Download presentation
Presentation is loading. Please wait.

1
Falls and Fall Prevention

2
Prevalence of Falls in Older Adults 33% of older adults fall each year Falls are the leading cause of fatal and nonfatal injuries Falls rates increase with age

3
Falls Prevalence (continued) Every 15 seconds, an older adult is treated in an ER for fall-related injuries Every 29 minutes, an older adult dies from a fall
 Every 15 seconds, an older adult is treated in an ER for fall-related injuries Every 29 minutes, an older adult dies from a fall")
4
Non-fatal Fall Injuries Major cause of serious injury Most common cause of hospital admission 1.6 million older adults are treated in EDs Fall injury rates 72% higher for women than men More women are hospitalized for injuries than men

5
Fall-related Fracture Injuries Most prevalent of all fall injuries Related to osteoporosis Over 95% of hip fractures are caused by falls Hip fracture leads to hospital admission 20% of people with hip fracture die within 1 year Survivors experience significant disability

6
Costs of Falls Total cost of all fall injuries for older adults = $28.3 BILLION per year Average health care cost for fall injury = $19,440 2020 estimate is $54.9 BILLION Costs driven by hospitalization due to fractures Hip fractures most costly

7
Other “Costs” Related to Falls Disability Functional limitations Decreased productivity Reduced quality of life Fear of falling

8
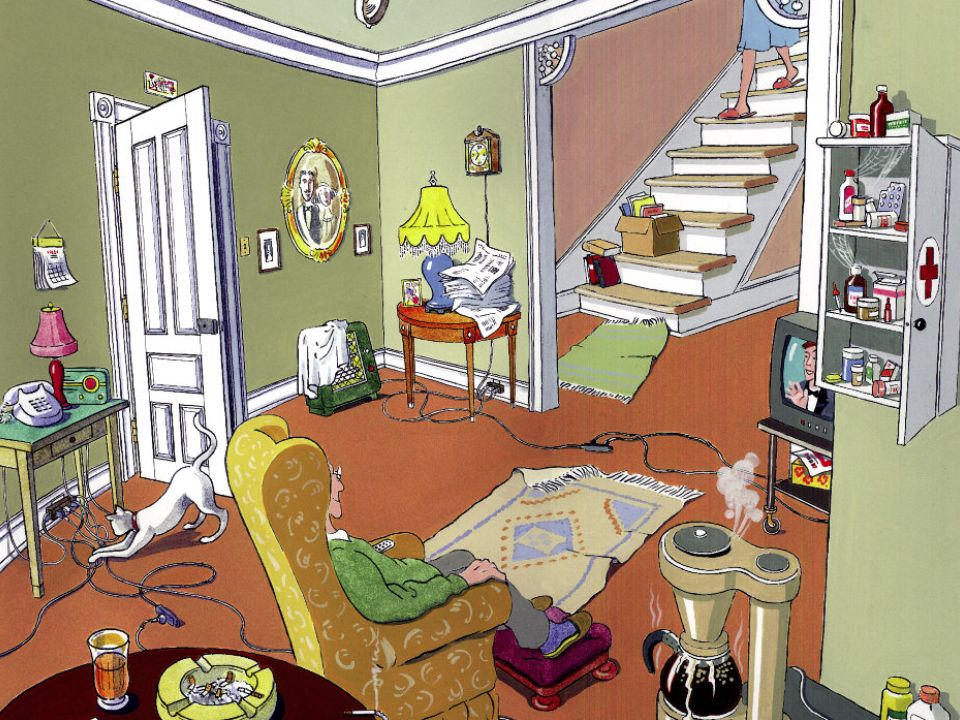
Risk Factors for Falls Personal Age Functional status Chronic conditions Environmental Fall and tripping hazards

9
Can Fall Risk Be Reduced? Non-modifiable risk Modifiable risk

10
Fall Prevention Strategies Clinical assessment and targeted risk reduction Lower risk of falling by 18% Reduced average number of falls by 43% Exercise Lower risk of falling by 12% Reduced number of falls by 19% Single most effective intervention in fall risk reduction

11
More Fall Prevention Strategies Medication management Home modifications Home safety assessment Remove fall and tripping hazards Hip protectors Multi-component strategies

13
Falls Injury Prevention Model Points of Intervention Continuum

14
Model: Falls Injury Points of Intervention Continuum Safety Promotion Support in the Community Rehabilitation Medical Care 1º & 2º Prevention

15
Safety Promotion Societal and community awareness about burden of injury from falls Take steps to reduce physical, behavioral, environmental and societal risk factors Change public values so that falls are seen as preventable

17
Primary Prevention Focus on preventing the first fall Includes: Risk identification and modification Treatment of medical illnesses Home safety/environmental modifications Physical activity to promote strength and balance

18
Secondary Prevention Aims to minimize the injury or complications once a fall occurs Prevent future falls Examples: Improving bone health to prevent fractures Personal alarm system for help Hip protectors Teaching older person how to get up from fall

19
Emergency, Primary & Acute Medical Care Goal: reduction in future morbidity and mortality and improvement of outcomes following a fall Includes: Emergency response and transport Treatment by physicians Referral for surgery & rehabilitation Correction of factors leading to the fall

20
Tertiary Prevention: Rehabilitation Aim is to maximize the level of functioning after a fall and prevent future falls Activities to prevent long-term complications and disability after a fall Address gait and balance issues, focus on strengthening lower body muscles

21
Support in the Community Post fall injury, appropriate home and medical support to enable and promote independence Examples: Community-based fall prevention program Community-based exercise program Home care services

22
Fall Prevention Programs

23
Step by Step Falls Prevention Program Goals: Enhance knowledge about falls and preventive behavior Embed falls prevention into senior centers and enhance relationships between centers and providers Focus: Physical activity and behavior modification Target: Community-dwelling older adults Located in Senior centers and facilitated by senior center staff

24
Step by Step Program Activities Falls risk assessment “Passbook” with tips on falls prevention Balance exercises Emphasized “appropriate” exercise level Program was ongoing

25
A Matter of Balance A Matter of Balance acknowledges the risk of falling but emphasizes practical coping strategies to reduce this fear, including: Promoting a view of falls and fear of falling as controllable Setting realistic goals for increasing activity Changing the environment to reduce fall risk factors Promoting exercise to increase strength and balance

26
MOB Program Goal The program’s goal is to reduce fear of falling, stop the fear of falling cycle, and increase activity levels among community-dwelling older adults.

27
MOB Program Rationale Studies indicate that up to half of community dwelling older adults experience fear of falling and that many respond to this concern by curtailing activity A majority of falls occur during routine activities Falls usually are not caused by just one issue A large portion of falls are preventable Being inactive results in loss of muscle strength and balance

28
MOB Program Focus Fear of falling can actually contribute to falling Participants learn to view falls and fear of falling as controllable and set realistic goals for increasing activity Participants find ways to change the environment and learn simple exercises to increase strength and balance The group format provides an opportunity for people with a common problem to learn from each other

29
MOB Program Components Group discussion Problem-solving Skill building Assertiveness training Exercise training Sharing practical solutions Cognitive restructuring— learning to shift from negative to positive Thinking patterns or thinking about something in a different way.

30
MOB Program Logistics Length/Timeframe of program: eight two- hour classes Recommended class size: 10-12 participants (minimum of 8, maximum of 14 ) Target population: people who are 60 or older, ambulatory, able to problem-solve, concerned about falls and interested in improving flexibility, balance, and strength
 Target population: people who are 60 or older, ambulatory, able to problem-solve, concerned about falls and interested in improving flexibility, balance, and strength")
31
MOB Desired Outcomes View falls and fear of falling as controllable Set realistic goals for increasing activity Change participants’ environment to reduce fall risk factors Increase strength and balance through exercise

32
MOB Measurement Tools Survey (given during the first class) with questions regarding falls management, exercise levels, and background information Last class survey; repeat of questions regarding falls management and exercise levels Last class evaluation with questions concerning comfort in talking about fear of falling, changes made to environment, comfort in increasing activity levels, plans to increase activity levels, and background information.
 with questions regarding falls management, exercise levels, and background information Last class survey; repeat of questions regarding falls management and exercise levels Last class evaluation with questions concerning comfort in talking about fear of falling, changes made to environment, comfort in increasing activity levels, plans to increase activity levels, and background information.")
33
MOB Results 97% of participants are more comfortable talking about fear of falling 97% feel comfortable increasing activity 99% plan to continue exercising 98% would recommend MOB (Healy, McMahon, & Haynes, 2006)
")
Similar presentations






![The National Audit of Falls and Bone Health in Older People [Speaker’s name and designation] On behalf of the Clinical Effectiveness and Evaluation Unit,](/14/4346764/big_thumb.jpg "The National Audit of Falls and Bone Health in Older People [Speaker’s name and designation] On behalf of the Clinical Effectiveness and Evaluation Unit,>")













