Download presentation
Presentation is loading. Please wait.

1
Differential Diagnosis of Parkinsonism
Katie Kompoliti, M.D. Associate Professor Movement Disorders Section Department of Neurological Sciences Rush University Medical Center

2
Parkinson’s Disease, Motor Abnormalities
Tremor Bradykinesia/akinesia Cogwheel rigidity Postural instability Parkinson disease is the most recognized of the movement disorders. Typically occurring in older indviduals, it is diagnosed clinically. The cardinal manifestations of Parkinson disease include the rest tremor, bradykinesia or slowness of movement and akinesia or lack of movement, muscle rigidity with a ratchety component, called cogwheeling and in advanced Parkinson disease, postural reflex impairment which causes difficulties with balance and falling. The gentleman shown in this slide has the typical posture of a patient with Parkinson disease. His posture is stooped, his elbows slightly flexed. He has a masked face and is walking slowly with a shuffle.

3
Parkinson’s Disease UKPDS Brain Bank Diagnostic Criteria
Inclusion criteria parkinsonism Bradykinesia One of the following Muscular rigidity Rest tremor Postural instability Supportive criteria for Parkinson’s Disease Begins on one side Remains asymmetric Rest tremor present Progressive disorder Responds to levodopa No atypical features Balance or falls in first year Early memory loss Early hallucinations Early problems with blood pressure, potency or urinary symptoms

5
Pathology of Parkinson’s Disease
On the left top is a picture of a normal midbrain with abundant pigmentation of the substantia nigra. Below that is the midbrain from a Parkinson’s disease patient with the substantia nigra depigmented. The second set at the top is the microscopic section of normal substantia nigra. Below that is the section from substantia nigra of a Parkinson’s patient. It shows profound loss of pigmented neurons and gliosis. On the extreme right is a pigmented neuron containing a Lewy body inclusion. The Lewy body is characterized by dense pink center and light pink periphery. Together, the loss of substantia nigra dopaminergic neurons and the presence of Lewy body inclusions are regarded as the hallmark of idiopathic Parkinson’s disease pathology.

6
DAT Scan to Differentiate Parkinson’s Disease from Essential Tremor

7
Early Parkinson’s disease
Early features Unilateral rest tremor Reduced spontaneous arm swing Loss of dexterity in one hand Loss of facial expression Unilateral foot dystonia (young onset) Pain in one shoulder
 Pain in one shoulder.")
8
Advancing Parkinson disease
Progression of PD Increased severity of motor symptoms Postural reflex impairment Loss of drug effect Freezing gait Drug side effects Motor fluctuations Dyskinesias

9
Parkinsonism, Differential Diagnosis
Primary parkinsonism Secondary parkinsonism Parkinsonism plus syndromes Heredofamiliar diseases

10
Parkinsonism, Differential Diagnosis
Primary parkinsonism Secondary parkinsonism Parkinsonism plus syndromes Heredofamiliar diseases

11
Primary Parkinsonism Dopa-responsive dystonia
Idiopathic Parkinson’s disease Juvenile parkinsonism

12
Juvenile Parkinsonism
Onset before 21 Heterogeneous disorder In most cases distinct from IPD Dystonia Sporadic or autosomal recessive Autosomal recessive chromosome 6q, Parkin (Park 2) no Lewy bodies
 no Lewy bodies.")
13
Dopa-Responsive Dystonia
Not a degenerative disease GTP-cyclohydrolase I gene Clinical features abnormal gait focal limb dystonia scoliosis rest or postural tremor bradykinesia rigidity diurnal fluctuation Normal PET or SPECT scans Levodopa responsive GTP cyclohydrolase is the enzyme that is responsible for the synthesis of tetrahydrobiopterin, an important cofactor of TH

14
Parkinsonism, Differential Diagnosis
Primary parkinsonism Secondary parkinsonism Parkinsonism plus syndromes Heredofamiliar diseases

15
Secondary Parkinsonism
Drugs antipsychotics, anti-emetics, tetrabenazine, reserpine, alpha-methyl-dopa, calcium channel blockers Hemiparkinsonism-hemiatrophy syndrome Hydrocephalus Infectious encephalitis lethargica, HIV, fungal, syphilis, SSPE, prion disease Metabolic symptomatic basal ganglia calcification/parathyroid abnormalities, acquired hepatolenticular degeneration Neoplastic Psychogenic Toxins MPTP, CO, Mn, cyanide, carbon disulfide, Hg, methanol Traumatic Vascular

16
Vascular Parkinsonism
Acute onset, stepwise progression Early gait/balance “lower body” Cognitive impairment Urinary incontinence Corticospinal or pseudobulbar signs Zijlmans JC et al. (2004), Mov Disord 19(6):
, Mov Disord 19(6):")
17
Vascular Parkinsonism
GTP cyclohydrolase is the enzyme that is responsible for the synthesis of tetrahydrobiopterin, an important cofactor of TH

18
Drug-Induced Parkinsonism
Drugs neuroleptics, anti-emetics, tetrabenazine, reserpine, alpha- methyl-dopa, calcium channel blockers, lithium, depakote Reversible Varies with: drug class, potency, dosage, length of treatment Treatment: discontinuation of offending agent switching to atypical neuroleptics anticholinergics, amantadine, sinemet?

19
Infectious Parkinsonism
Encephalitis lethargica HIV Fungal Syphilis SSPE Prion disease

20
Subacute Sclerosing Panencephalitis-SSPE
Progressive disorder 2-10 years after measles Cognitive, behavioral abnormalities, myoclonus, parkinsonism, coma, death (1-3 yrs) EEG periodic complexes High Ab titers in serum and CSF Atrophy, neuronal loss, lymphocytic infiltration, demyelination, gliosis, NFTs Nuclear oligodendroglial inclusions, staining for viral Ag (NP and HA proteins) Post-infectious encephalomyelitis (2 wks post acute infection) Subacute neasles encephalitis (1-9 months after acute infection), immunosuppressed patients Nuclear inclusions formed in oligodendroglia (in acute encephalitis also seen in neurons and astrocytes) Ultrastructurally the nucleus is filled with rod- or spiral-shaped tube-like structures representing the nucleocapsid of measles virus
 EEG periodic complexes. High Ab titers in serum and CSF. Atrophy, neuronal loss, lymphocytic infiltration, demyelination, gliosis, NFTs. Nuclear oligodendroglial inclusions, staining for viral Ag (NP and HA proteins) Post-infectious encephalomyelitis (2 wks post acute infection) Subacute neasles encephalitis (1-9 months after acute infection), immunosuppressed patients. Nuclear inclusions formed in oligodendroglia (in acute encephalitis also seen in neurons and astrocytes) Ultrastructurally the nucleus is filled with rod- or spiral-shaped tube-like structures representing the nucleocapsid of measles virus.")
21
Periodic bursts of high-amplitude, slow-wave complexes with normal background rhythm
Electroencephalogram (EEG) at the time of presentation in the neurology clinic (A) and 3 months later (B). The initial EEG (A) reveals periodic bursts of high-amplitude, slow-wave complexes. (Onset of the complexes is indicated by solid arrows; offset, by open arrows.) The background rhythm is normal, except for bifrontal slowing. This “burst-suppression” pattern is highly characteristic of subacute sclerosing panencephalitis
 at the time of presentation in the neurology clinic (A) and 3 months later. (B). The initial EEG (A) reveals periodic bursts of high-amplitude, slow-wave complexes. (Onset of the complexes. is indicated by solid arrows; offset, by open arrows.) The background rhythm is normal, except for bifrontal. slowing. This burst-suppression pattern is highly characteristic of subacute sclerosing panencephalitis.")
22
Transmissible Spongiform Encephalopathy
Sporadic CJD, % of cases with MD Cerebellar 70% Myoclonus 80% Extrapyramidal 56% Other (including tremor) 36% Brown P. Ann Neurol 1994 Proposed conversion of normal to pathological isoform of prion protein. Strings denote unstructured regions, coils denote alpha-helical structure, ribbons denote beta-sheet structure. Note reduction of alpha helical structure and conversion to beta-sheet structure With the exception of cerebellar, the others are rare early in the disease
 36% Brown P. Ann Neurol Proposed conversion of normal to pathological isoform of prion protein. Strings denote unstructured regions, coils denote alpha-helical structure, ribbons denote beta-sheet structure. Note reduction of alpha helical structure and conversion to beta-sheet structure. With the exception of cerebellar, the others are rare early in the disease.")
23
Transmissible Spongiform Encephalopathy

24
Psychogenic Parkinsonism
Not as frequent Maximal disability at onset Rigidity: voluntary resistance, no cogwheeling, distractible Bradykinesia: no fatiguing component Gait: atypical, arm held tightly to the trunk, exaggerated response to pull test Tremor: same at rest, posture action, variability, distractibility, entrainment CAUTION: Psychogenic parkinsonism has a high incidence of underlying Parkinson’s disease GTP cyclohydrolase is the enzyme that is responsible for the synthesis of tetrahydrobiopterin, an important cofactor of TH

25
Carbon Monoxide-Induced Parkinsonism
Long-term exposure or severe acute exposure Parkinsonism days to weeks later Two thirds complete recovery Other neurological manifestations memory impairment, confabulations emotional lability apraxia, agnosia stupor, coma hyperreflexia homonymous hemianopia vestibular dysfunction

26
Carbon Monoxide-Induced Parkinsonism
Carbon monoxide poisoning: Acute CO poisoning causes a cherry red discoloration of the brain and can also cause necrosis of the globus pallidus, as seen in this slide.

27
Mov Disord Sep;9(5):550-8. Neurological sequelae following carbon monoxide poisoning clinical course and outcome according to the clinical types and brain computed tomography scan findings. Lee MS, Marsden CD. Department of Neurology, Yongdong Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. Abstract The prognosis for patients who survive carbon monoxide (CO) poisoning is uncertain, particularly in those who develop persistent neurological complications after recovery from the initial coma. Thirty-one patients with the sequelae of CO poisoning, followed for a year, are described. Eight had a progressive course, and 23 had a delayed relapse after an initial recovery period of approximately 20 days (range, 1-36 days). Those with a progressive course developed a persistent akinetic-mute state, and four of the eight died. Those with the delayed relapsing course either developed a parkinsonian state with behavioral and cognitive impairment but could walk (nine cases), or progressed further to an akinetic-mute state, and were bed-bound (14 cases); the deterioration to either condition occurred rapidly over a few days to a week. Fourteen of the patients with the delayed relapses (61%) subsequently improved, but three (13%) died. Those with a progressive course without initial recovery were younger (mean age, 37.0 years) than those with a delayed relapsing course (55.2 years; p < 0.01). The mean duration of their initial coma (9.8 days) was longer than that in delayed relapsing cases (2.0 days; p < 0.01). The mean initial CO hemoglobin level was not different in the two groups. Brain computed tomography (CT) scans were obtained at the onset of sequelae in both groups. Ten patients had a normal CT scan, 13 had white matter low-density lesions, and four had globus pallidus low-density lesions. Yonsei Med J Jun 30;45(3):363-6. Chorea following acute carbon monoxide poisoning. Park S, Choi IS. Department of Neurology, Yonsei University College of Medicine, 134, Shinchon- dong, Seodaemoon-gu, Seoul , Korea. The clinical cases of 6 patients suffering with chorea after acute carbon monoxide (CO) poisoning were reviewed. There were 2 men and 4 women, and the age at onset ranged from 11 to 60 (mean 33.0) years. All the patients except one were associated with mild delayed CO encephalopathy. The latency period between CO poisoning and the onset of chorea was 10 to 30 (mean 21.7) days. The duration of chorea after CO poisoning was 14 to 90 (mean 39.8) days. The brain CT findings were bilateral low- density lesions in the basal ganglia and/or in the white matter of the cerebral cortex, and there was no correlation between the lesion sites on the imagings and the development of chorea. Neuroleptic agents alleviated the chorea and the patients did not relapse after neuroleptic agents were halted.
 poisoning is uncertain, particularly in those who develop persistent neurological complications after recovery from the initial coma. Thirty-one patients with the sequelae of CO poisoning, followed for a year, are described. Eight had a progressive course, and 23 had a delayed relapse after an initial recovery period of approximately 20 days (range, 1-36 days). Those with a progressive course developed a persistent akinetic-mute state, and four of the eight died. Those with the delayed relapsing course either developed a parkinsonian state with behavioral and cognitive impairment but could walk (nine cases), or progressed further to an akinetic-mute state, and were bed-bound (14 cases); the deterioration to either condition occurred rapidly over a few days to a week. Fourteen of the patients with the delayed relapses (61%) subsequently improved, but three (13%) died. Those with a progressive course without initial recovery were younger (mean age, 37.0 years) than those with a delayed relapsing course (55.2 years; p < 0.01). The mean duration of their initial coma (9.8 days) was longer than that in delayed relapsing cases (2.0 days; p < 0.01). The mean initial CO hemoglobin level was not different in the two groups. Brain computed tomography (CT) scans were obtained at the onset of sequelae in both groups. Ten patients had a normal CT scan, 13 had white matter low-density lesions, and four had globus pallidus low-density lesions. Yonsei Med J Jun 30;45(3): Chorea following acute carbon monoxide poisoning. Park S, Choi IS. Department of Neurology, Yonsei University College of Medicine, 134, Shinchon- dong, Seodaemoon-gu, Seoul , Korea. The clinical cases of 6 patients suffering with chorea after acute carbon monoxide (CO) poisoning were reviewed. There were 2 men and 4 women, and the age at onset ranged from 11 to 60 (mean 33.0) years. All the patients except one were associated with mild delayed CO encephalopathy. The latency period between CO poisoning and the onset of chorea was 10 to 30 (mean 21.7) days. The duration of chorea after CO poisoning was 14 to 90 (mean 39.8) days. The brain CT findings were bilateral low- density lesions in the basal ganglia and/or in the white matter of the cerebral cortex, and there was no correlation between the lesion sites on the imagings and the development of chorea. Neuroleptic agents alleviated the chorea and the patients did not relapse after neuroleptic agents were halted.")
29
Parkinsonism, Differential Diagnosis
Primary parkinsonism Secondary parkinsonism Parkinsonism plus syndromes Heredofamiliar diseases

30
Parkinsonism plus syndromes
Cortico-basal degeneration Dementia syndromes AD, DLB, fronto-temporal degeneration Multiple system atrophy OPCA Shy-Drager striato-nigral degeneration Parkinsonism-dementia-ALS complex Progressive pallidal, pallidonigral and pallidoluysio- nigral degeneration Progressive supranuclear palsy

31
Parkinsonism Synucleinopathy Parkinson’s Disease MSA
Dementia with Lewy bodies Tauopathy PSP CBD Frontotemporal dementia

32
Multiple System Atrophy Core Features
Autonomic dysfunction Orthostatic hypotension Urinary incontinence Erectile dysfunction Parkinsonism Poor levodopa response Cerebellar dysfunction Gait ataxia/limb ataxia Dysarthria Gaze evoked nystagmus Corticospinal abnormalities Hyperreflexia extensor plantar responses Litvan I (2003), Mov Disord 18(5): ; Weiner WJ (2005), Rev Neurol Dis 2(3):
, Mov Disord 18(5): ; Weiner WJ (2005), Rev Neurol Dis 2(3):")
34
Dementia with Lewy Bodies Core features
Parkinsonism Dementia Within 1 year of onset Fluctuating cognition pronounced variation in attention and alertness Recurrent visual hallucinations Cortical Lewy Bodies Ubiquitin Immunocytochemistry Litvan, Mov Disord 2003;5:

35
Progressive Supranuclear Palsy Core Findings
Progressive disorder Age onset > 40 Often symmetric at onset Falls in the first year Vertical supranuclear gaze palsy Dysarthria Minimal levodopa response Cognitive and behavioral problems Litvan, Mov Disord 2003;5:

36
Progressive Supranuclear Palsy
Gradually progressive parkinsonism, ≥ 40 yrs plus: Possible: vertical supranuclear palsy or slow vertical saccades + falls < 1 yr of disease onset Probable: vertical supranuclear palsy and falls < 1 yr of disease onset Definite: All criteria for possible or probable plus histopathological confirmation NINDS diagnostic criteria for PSP

38
Corticobasal Degeneration
Asymmetric Parkinsonism Other movement disorders Dystonia Stimulus sensitive myoclonus Action-postural tremor Higher cortical dysfunction Dementia Aphasia Apraxia Cortical sensory loss Alien limb syndrome

40
Parkinsonism, Heredofamiliar diseases
Ceroid lipofuscinosis Familial basal ganglia calcification (Fahr’s disease) GM1 gangliosidosis Gaucher’s disease Hallervorden Spatz disease Huntington’s disease Mitochondrial encephalopathies Chorea acanthocytosis Spinocerebellar ataxia Wilson’s disease X-linked dystonia-parkinsonism (Lubag) Premutation carriers of fragile X chromosome
 GM1 gangliosidosis. Gaucher’s disease. Hallervorden Spatz disease. Huntington’s disease. Mitochondrial encephalopathies. Chorea acanthocytosis. Spinocerebellar ataxia. Wilson’s disease. X-linked dystonia-parkinsonism (Lubag) Premutation carriers of fragile X chromosome.")
41
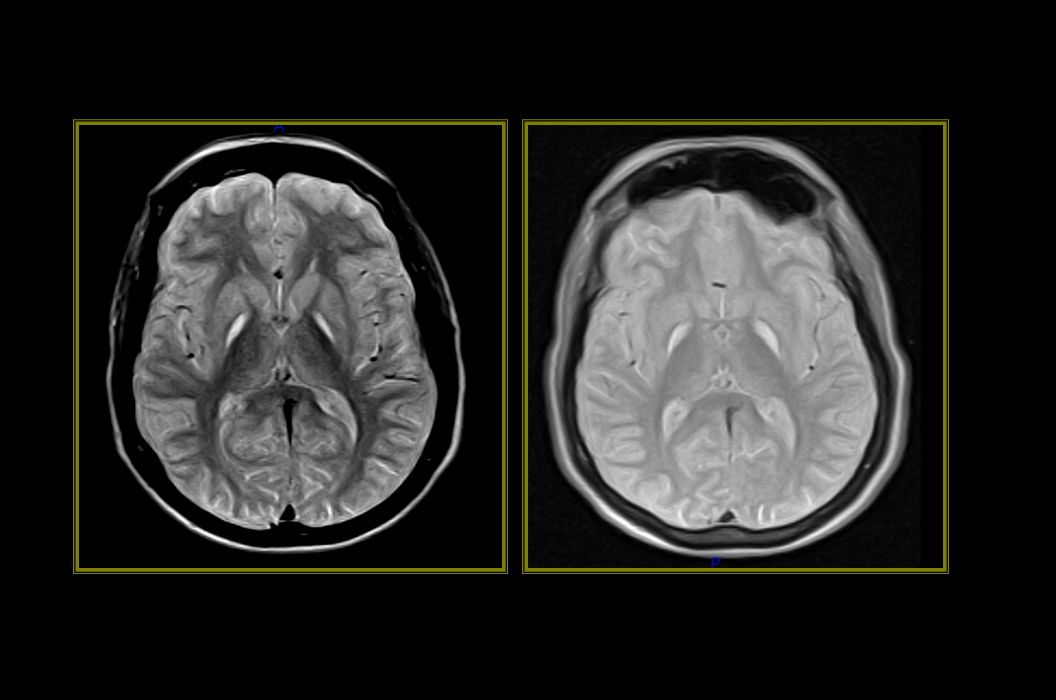
Carriers of premutation alleles (55-200 CGG)
Fragile X Premutation Carriers of premutation alleles ( CGG) Mild cognitive/behavioral deficits Premature ovarian failure Progressive tremor, ataxia, parkinsonism, autonomic dysfunction ± peripheral neuropathy, memory, executive impairment Fragile X chromosomes are characterizied by satellite regions visible at the ends of metaphase chromosomes. These are due to a long series of CGG triplet repeats, as seen in Giemsa-stained (left) and scanning electron micrograph (right) material. Fragile X is associated with Martin-Bell Syndrome, the most common form of inherited mental retardation eosinophilic intranuclear inclusions Symmetric T2 hyperintensities in MCP 1/3 of male carriers over 50 Protection due to random X inactivation of the premutation allele
 Mild cognitive/behavioral deficits. Premature ovarian failure. Progressive tremor, ataxia, parkinsonism, autonomic dysfunction ± peripheral neuropathy, memory, executive impairment. Fragile X chromosomes are characterizied by satellite regions visible at the ends of metaphase chromosomes. These are due to a long series of CGG triplet repeats, as seen in Giemsa-stained (left) and scanning electron micrograph (right) material. Fragile X is associated with Martin-Bell Syndrome, the most common form of inherited mental retardation. eosinophilic intranuclear inclusions. Symmetric T2 hyperintensities in MCP. 1/3 of male carriers over 50. Protection due to random X inactivation of the premutation allele.")
42
Children: Adults: Wilson’s Disease
tremor, dystonia, rigidity, postural instability, dysarthria, ataxia, mental/behavioral changes, seizures, sardonic smile Adults: parkinsonism, dystonia, tremor, psychiatric symptoms (1/3)
")
43
X-linked Dystonia-Parkinsonism (Lubag)
Men from the island of Panay 4th-5th decade (as early as adolescence) Parkinsonism, action tremor, dystonia Poor response to levodopa Neuronal loss in caudate, putamen, no LBs DYT3, Xq13.1
 Parkinsonism, action tremor, dystonia. Poor response to levodopa. Neuronal loss in caudate, putamen, no LBs. DYT3, Xq13.1.")
44
Juvenile Huntington’s
Very high repeat length, paternal transmission Westphal variant bradykinesia rigidity tremor dystonic posturing ataxia seizures myoclonus mental regression

45
Summary Parkinsonism is a clinically defined syndrome.
Parkinson’s disease is the most frequent cause of parkinsonism In life, defined by clinical findings No diagnostic laboratory/imaging tests Parkinsonism can occur as a part of many other disorders

Similar presentations




 (MND) are a group of neurological disorders that selectively affect motor neurons.>")

>")






>")


 A Clinical Perspective>")






