Download presentation
Presentation is loading. Please wait.

1
Straightening the mast might not improve getting the wind in the sails Sean Haloman, R1

2
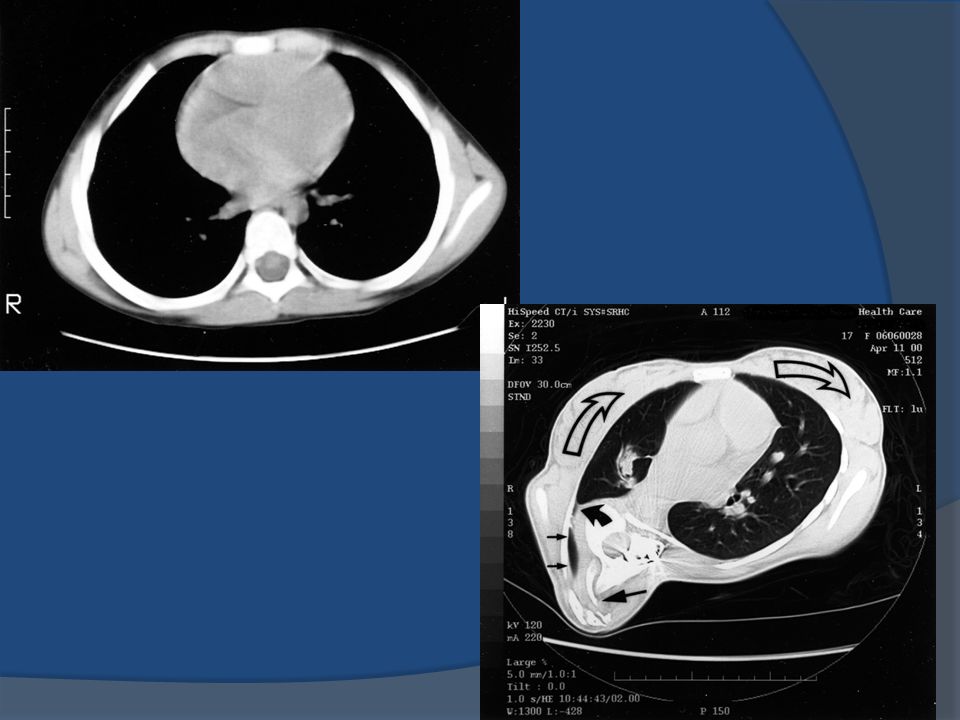
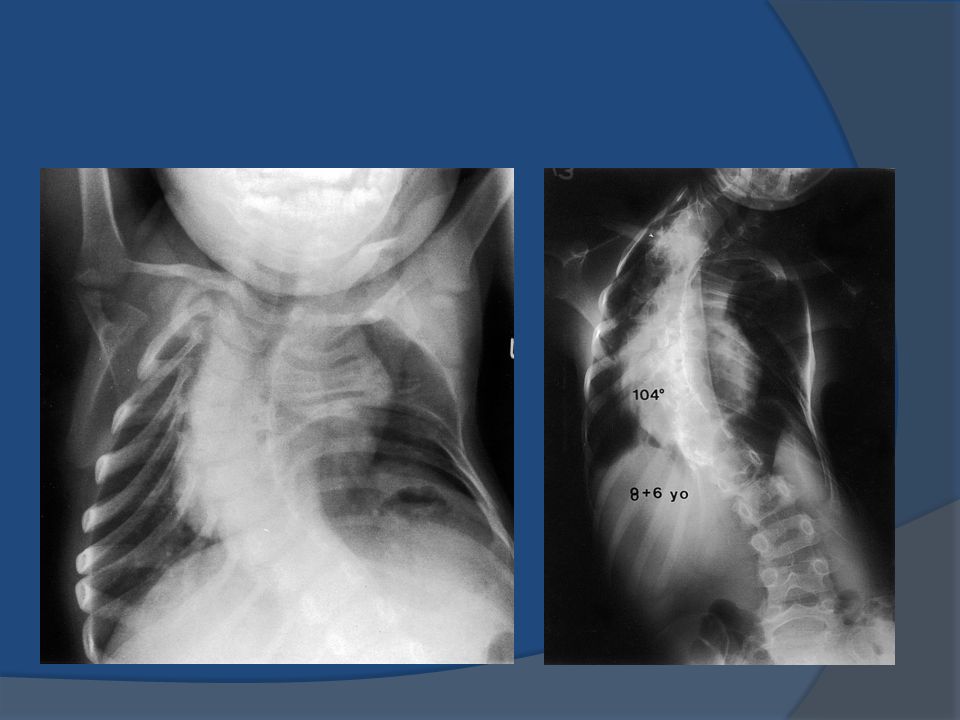
Thoracic Insufficiency Syndrome Inability of thorax to support normal respiratory function or lung growth Causes- Fused ribs Congenital scoliosis Early onset scoliosis Normal thorax has 2 key characteristics Normal volume (height, width, depth) Ability to change that volume
 Ability to change that volume")
3
Thoracic Insufficiency Diagnosed based on: Clinical signs of respiratory insufficiency Loss of chest wall mobility Worsening indices of three dimensional deformity Relative decline in percent predicted vital capacity All have potential to develop: Respiratory Failure Pulmonary HTN R ventricular failure Cor pulmonale

5
Previous treatment Spinal fusion to prevent further curve progression Little attention paid to lung function or Growth of lung and thoracic cavity

8
The History of VEPTR Designed by Dr. Robert Campbell Been in use since 1989 in San Antonio Introduced in Europe in 2002

9
J Bone Joint Surg. 2004;86A:51-64.

10
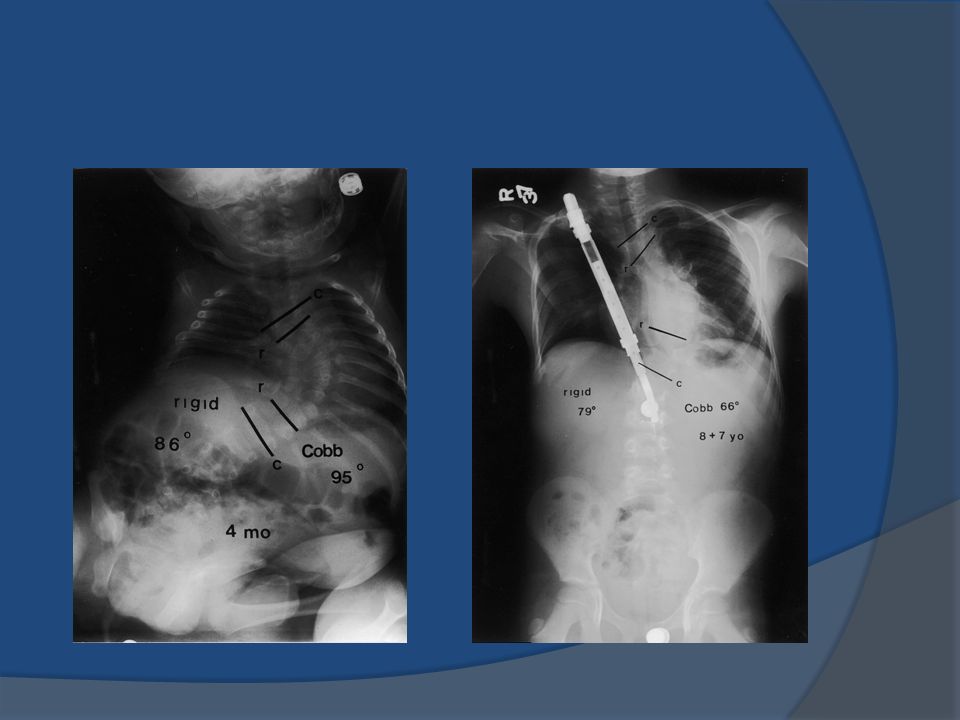
Goal of Treatment Acute increase in thoracic volume Correction of any flail chest abnormalities Maintain these improvements as the patient grows Avoid spinal fusion prior to skeletal maturity

12
Campbell et al 27pts with fused ribs and congenital scoliosis followed for 5.7 years ○ Mean age at initial procedure 3.2 yrs ○ Mean progression of curvature was 15°/ yr

13
Outcomes: Spine curvature

16
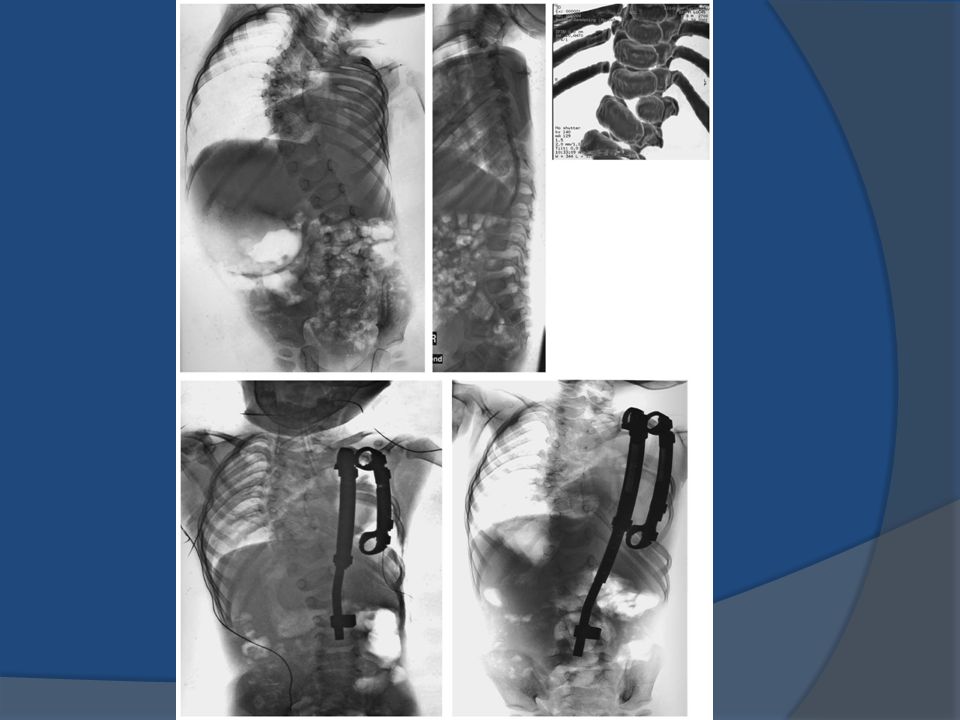
Basel, Switzerland n=15; mean age of 6; seven girls, eight boys 6 w/ neuromuscular scoliosis ○ Secondary TIS All others had severe congenital scoliosis with chest wall deformity

17
Results Subjective ○ Families reported increased playing and sport activities ○ Better sitting abilities in neuromuscular patients ○ Improved cosmesis Objective ○ Cobb angle: Before 76 °, After 55 ° ○ Pelvic Obliquity: reduced by 10 degrees ○ Height of hemithorax changed from 78% to 94%

20
Retrospective, excluded congenital vertebral anomalies and rib fusions 23 children Hasler et al

21
Pre-Op Average Post-Op Average Final Follow- up Coronal Cobb Angle 68° (11° -111° )48° (10° -86° )54° (0° -105° ) Pelvic Obliquity33° (13-60° )14° (1-41° )16° (0-42° )
48° (10° -86° )54° (0° -105° ) Pelvic Obliquity33° (13-60° )14° (1-41° )16° (0-42° )")
22
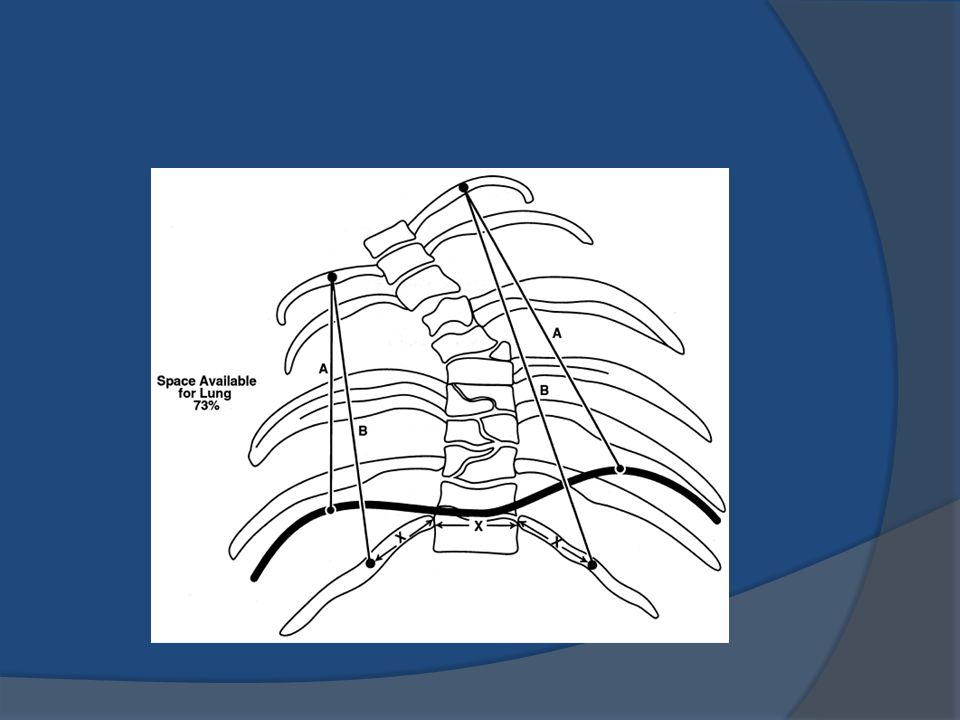
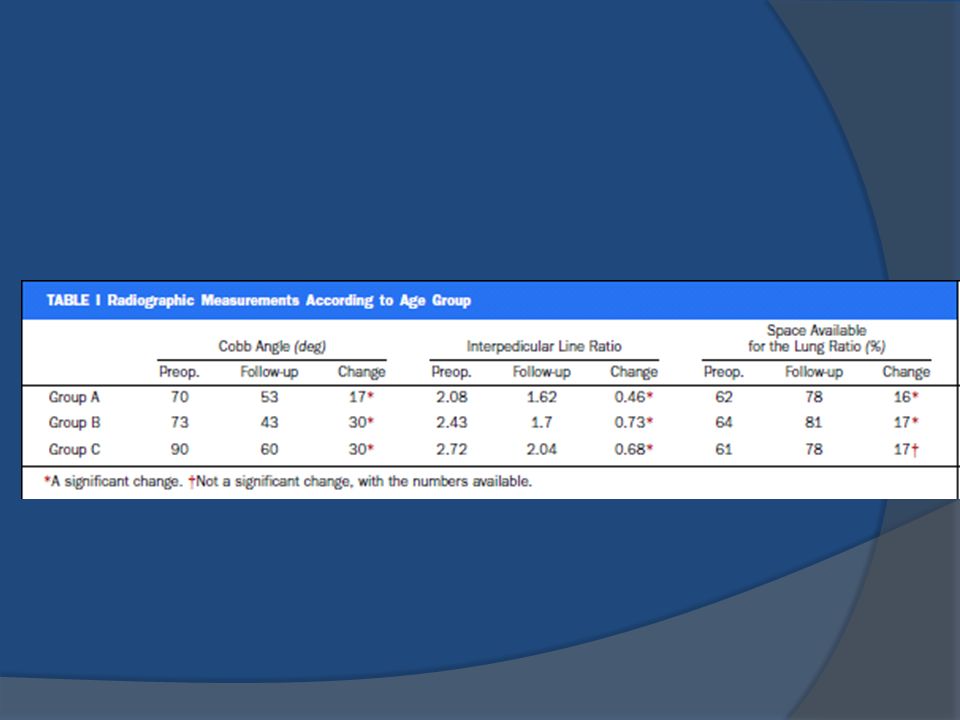
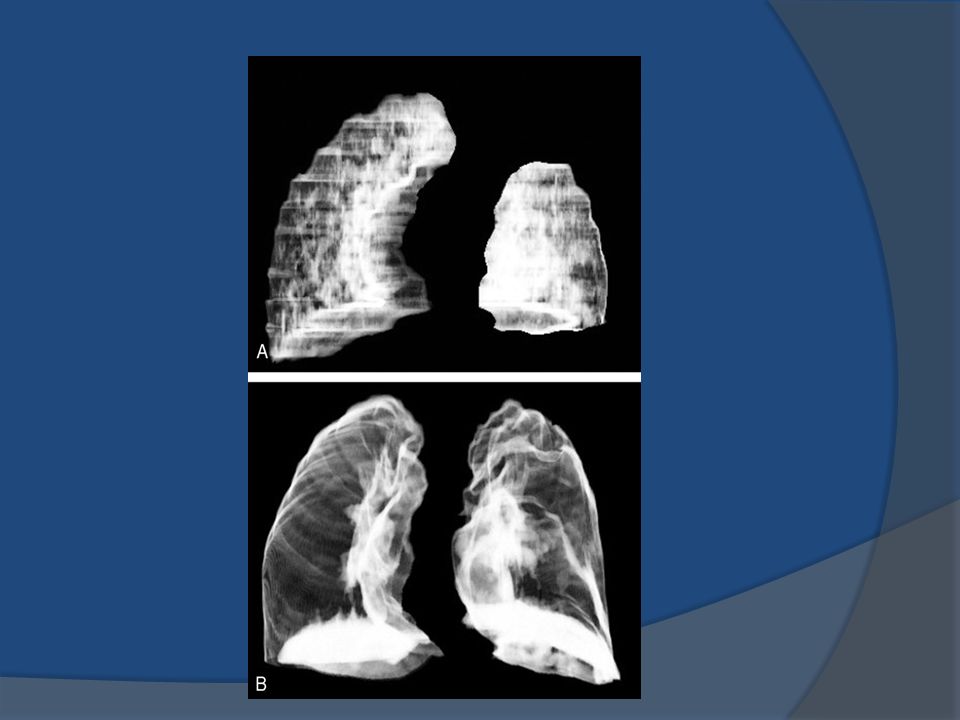
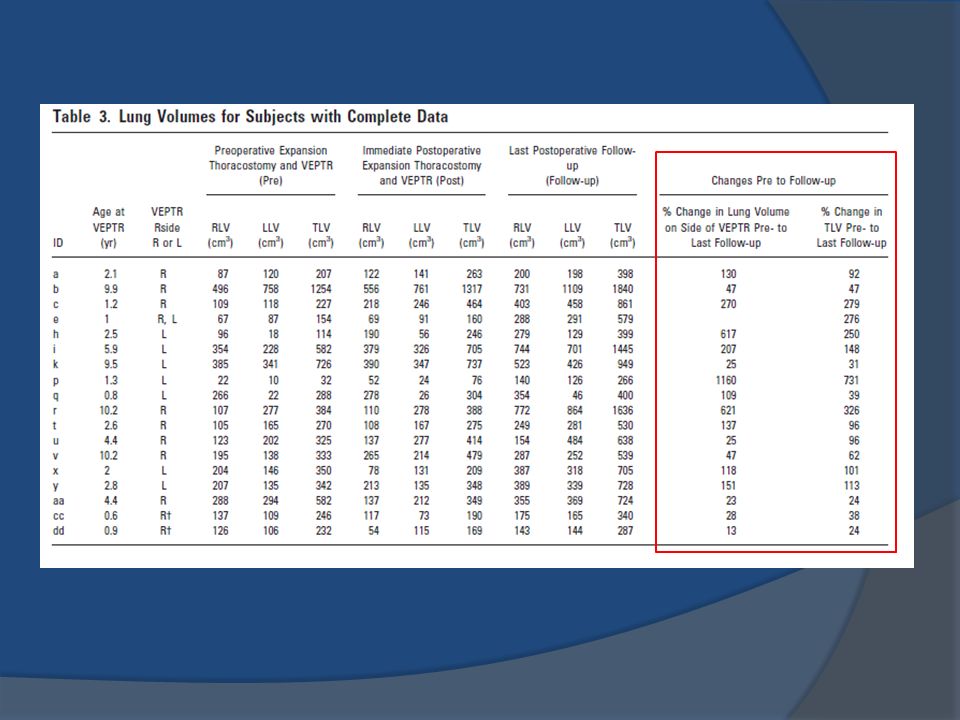
Emans et al 31 patients, mean age 4.2 years, mean f/u 2.6yrs Outcomes ○ Thoracic spine length (via CT scan) Increased on average by 2.3cm ○ Growth 1.2 cm/yr ○ Curve 55° 39° 43° (last f/u) ○ Lung Volumes (18 of 30 pts had complete set CT exams) 369cm 3 736cm 3 Mean increase in lung volumes for unilateral VEPTR was 219cm 3
 Increased on average by 2.3cm ○ Growth 1.2 cm/yr ○ Curve 55° 39° 43° (last f/u) ○ Lung Volumes (18 of 30 pts had complete set CT exams) 369cm 3 736cm 3 Mean increase in lung volumes for unilateral VEPTR was 219cm 3")
26
Interval PFTs (16 of 22pts) ~3yr f/u Group A: ○ VC 0.51L 0.72L ○ Percent predicted 50.7% 53% Group B: ○ VC 0.69L 0.98L ○ PPV 44% 45%
 ~3yr f/u Group A: ○ VC 0.51L 0.72L ○ Percent predicted 50.7% 53% Group B: ○ VC 0.69L 0.98L ○ PPV 44% 45%")
28
Motomoya et al Immediate effects of VEPTR ○ No change in FVC or Lung compliance ○ Stiff parietal pleura? Long-term effects of repeated expansion ○ FVC in absolute values increased in most pts at an average annual rate of 26.8% (similar to normal rate increases in lung volumes) ○ FVC in relation to percent predicted values showed no improvement ○ Lung compliance also did not improve No correlation between improvement in Cobb angles versus indices of lung volumes and function
 ○ FVC in relation to percent predicted values showed no improvement ○ Lung compliance also did not improve No correlation between improvement in Cobb angles versus indices of lung volumes and function.")
29
© 2006 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc.2 Table 2 Effects on Lung Function of Multiple Expansion Thoracoplasty in Children With Thoracic Insufficiency Syndrome: A Longitudinal Study. Motoyama, Etsuro; Deeney, Vincent; Fine, Gavin; MBBS, BCh; Yang, Charles; Mutich, Rebecca; BS, RT; Walczak, Stephen; BS, RRT; Moreland, Morey Spine. 31(3):284-290, February 1, 2006. DOI: 10.1097/01.brs.0000197203.76653.d0 Table 2 Pulmonary Function Results
: , February 1, DOI: /01.brs d0 Table 2 Pulmonary Function Results.")
30
© 2006 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc.3 Figure 4 Effects on Lung Function of Multiple Expansion Thoracoplasty in Children With Thoracic Insufficiency Syndrome: A Longitudinal Study. Motoyama, Etsuro; Deeney, Vincent; Fine, Gavin; MBBS, BCh; Yang, Charles; Mutich, Rebecca; BS, RT; Walczak, Stephen; BS, RRT; Moreland, Morey Spine. 31(3):284-290, February 1, 2006. DOI: 10.1097/01.brs.0000197203.76653.d0 Figure 4. Longitudinal changes in FVC (in liters on the y- axis) with multiple VEPTR expansion thoracoplasties in 10 children with TIS. The duration of the study is shown on the x-axis. As a group, there was a significant increase in FVC over time (P < 0.01).
: , February 1, DOI: /01.brs d0 Figure 4. Longitudinal changes in FVC (in liters on the y- axis) with multiple VEPTR expansion thoracoplasties in 10 children with TIS. The duration of the study is shown on the x-axis. As a group, there was a significant increase in FVC over time (P < 0.01)..")
31
© 2006 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc.4 Figure 5 Effects on Lung Function of Multiple Expansion Thoracoplasty in Children With Thoracic Insufficiency Syndrome: A Longitudinal Study. Motoyama, Etsuro; Deeney, Vincent; Fine, Gavin; MBBS, BCh; Yang, Charles; Mutich, Rebecca; BS, RT; Walczak, Stephen; BS, RRT; Moreland, Morey Spine. 31(3):284-290, February 1, 2006. DOI: 10.1097/01.brs.0000197203.76653.d0 Figure 5. Longitudinal changes in FVC (expressed as percent predicted values on the y-axis) with multiple VEPTR expansion thoracoplasties in 10 children with TIS. As a group, there was no significant change in the percent predicted values of FVC over time.
: , February 1, DOI: /01.brs d0 Figure 5. Longitudinal changes in FVC (expressed as percent predicted values on the y-axis) with multiple VEPTR expansion thoracoplasties in 10 children with TIS. As a group, there was no significant change in the percent predicted values of FVC over time..")
32
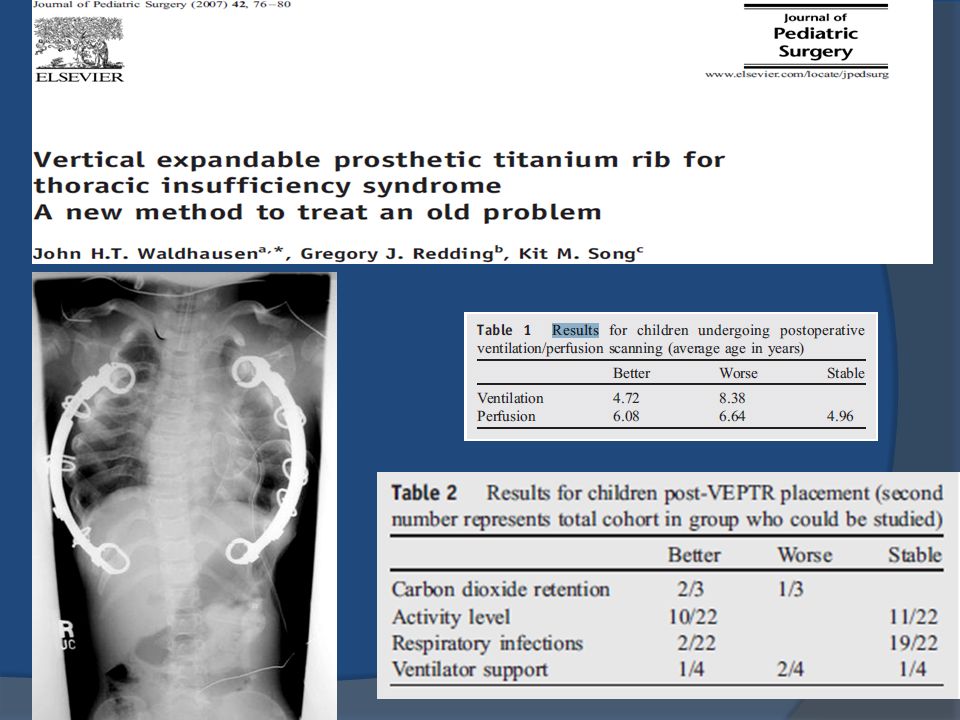
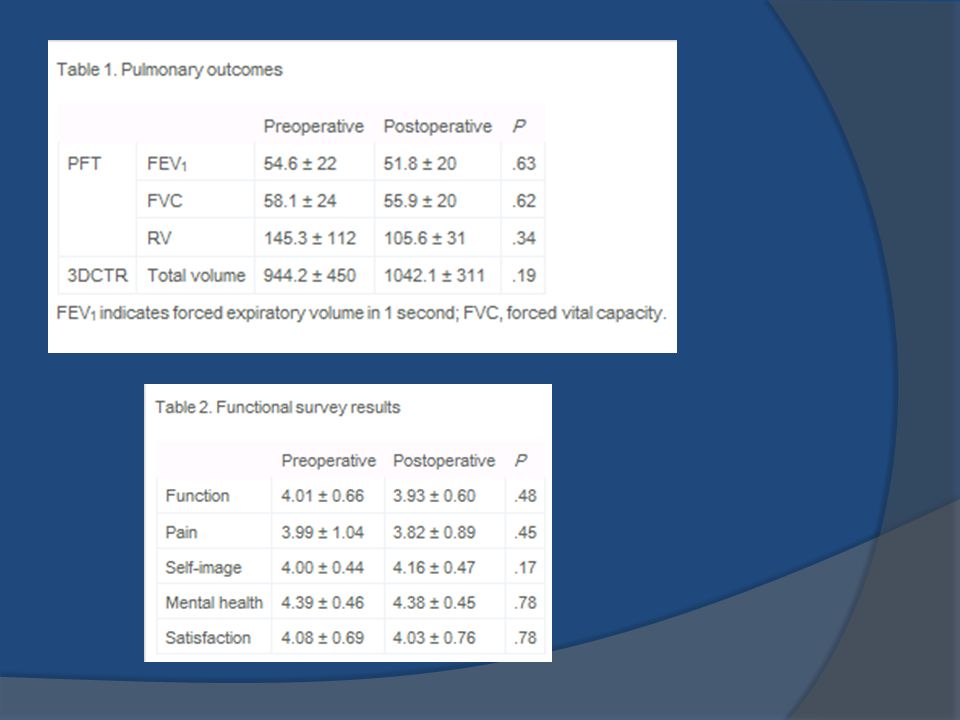
Gadepalli et al 26 pts, 29 insertions, 57 expansions; prospective ○ Age ~91months (increased age pool) measures 3D CT scans, PFTs, Scoliosis Research Society scores Cobb angle improvement from ave of 64.7 to 58.1 SRS-22; no improvement (normal function before and after) PFTs, no improvement Total lung volume corrected for age, no improvement
 measures 3D CT scans, PFTs, Scoliosis Research Society scores Cobb angle improvement from ave of 64.7 to 58.1 SRS-22; no improvement (normal function before and after) PFTs, no improvement Total lung volume corrected for age, no improvement")
34
Discussion Difficult to perform PFTs in this population Small numbers No control groups Comparing different patient populations

35
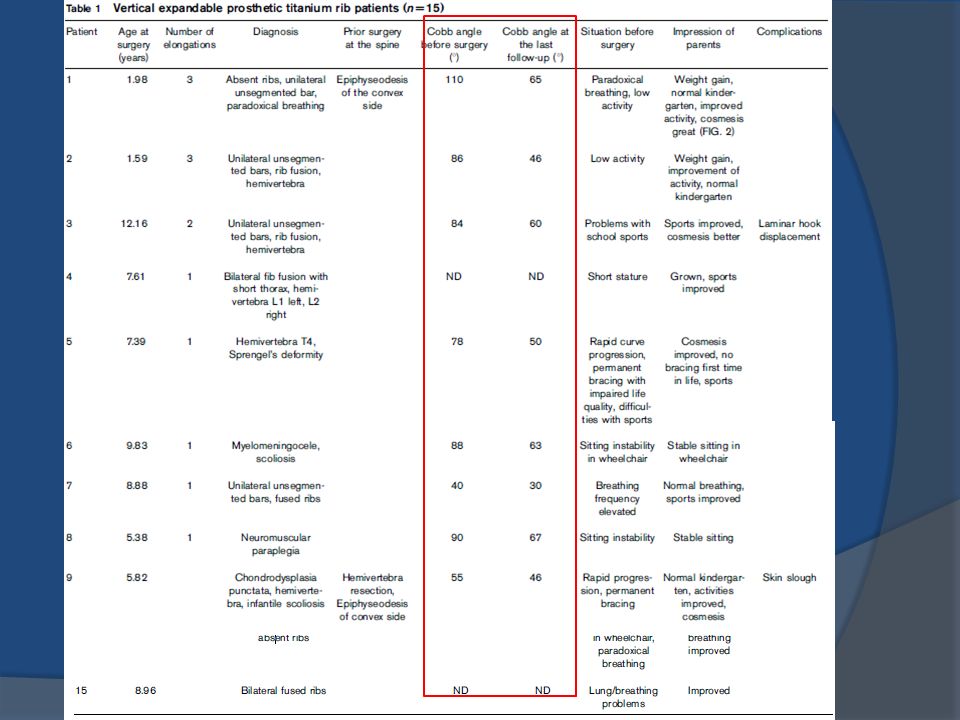
Thank you! The vertical expandable prosthetic titanium rib implant for the treatment of thoracic insufficiency syndrome associated with congenital and neuromuscular scoliosis in young children. Hell, Anna; Campbell, Robert; Hefti, Fritz Journal of Pediatric Orthopaedics B. 14(4):287-293, July 2005.
: , July")
36
Bibliography R.M. Campbell, M.D. Smith, T.C. Mayes et al.The characteristics of thoracic insufficiency syndrome associated with fused ribs and congenital scoliosis. J Bone Joint Surg, 85A (2003), pp. 399–408 John H.T. Waldhausen, Gregory J. Redding, Kit M. Song, Vertical expandable prosthetic titanium rib for thoracic insufficiency syndrome: A new method to treat an old problem, Journal of Pediatric Surgery, Volume 42, Issue 1, January 2007, Pages 76-80. Hell AK, Campbell RM, Hefti F. The vertical expandable prosthetic titanium rib implant for the treatment of thoracic insufficiency syndrome associated with congenital and neuromuscular scoliosis in young children. J Pediatr Orthop B 2005;14:287-293 Effects on Lung Function of Multiple Expansion Thoracoplasty in Children With Thoracic Insufficiency Syndrome: A Longitudinal Study. Motoyama, Etsuro; Deeney, Vincent; Fine, Gavin; MBBS, BCh; Yang, Charles; Mutich, Rebecca; BS, RT; Walczak, Stephen; BS, RRT; Moreland, Morey Spine. 31(3):284-290, February 1, 2006. Samir K. Gadepalli, Ronald B. Hirschl, Wan C. Tsai, Michelle S. Caird, Kelly L. Vanderhave, Peter J. Strouse, Robert A. Drongowski, Frances A. Farley, Vertical expandable prosthetic titanium rib device insertion: does it improve pulmonary function?, Journal of Pediatric Surgery, Volume 46, Issue 1, January 2011, Pages 77-80, ISSN 0022-3468, 10.1016/j.jpedsurg.2010.09.070. Campbell RM Jr, Smith MD, Mayes TC, et al. The effect of opening wedge thoracostomy on thoracic insufficiency syndrome associated with fused ribs and congenital scoliosis. J Bone Joint Surg Am 2004;86:1659–74. Emans JB, Caubet JF, Ordonez CL, Lee EY, Ciarlo M (2005) The treatment of spine and chest wall deformities with fused ribs by expansion thoracostomy and insertion of vertical expandable prosthetic titanium rib: growth of thoracic spine and improvement of lung volumes. Spine 30:S58–S68
, pp. 399–408 John H.T. Waldhausen, Gregory J. Redding, Kit M. Song, Vertical expandable prosthetic titanium rib for thoracic insufficiency syndrome: A new method to treat an old problem, Journal of Pediatric Surgery, Volume 42, Issue 1, January 2007, Pages Hell AK, Campbell RM, Hefti F. The vertical expandable prosthetic titanium rib implant for the treatment of thoracic insufficiency syndrome associated with congenital and neuromuscular scoliosis in young children. J Pediatr Orthop B 2005;14: Effects on Lung Function of Multiple Expansion Thoracoplasty in Children With Thoracic Insufficiency Syndrome: A Longitudinal Study. Motoyama, Etsuro; Deeney, Vincent; Fine, Gavin; MBBS, BCh; Yang, Charles; Mutich, Rebecca; BS, RT; Walczak, Stephen; BS, RRT; Moreland, Morey Spine. 31(3): , February 1, Samir K. Gadepalli, Ronald B. Hirschl, Wan C. Tsai, Michelle S. Caird, Kelly L. Vanderhave, Peter J. Strouse, Robert A. Drongowski, Frances A. Farley, Vertical expandable prosthetic titanium rib device insertion: does it improve pulmonary function , Journal of Pediatric Surgery, Volume 46, Issue 1, January 2011, Pages 77-80, ISSN , /j.jpedsurg Campbell RM Jr, Smith MD, Mayes TC, et al. The effect of opening wedge thoracostomy on thoracic insufficiency syndrome associated with fused ribs and congenital scoliosis. J Bone Joint Surg Am 2004;86:1659–74. Emans JB, Caubet JF, Ordonez CL, Lee EY, Ciarlo M (2005) The treatment of spine and chest wall deformities with fused ribs by expansion thoracostomy and insertion of vertical expandable prosthetic titanium rib: growth of thoracic spine and improvement of lung volumes. Spine 30:S58–S68.")
Similar presentations





 Emma Orton BME 281.>")






 alerts during implantation of rib based growing constructs did not sustain neurologic injury during.>")






