Oral Metronidazole Oral Vancomycin Standard treatment

33
Recurrent Infection Recurrences occur up to 35% of the time. 18 Risk of subsequent episodes up to 65%. 18 18.McFarland LV, Elmer GW, Surawicz CM. Breaking the cycle: treatment strategies for 163 cases of recurrent Clostridium difficile disease. Am J Gastroenterology. 2002;97:1769-1775.

34
Best Treatment PREVENTION

35
Prevention Bundle SurveillanceSurveillance EducationEducation Antimicrobial stewardshipAntimicrobial stewardship Environmental cleaningEnvironmental cleaning Hand hygieneHand hygiene Contact IsolationContact Isolation

36
Surveillance

37
CDI Surveillance Issues There is no standard U.S. reporting system. Prevalence Benchmarking Case definitions not widely reported

38
Surveillance Definitions Interim definitions and recommendations… Based on existing literature and expert opinion.

39
Surveillance Focus Healthcare Onset-Healthcare Facility Associated (HO-HCFA) CDI. Community Onset-Healthcare Facility Associated (CO-HCFA) CDI.
 CDI..")
40
Surveillance Focus HO-HCFA… CDI onset more than 48 hours after admission to a HCF. CO-HCFA… CDI onset within the 48 hour window, and symptom onset was less than 4 weeks after the last discharge from a HCF.

41
Surveillance Timelines Admission HO-HCFA Discharge < 4 weeks post DC CO-HCFA 4-12 wks Post DC Indeterminate >12 weeks CA Time-lines ** CO-HCFA: Community Onset- Healthcare Facility Associated CDI has onset on admission or within the 48 hour window, and symptom onset was < 4 weeks since last discharge from a HCF. ** CA: Community Associated CDI has onset on admission or within the 48 hour window and patient onset was > than 12 weeks since last discharge from a HCF. HO-HCFA: Healthcare Onset- Healthcare Facility Associated. CO-HCFA: Community Onset -Healthcare Facility Associated. Indeterminate disease: If CDI onset is within a 4-12 weeks time period since last discharge from a HCF. HCF: Healthcare facility. Defined as any acute care, long-term care, long term acute care, or other facility in which skilled nursing care is provided and patients are admitted at least overnight. *48hrs=Two complete 24 hour days. Adapted from CDI Surveillance Working Group. Infect Control Hosp Epidemiol 2007; 28: 140-145. ** 4 wks prior to admit *48 hrs

42
Surveillance Focus Tracking of healthcare onset-healthcare facility associated CDI is the minimum surveillance required for healthcare settings.* Tracking of community onset-healthcare facility associated CDI should be performed only in conjunction with tracking of healthcare facility onset-healthcare facility associated CDI.* *Adapted from Infect Control Hosp Epidemiol 2007; 28:140-145

43
Both HO-HCFA and CO-HCFA CDI… NIM eligible… Tracked using the NIM scorecard

44
Community Associated (CA)… Tracked using the CIM scorecard
… Tracked using the CIM scorecard")
45
CO-HCFA

46
Surveillance Consider… Rates of severe CDI. Highly virulent/epidemic strain ID.

47
Education Knowledge is power! Educate staff Don’t leave out EVS!

48
Antimicrobial Stewardship Proven prevention strategy! Maximizes antibiotic usage.

49
The Environment

50
Contamination?

51
Environmental Contamination Should we wait until we have a problem to clean? Should we clean known CDI patient rooms?

52
Environmental Contamination Adapted from :

53
A standardized cleaning regimen is a must!

55
Hand Hygiene

56
Hand rub and handwashing

57
Prevention Contact IsolationContact Isolation SignageSignage Gown and gloves when entering roomGown and gloves when entering room

58
Just when we thought it couldn’t get worse….

59
Epidemic Strain ( NAP 1, Type III) Has been around since 1980’s…but rare… 6000 isolates from years 1980-2000 had 14 NAP1, epidemic since 2000. NAP1 strain has a gene deletion, causing greater quantities of toxins A and B... 16-23 times more. Toxin regulating! Binary toxin.

60
Prevalence Outbreaks in 10 countries NAP1 is usually about 30% of isolates

61
Epidemic Strain NAP 1 Is more resistant to Fluoroquinolones. 1,2 Higher mortality...2 times more likely to die! 1. McDonald LC, et al. 42nd Annual Meeting of the Infectious Diseases Society of America (IDSA); 2004. Abstract LB-2 2. McDonald LC, et al. N Engl J Med. 2005;353:2433-2441.
; Abstract LB-2 2. McDonald LC, et al. N Engl J Med. 2005;353:")
62
Fluoroquinolones as Risk Factor A study during an epidemic in Quebec 293 cases of CDAD –50.5% of patients were ≥ 80 years old –63.5% received fluoroquinolones –21.8% died within 30 days of diagnosis Fluoroquinolones identified as most important risk factor for CDAD during large epidemic Adapted from Pépin J, et al. Clin Infect Dis. 2005;41:1254-1260.

63
Epidemic strain CDI outbreak 2000-2002 Pittsburgh Pennsylvania –Life-threatening disease doubled –2000-2001: 26 colectomies and 18 deaths Fluoroquinolone use a major factor! Carlene Muto

64
Epidemic Strain All epidemic strains from Quebec, UK and US have the… Gene deletion...toxin over-production Fluoroquinolone resistance Increased morbidity and mortality Adapted from Warny et al Lancet 2005;366:1079-84

65
Countries in Europe with BI/NAP1/027, November 2007

66
Pink = Pos

67
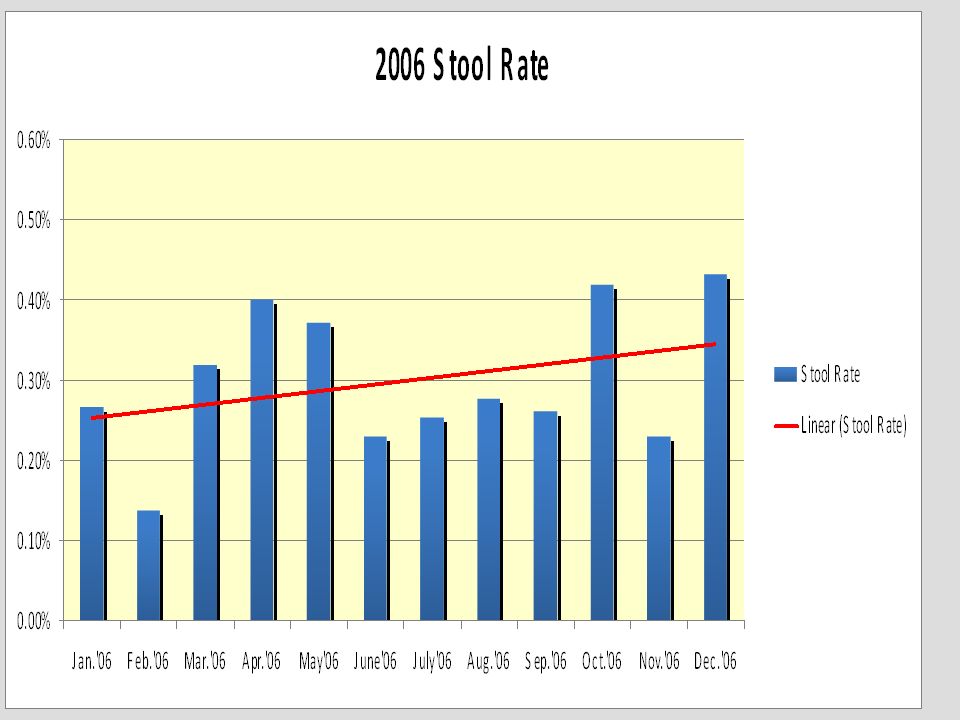
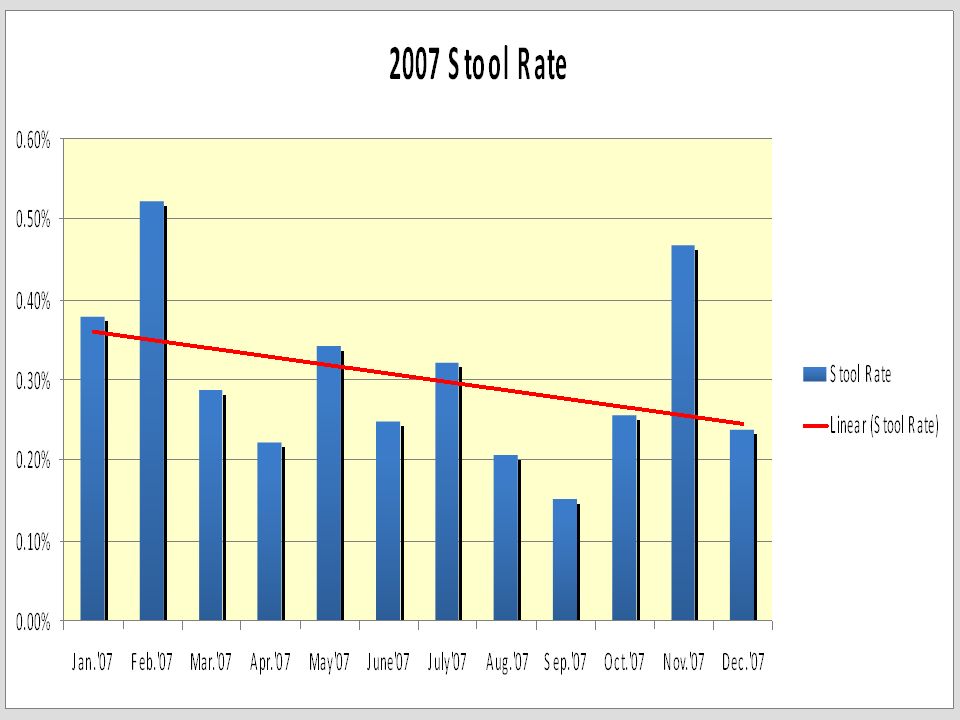
How were we doing?

69
Time to get serious!

70
Stepped up bundle use! Targeted education: EVS environmental cleaning…CBL. EVS environmental cleaning…CBL. Unit based education on… Unit based education on… CDICDI Hand hygiene Hand hygiene Contact Isolation Contact Isolation

71
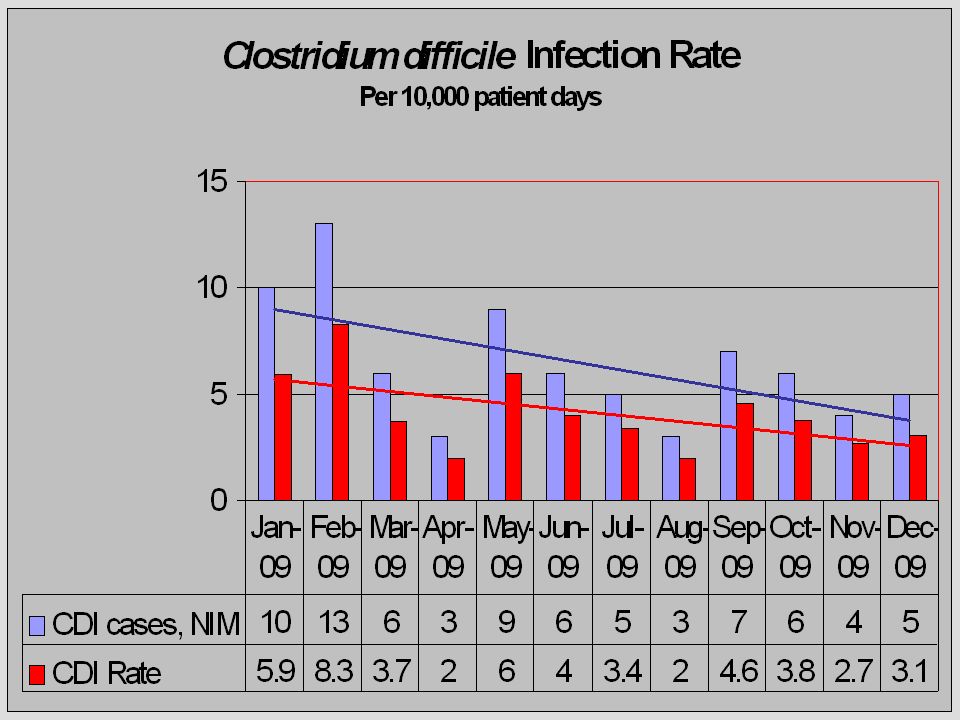
Surveillance Sentinel use Increase known real time. Daily isolation check. Severity/mortality.

73
Jan 08 Feb 08 March 08 April 08 May08 June 08 July 08 Aug 08 Sep 08 Oct 08 Nov 08 Dec 08

76
Future considerations Prevention bundles Standard reporting Testing methods New treatment methods

77
Summary/Comments CDI is at epidemic levels in the US and rising! Prevention is key!

78
Questions? Thank You!

Similar presentations



 Infections Toolkit Activity C: ELC Prevention Collaboratives Draft - 12/23/09 --- Disclaimer: The findings and conclusions.>")






: Fast Facts. What is Clostridium difficile (C. diff)? C. diff is a bacteria that lives in the intestinal tract of about.>")


 surveillance in Colorado Kelly R. Kast, MSPH.>")
 Infections For National Patient Safety Goal 07.03.01 2009.>")
, CIC Infection Preventionist Consultant.>")



 Nebraska Public Health Laboratory 402-559-7774.>")

