Download presentation
Presentation is loading. Please wait.

1
Gastro Esophageal Reflux Disease (GERD)
Dr Raed Altiti SECRETARY GENERAL OF PLAESTINIAN GASTROENTEROLOGY ASSOCIATION Jericho –Palestine 2012

2
The Montréal definition and Classification of GERD A Global Evidence-Based Consensus
What is GERD? “GERD is a condition which develops when the reflux of stomach contents causes troublesome symptoms and/or complications” The Montréal definition concludes that refluxed acidic stomach contents cause the symptoms and complications of GERD. Furthermore, the degree of troublesomeness of symptoms is one of the defining factors in a diagnosis of GERD.1 Using this patient-centred approach, GERD can therefore be diagnosed successfully in primary care on the basis of symptoms, without the need for further investigations. Vakil N et al. Am J Gastroenterol 2006; in press Vakil N et al. Am J Gastroenterol 2006;101:

3
GASTROESOPHAGEAL REFLUX DISEASE
DIAGNOSED BY 1- CLINICAL PICTURE 2-UPPER ENDOSCOPY 3- PH METRY 4- MANOMETRY? 5- The impedance metry

4
UPPER ENDOSCOPY Upper endoscopy should be the initial evaluation of suspected GERD because it provides a mechanism for detecting, stratifying, and managing the esophageal manifestations of GERD Not indicated in every patient

5
What can We Detect by EGD
1- FROM THE LARYNX 2- FROM THE ESOPHAGUS 3- FROM STOMACH

6
Laryngopharyngeal reflux, or LPR
laryngeal hyperemia posterior commissure hypertrophy. Thick endolaryngeal mucus.

8
some persons with LPR do suffer from heartburn or esophagitis (12%), most persons with LPR do not.
The reason for this is that the refluxate spends very little time in the esophagus and does most of its damage in the larynx. The anatomic abnormality in patients with LPR is thought to exist at the level of the upper esophageal sphincter

10
ESOPHAGUS NERD % so BIOPSIES ARE NEEDED GERD

11
The GERD symptom pattern is similar in patients with and without esophagitis
Heartburn (100%) Epigastric pain Regurgitation without esophagitis with esophagitis Belching Nausea 16. The GERD symptom pattern is similar in patients with and without esophagitis Regardless of the presence of esophagitis, patients with GERD have a similar pattern of symptoms, the most common of which is heartburn. This was shown by an international, multicentre study involving patients presenting in primary care because of upper gastrointestinal discomfort and who were diagnosed as having GERD. Subsequent endoscopy showed that 277 patients had esophagitis while 261 did not, but the symptom pattern was virtually the same in both groups of patients. Heartburn was present in over 90% of patients with esophagitis and in over 80% of those without esophagitis, while regurgitation, epigastric pain and belching were also present in 70–80% of patients.14 14. Carlsson R, Dent J, Watts R, Riley S, Sheikh R, Hatlebakk J et al. Gastro-oesophageal reflux disease in primary care: an international study of different treatment strategies with omeprazole. International GORD Study Group. Eur J Gastroenterol Hepatol 1998b;10:119–24. Bloating Abdominal pain Scale=% of patients with symptom Carlsson et al 1998b
 Epigastric pain. Regurgitation. without esophagitis. with esophagitis. Belching. Nausea. 16. The GERD symptom pattern is similar in patients with and without esophagitis. Regardless of the presence of esophagitis, patients with GERD have a similar pattern of symptoms, the most common of which is heartburn. This was shown by an international, multicentre study involving patients presenting in primary care because of upper gastrointestinal discomfort and who were diagnosed as having GERD. Subsequent endoscopy showed that 277 patients had esophagitis while 261 did not, but the symptom pattern was virtually the same in both groups of patients. Heartburn was present in over 90% of patients with esophagitis and in over 80% of those without esophagitis, while regurgitation, epigastric pain and belching were also present in 70–80% of patients Carlsson R, Dent J, Watts R, Riley S, Sheikh R, Hatlebakk J et al. Gastro-oesophageal reflux disease in primary care: an international study of different treatment strategies with omeprazole. International GORD Study Group. Eur J Gastroenterol Hepatol 1998b;10:119–24. Bloating. Abdominal pain. Scale=% of patients with symptom. Carlsson et al 1998b.")
12
Endoscopic Severity of GERD
Non-erosive Reflux Disease (NERD) Mild reflux esophagitis (LA grade A/B) Severe reflux esophagitis (LA grade C/D) ~1% ~10% ~30% ~30% ~60% ~70% The term gastroesophageal reflux disease therefore covers a broad range of findings. But if you look at the frequency of all these different findings in referral centers and in the community, you will see that the majority of patients with GERD have a normal esophagus on endoscopy. This is the case for 60% of patients in referral centres and 70% in the community. Around 30% of patients in both settings have mild reflux esophagitis, and severe reflux esophagitis is found in about 10% of the patients in referral centres and only 1% in the community. The frequency of Barrett's esophagus is low in the community, at around 2.5%, and in the referral centres it is between 10 and 15%. Labenz J, Malfertheiner P. World J Gastroenterol 11:4291–9 (2005) Ronkainen J et al. Scand J Gastroenterol 40:275–85 (2005) In referral center In community Labenz, Malfertheiner. World J Gastroenterol 2005 Ronkainen et al. Scand J Gastroenterol 2005 LA: Los Angeles Classification
 Mild reflux esophagitis (LA grade A/B) Severe reflux esophagitis (LA grade C/D) ~1% ~10% ~30% ~30% ~60% ~70% The term gastroesophageal reflux disease therefore covers a broad range of findings. But if you look at the frequency of all these different findings in referral centers and in the community, you will see that the majority of patients with GERD have a normal esophagus on endoscopy. This is the case for 60% of patients in referral centres and 70% in the community. Around 30% of patients in both settings have mild reflux esophagitis, and severe reflux esophagitis is found in about 10% of the patients in referral centres and only 1% in the community. The frequency of Barrett s esophagus is low in the community, at around 2.5%, and in the referral centres it is between 10 and 15%. Labenz J, Malfertheiner P. World J Gastroenterol 11:4291–9 (2005) Ronkainen J et al. Scand J Gastroenterol 40:275–85 (2005) In referral center. In community. Labenz, Malfertheiner. World J Gastroenterol Ronkainen et al. Scand J Gastroenterol LA: Los Angeles Classification.")
13
Biopsies should target any areas of suspected:
metaplasia, dysplasia, or, in the normal mucosa eosinophilic esophagitis

14
So biopsies are needed for many reasons:
1- For diagnosis of NERD 2- For excluding Esinophilic Esophagitis 3- For Diagnosis and staging of Barrett’s

15
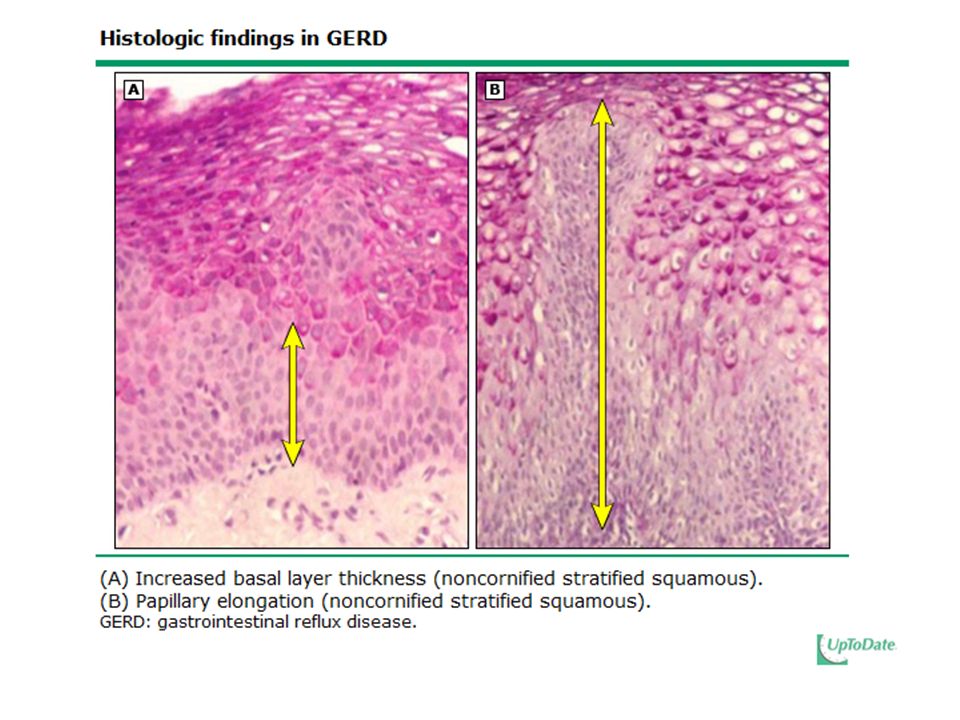
Histology . NERD =The most consistently observed histologic finding is dilation of the intercellular spaces seen on transmission electron microscopy. This finding is also present in patients with reflux esophagitis. GERD=Cellular injury stimulates cell proliferation, the morphologic equivalent of which is thickening of the basal cell layer and elongation of the papillae of the epithelium Other histologic features include the presence of neutrophils and eosinophils, dilated vascular channels in papillae of the lamina propria, and distended, pale squamous ("balloon") cells. However, none of these findings is specific for GERD.
 cells. However, none of these findings is specific for GERD.")
17
Dilated intercellular space in NERD

18
MACROSCOPICAL APEARANCE
Los Angeles classification — The Los Angeles classification grades esophagitis severity by the extent of mucosal abnormality, complications recorded separately. Grade A – one or more mucosal breaks each ≤5 mm in length Grade B – at least one mucosal break >5 mm long, but not continuous between the tops of adjacent mucosal folds Grade C – at least one mucosal break that is continuous between the tops of adjacent mucosal folds, but which is not circumferential Grade D – mucosal break that involves at least three-fourths of the luminal circumference .

28
Stricture of the esophagus

29
DEFINITION of BARRETT’S
Barrett's esophagus is the condition in which an abnormal columnar epithelium replaces the stratified squamous epithelium that normally lines the distal esophagus. It is a consequence of chronic (GERD) and predisposes to the development of adenocarcinoma of the esophagus.
 and. predisposes to the development of. adenocarcinoma of the esophagus.")
30
Barrett’s Esophagus

34
BARRETT’S CAN BE 1- With no DYSPLASIA. 2 – With low Dysplasia.
3- With high Dysplasia.

35
For patients without dysplasia, the risk of esophageal adenocarcinoma is approximately 0.5 % per year For patients with low-grade dysplasia, the risk of esophageal adenocarcinoma is approximately 0.6 % per year For patients with high-grade dysplasia, the rate of cancer development is 4 to 6 % per year.

36
WHAT WE SEE BY RETROGRADE FELXION FROM THE STOMACH

39
Ambulatory esophageal pH monitoring
Transnasally placed catheter or a wireless, capsule-shaped device that is affixed to the distal esophageal mucosa The catheter type pH electrode is positioned 5 cm above the manometrically defined upper limit of the lower esophageal sphincter. In the case of the wireless device, the pH capsule is attached 6 cm proximal to the endoscopically defined squamocolumnar junction

40
the percentage time with the intraesophageal pH below 4 as the most useful outcome measure in discriminating between physiologic and pathologic esophageal reflux

42
INDICATIONS FOR PH -METRY
1---To document abnormal esophageal acid exposure in an endoscopy-negative patient being considered for surgical antireflux repair . 2---To evaluate patients after antireflux surgery who are suspected to have ongoing abnormal reflux 3- To evaluate patients with either normal or equivocal endoscopic findings and reflux symptoms that are refractory to PPI therapy .

43
Is possibly indicated to detect refractory reflux in chest pain patients after cardiac evaluation using a symptom reflux association scheme, preferably the symptom association probability calculation . Is possibly indicated to evaluate a patient with suspected LPR manifestations (laryngitis, pharyngitis, chronic cough) of GERD after symptoms have failed to respond to at least 4 weeks of PPI therapy . possibly indicated to document concomitant GERD in an adult onset, non-allergic asthmatic suspected of having reflux induced asthma exacerbations .
 of GERD after symptoms have failed to respond to at least 4 weeks of PPI therapy . possibly indicated to document concomitant GERD in an adult onset, non-allergic asthmatic suspected of having reflux induced asthma exacerbations .")
44
Esophageal manometry Esophageal manometry should be considered in patients with symptoms of GERD and normal upper endoscopy, especially if there is any associated dysphagia, even though esophageal manometry is of minimal use in the diagnosis of GERD. Useful in identifying alternative diagnoses such as achalasia, the symptoms of which sometimes closely mimic those of GERD . The evaluation of peristaltic function to exclude major motor disorders is also important before antireflux surgery, and it can also be used to ensure that ambulatory pH probes are placed correctly .

45
Combined Multichannel intraluminal impedance and pH testing
All patients with persistent GERD symptoms despite PPI therapy require multichannel intraluminal impedance and pH testing. Combined multichannel intraluminal impedance and pH (MII-pH) monitoring is based upon detection of changes in resistance to electrical currents. retrograde bolus movement causes the electrical resistance changes
 monitoring is based upon detection of changes in resistance to electrical currents. retrograde bolus movement causes the electrical resistance changes.")
47
This techinc provides information on:
The number of acid and non-acid reflux episodes Number of liquid, gas, and mixed reflux episodes Proximal extent of reflux episodes Bolus contact time (ie, percentage of time bolus was present at 5 cm above the lower esophageal sphincter [LES]) Acid contact time (ie, percentage of time pH <4.0 at 5 cm above the LES)
 Acid contact time (ie, percentage of time pH <4.0 at 5 cm above the LES)")
48
CONTINUE TO BE PATIENT RR

49
WHY NO RESPONSE Differences in Bioavailability (change the drugs) Food
Differences in metabolism gentetic (change the drug) Dose interval (split the dose) Gastric acid secretion Esphageal hypersensitivity (increase the dose) Esinophillic esophagitis Bilereflux (considere sucralfate ) Other drugs
 Dose interval (split the dose) Gastric acid secretion. Esphageal hypersensitivity (increase the dose) Esinophillic esophagitis. Bilereflux (considere sucralfate ) Other drugs.")
50
Medical therapy is the first line of management for GERD.
+++Esophagitis will heal in approximately 90% of cases with intensive medical therapy. ---- medical management does not address the etiology; thus symptoms recur in more than 80% of cases within one year of drug withdrawals. ---- mucosal injury may continue due to ongoing alkaline reflux . ----may be required for life.

51
----The cost ----Psychological burden of a life time of medication dependence, ----Undesirable life style changes, Chronic medical management may be most appropriate for patients with limited life expectancy or comorbid conditions which would prohibit safe surgical intervention. young people.

52
"Long-term control of chronic GERD can be very effectively obtained with either maintenance esomeprazole or laparoscopic antireflux surgery, "Both treatments are safe and well tolerated."

53
Proton pump inhibitors (PPIs) are just as effective as laparoscopic surgery for patients with chronic gastroesophageal reflux disease, results of a multicenter clinical trial suggest. After five years of follow-up, 92% of patients treated with the PPI esomeprazole remained in remission, compared with 85% of patients who had antireflux surgery. But clinical relevance is questionable

54
SURGERY The most frequent indication for antireflux surgery has traditionally been severe GERD unresponsive to optimal medical therapy, which consists of both drug therapy and lifestyle modifications .

55
Surgical management of gastroesophageal reflux in adults
Gastrointestinal indications Failed optimal medical management Noncompliance with medical therapy High volume reflux Severe esophagitis by endoscopy Benign stricture Barrett's columnar-lined epithelium (without severe dysplasia or carcinoma)
")
56
Non gastrointestinal indications
About one-half of patients with GERD report upper respiratory symptoms including hoarseness, laryngitis, wheezing, nocturnal asthma, cough, aspiration, or dental erosion . Relief of respiratory symptoms is usually achievable by fundoplication in patients who also have typical reflux symptoms; however, the outcome is less favorable in the substantial minority of patients in whom respiratory symptoms occur in association with abnormalities of esophageal motility

57
Asthma Consensus has not been achieved on the role of surgery in patients with asthma that is thought to be related to GERD. A systematic review that included 24 reports (mostly case series and uncontrolled trials) suggested that surgery improved asthma symptoms in 79 , asthma medication use 88, and pulmonary function in, 27 percent of patient. A dramatic reduction in steroid dependency postoperatively was documented in another study . Medical therapy is associated with an improvement in symptoms and reduction in asthma medication use in 60 to 70 percent of patients . Improvement in pulmonary function has not been documented after medical or surgical therapy .
 suggested that surgery improved asthma symptoms in 79 , asthma medication use 88, and pulmonary function in, 27 percent of patient. A dramatic reduction in steroid dependency postoperatively was documented in another study . Medical therapy is associated with an improvement in symptoms and reduction in asthma medication use in 60 to 70 percent of patients . Improvement in pulmonary function has not been documented after medical or surgical therapy .")
58
Laryngeal disease There is no role for considering surgery as a first-line treatment for posterior laryngitis. However, it is reasonable to consider surgery for patients who have abnormal pharyngeal acid on a double probe pH study when medical therapy has been maximized, is not tolerated, or is impractical.

59
A controlled trial suggested that surgery was not consistently effective in patients who were unresponsive to aggressive PPI therapy ; thus, failure to respond to a PPI should serve as a warning that symptoms may not be relieved with surgery

60
What to do for refractory cases
CONSIDER OTHER DIAGNOSIS or GERD complications Split the doses Increase the dose Use compound therapy Change the drug surgery

Similar presentations



















 has Barrett’s esophagus diagnosed on upper endoscopy. Which of.>")









, FRACP. SHAKESPEARE SPECIALIST GROUP MILFORD, AUCKLAND.>")


>")




