Download presentation
Presentation is loading. Please wait.

1
Chest pain, angina and AF Dr Peter Scott Royal Bolton Hospital

2
Some epidemiology regarding chest pain 1-2% of primary care consultations 15-25% of 999 calls 5-20% of A&E visits

3
Aetiology of chest pain depending on clinical setting GP surgery A&E dept Cardiac 20% 45% Musculoskeletal 43% 14% Pulmonary 4% 5% GI 5% 6% Psychiatric 11% 8% Other 17% 22%

4
Is this cardiac pain?

5
Likelihood of chest pain being cardiac History (typical vs atypical) Risk factors male sex, age, previous IHD, other arterial disease, diabetes, hypertension, smoking, +ve FH Examination ECG findings
 Risk factors male sex, age, previous IHD, other arterial disease, diabetes, hypertension, smoking, +ve FH Examination ECG findings")
6
Clinical assessment: history Cause of pain Type of pain Referred pain Response to posture and or movement Response to Food or fluid Tenderness Ischaemic cardiac VisceralYesNo Non ischaemic cardiac VisceralYesYes/noNo Pulmonary disease Visceral/ cutaneous Usually noNo PneumothoraxVisceral/ cutaneous NoYesNoNo/yes MusculoskeletalCutaneousNoYesNoYes GastrointestinalVisceralSometimesNoYesNo Aortic dissectionVisceralYesNo PsychiatricVisceral/ cutaneous No No/yes

7
Typical ischaemic pain Increases in intensity Central/across chest Radiation to jaw/left arm Heavy/squeezing/crushing/tight Occ. burning Sweating/nausea/faintness

8
Atypical presentations of CAD (20-30% of cases) 20-40 yrs old >75 yrs Diabetics Women Stabbing pain Epigastric pain Radiation to back Dyspnoea predominant
 yrs old >75 yrs Diabetics Women Stabbing pain Epigastric pain Radiation to back Dyspnoea predominant")
9
Clinical features making ischaemia unlikely Pain affected by -palpation -breathing -turning/twisting -bending Pain localised to one spot Pain generated from multiple sites

10
Examination findings making ischaemia likely Physical examination usually normal Transient (ischaemic induced) MR Hypotension LVF (gallop rhythm, crackles)
 MR Hypotension LVF (gallop rhythm, crackles)")
11
ECG findings making ischaemia likely ST elevation/depression New T wave inversion Fixed Q waves Repolarisation changes that are not new Arrhythmias (ischaemic induced)
")
12
ECG in chest pain assessment: Important things to remember Most valuable if recorded when symptomatic 30% of patients presenting with cardiac chest pain will have normal initial ECG 2-4% of patients discharged from A&E because of normal ECG and atypical symptoms have evolving MI 30% of patients with T wave inversion will have normal coronary arteries at angiography

13
American Heart Association scheme for estimating the probability of unstable angina FeatureHigh probability Intermediate probability Low probability HistorySymptoms identical to previous ischaemic pain Known IHD Typical chest or arm pain Age >70yrs Male sex Diabetes Possible ischaemic pain in the absence of high or intermediate risk features ExaminationTransient MR Hypotension LVF PVD or CVD Arterial bruits Chest discomfort reproduced by palpation ECG findings ST depression New T wave inversion Fixed Q waves Old ST/T wave changes T wave flattening or inversion in leads with dominant R waves Normal

14
Non ischaemic causes of chest pain Oesophageal Pulmonary embolism Hyperventilation Pneumothorax Aortic dissection Pericarditis Costochondritis Shingles Ectopic beats Other GI causes (peptic ulcer, biliary colic, cholecystitis, pancreatitis) Depression Alcohol related
 Depression Alcohol related")
15
Chest Pain: Practical aspects: New onset possible cardiac chest pain at rest <72 hrs ago: *Admit for further assessment Possible cardiac chest pain >72 hrs ago: *ECG evidence of recent cardiac event (new Q waves/T wave inversion) and ongoing chest pain: Admit. No further pain: Start Aspirin/B.Blocker and Statin and arrange urgent cardiology appt. *Normal ECG but ongoing chest pain: Consider admission. No further pain: Start Aspirin/B.Blocker and refer to Rapid Access chest pain clinic. Symptoms of exertional angina: *Refer to Rapid Access chest pain clinic

18
Most stable angina is produced by fixed coronary stenosis +/- varying degrees of vasoconstriction

19
Management of patients with symptoms of exertional angina Start Aspirin and prophylactic GTN Add B.Blocker if marked symptoms Refer to Rapid Access chest pain clinic

20
Role of Rapid Access Clinic Assess likelihood of chest pain symptoms being of cardiac origin Assess potential severity of CAD in subjects with exertional angina

21
Cardiac assessment Exercise ECG: normal resting ECG and subject capable of reasonable physical exertion Stress echo or myocardial perfusion scanning: abnormal resting ECG, subject unable to exercise adequately, equivocal exercise ECG Cardiac CT: ?subjects with chest pain and low risk of CAD

22
CT coronary angiography

23
Atrial fibrillation Is the commonest sustained cardiac arrhythmia Lone AF accounts for approx. 30% of cases

24
ATRIAL FIBRILLATION

25
Atrial fibrillation - causes Hypertensive heart disease IHD – acute or previous MI Rheumatic heart disease Sinus node disease Cardiomyopathy Thyrotoxicosis Ethanol abuse COPD/cor pulmonale/pulmonary embolism Recent surgery (esp cardiac) Constrictive pericarditis
 Constrictive pericarditis")
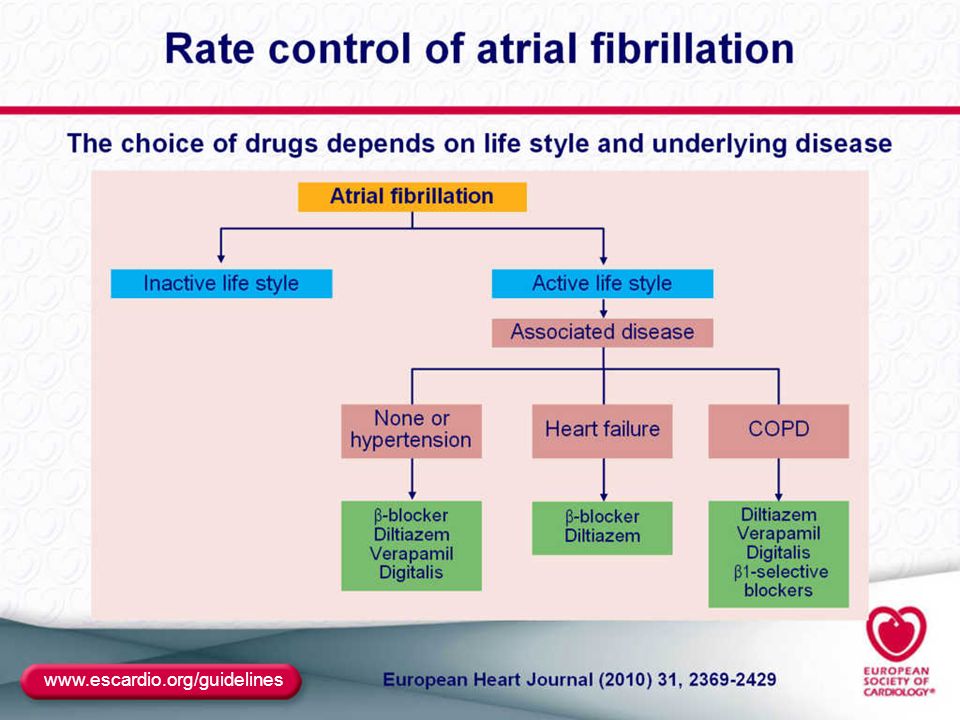
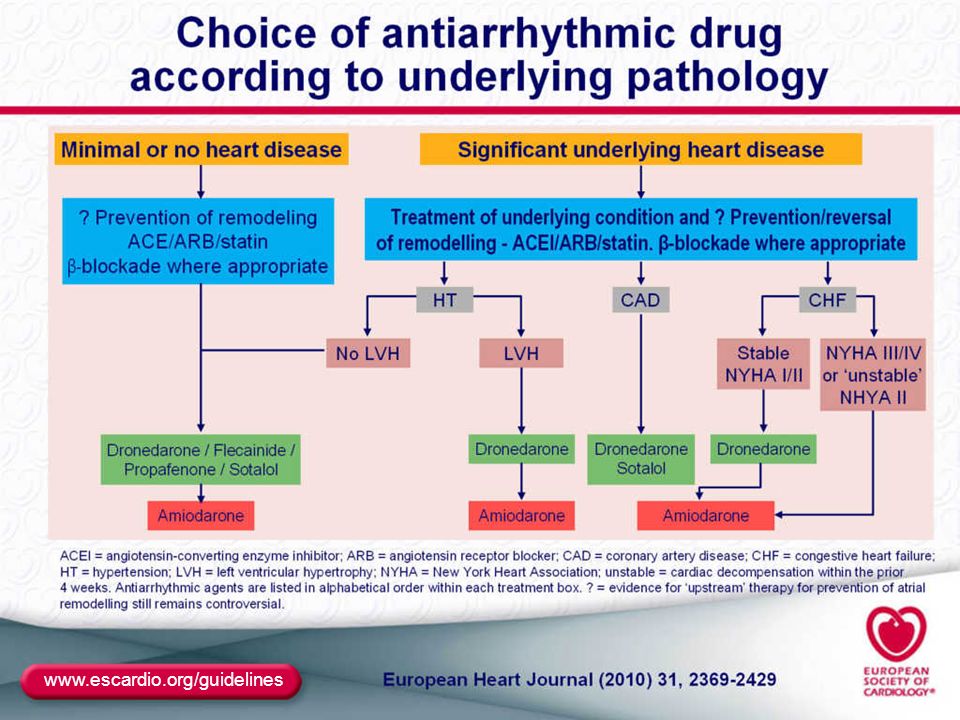
26
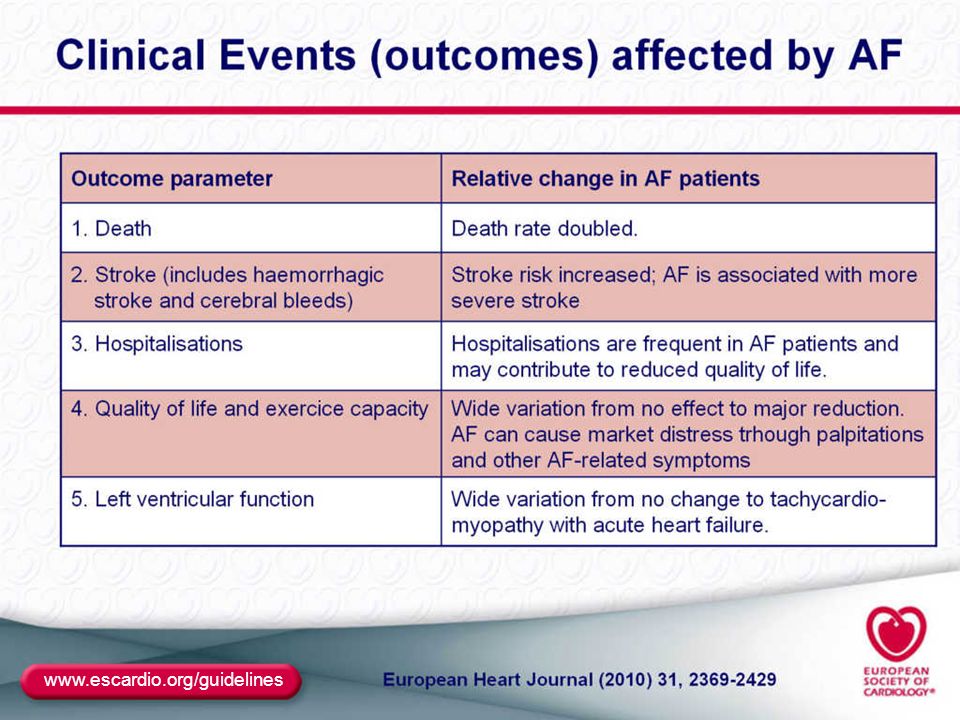
www.escardio.org/guidelines
40
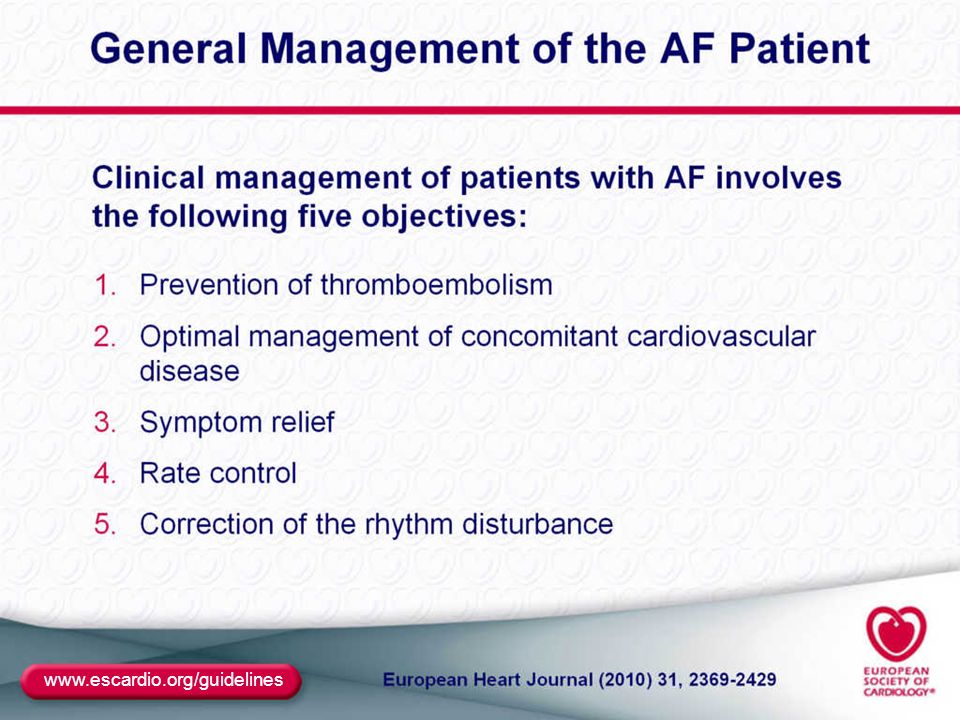
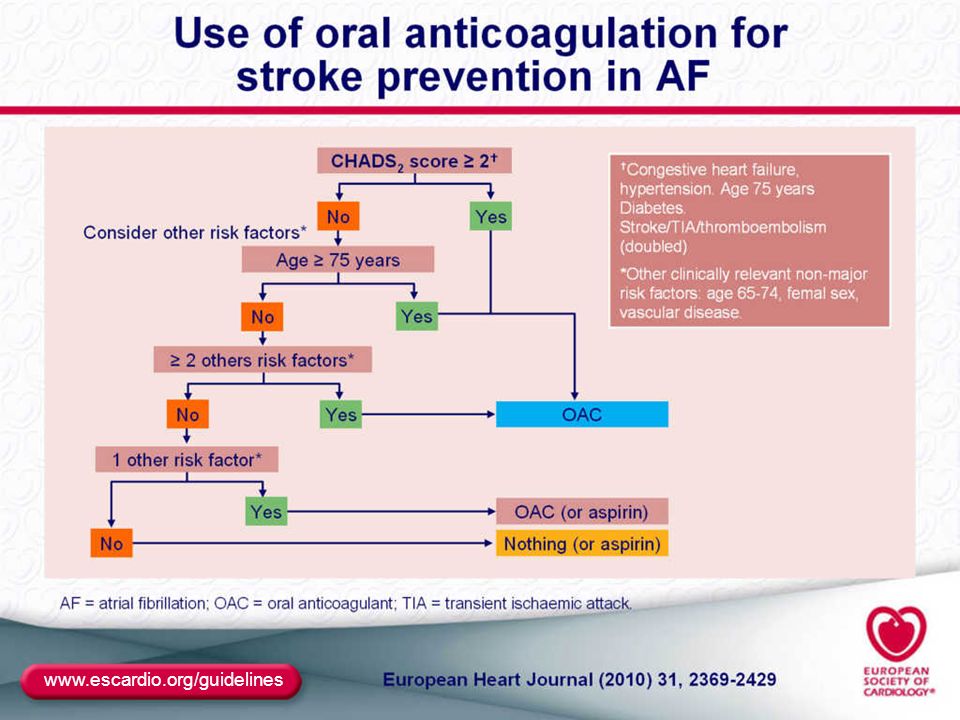
Atrial fibrillation: general principles Record ECG Assess thromboembolic risk (CHADS 2 risk score) Look for precipitating factors (structural heart disease, thyroid disease, pyrexial illness, recent surgery etc) Arrange echocardiogram
 Look for precipitating factors (structural heart disease, thyroid disease, pyrexial illness, recent surgery etc) Arrange echocardiogram")
41
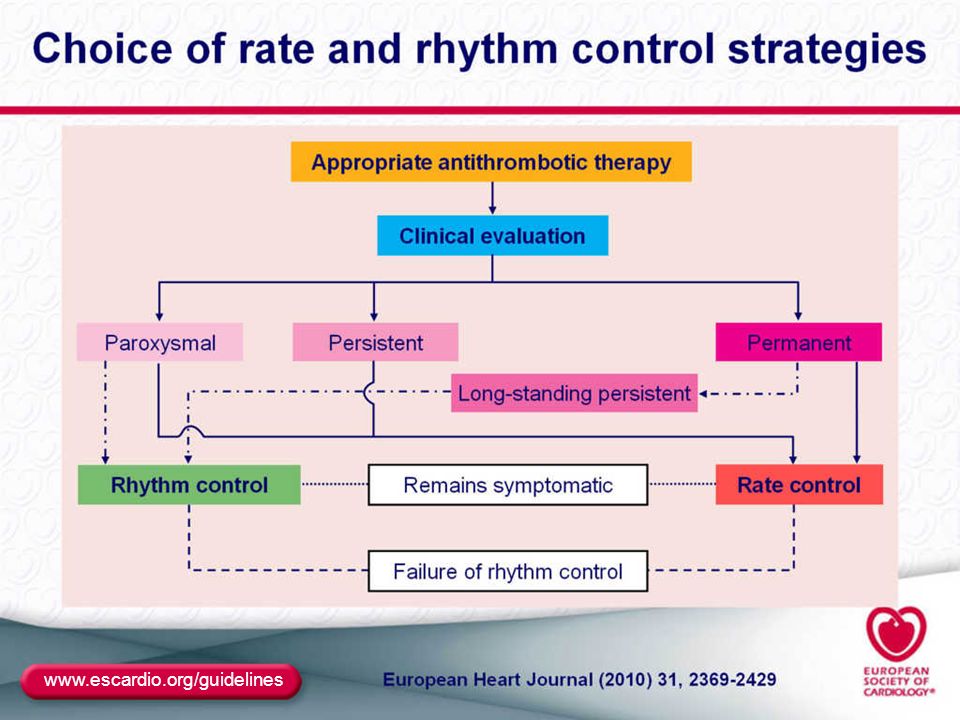
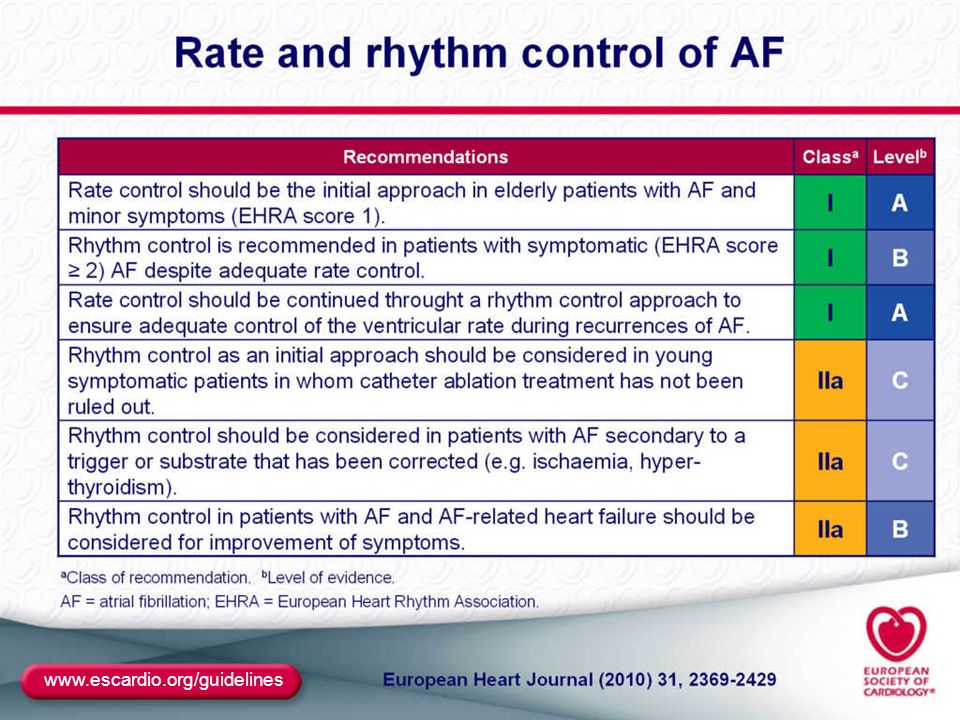
Atrial fibrillation: general principles >12 months duration or detected by chance and subject asymptomatic: rate control and appropriate thromboprophylaxis <12 months duration but minimal or no symptoms and low probability of maintaining SR: rate control and appropriate thromboprophylaxis

42
Atrial fibrillation: general principles <12 months duration and symptomatic: rate control, anticoagulate and consider referral for cardioversion Paroxysmal AF: rhythm control – drugs and/or catheter ablation AF associated with SND: dual chamber PM and antiarrhythmic drug

43
AF: when to refer Problems with rate control For cardioversion of symptomatic persistent AF (most will need long term antiarrhythmic drug therapy as well) Paroxysmal AF Patients with significant LV dysfunction Patients with significant valvular disease
 Paroxysmal AF Patients with significant LV dysfunction Patients with significant valvular disease")
44
Diagnosing heart failure Clinical assessment ECG CXR Echocardiogram BNP

45
Clinical assessment (suspected heart failure) Symptoms Medical history (previous MI, hypertension, diabetes Family history (cardiomyopathies) Physical findings (S3, S4, murmur, raised JVP, lung crackles, oedema.
 Symptoms Medical history (previous MI, hypertension, diabetes Family history (cardiomyopathies) Physical findings (S3, S4, murmur, raised JVP, lung crackles, oedema.")
46
ECG Abnormal in 80-90% of patients with significant heart failure Left atrial hypertension Q waves LVH T wave changes LBBB

47
CXR Can be ‘normal’ even in advanced HF Cardiomegaly PV hypertension Septal lines Pleural effusions Pulmonary oedema

48
Echocardiography Gold standard Systolic and diastolic function Valve disease Pericardial disease Easily repeated

49
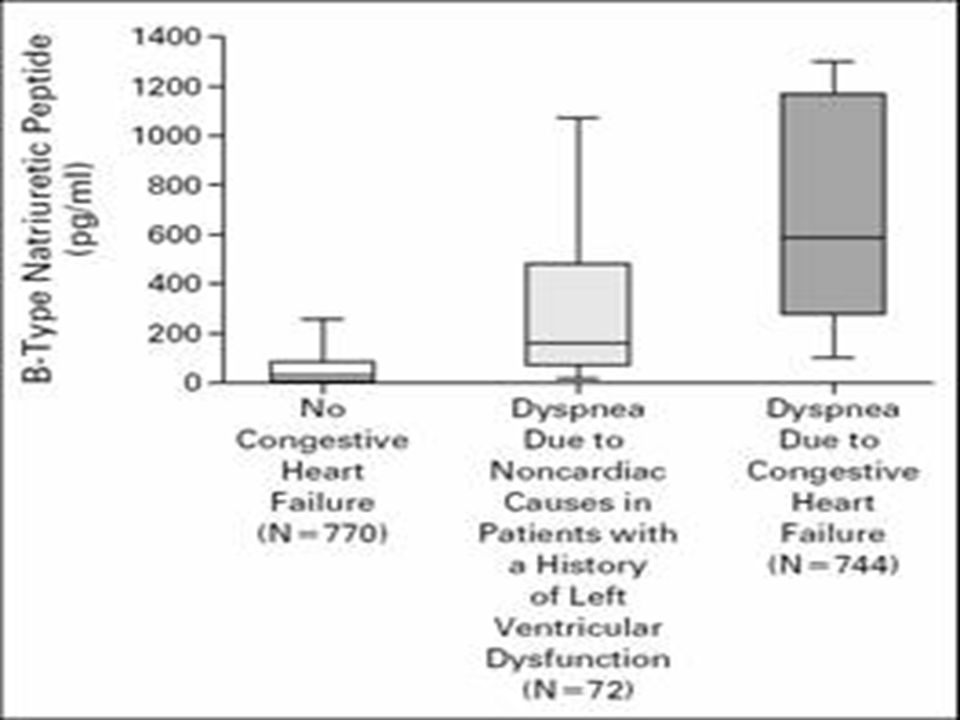
BNP HF most unlikely if normal May help predict severity of HF False positive results

53
Suggested diagnostic pathway Suspected HF BNP and/or ECG Both normal (likelihood of HF <1%) PFT/CXR/ETT One or both abnormal Echocardiogram
 PFT/CXR/ETT One or both abnormal Echocardiogram")
Similar presentations












 -Pt acutely unwell with palpitations -Pt with haemodyanically unstable acute onset AF -2 nd /3 rd heart block -Exercise.>")









 Risk factors (associated diseases) Physical signs Investigations Complications and treatment.>")




