Download presentation
Presentation is loading. Please wait.

1
Puberty Disorders Dr. Sarar Mohamed
MBBS, FRCPCH(UK), MRCP (UK), MRCPCH(UK), DCH(Ire), CCST(Ire), CPT(Ire), MD Consultant Pediatric Endocrinologist & Metabolic Physician Assistant Professor of Pediatrics King Saud University
, MRCP (UK), MRCPCH(UK), DCH(Ire), CCST(Ire), CPT(Ire), MD. Consultant Pediatric Endocrinologist & Metabolic Physician. Assistant Professor of Pediatrics. King Saud University.")
3
Definition of puberty What is puberty?
It is the transitional period of development during which an individual mature from childhood to physical, psychosocial, sexual & reproductive maturity

4
FERTILITY AND FINAL HEIGHT
PUBERTY Gonadal maturation with acquisition of secondary sexual characteristics and associated growth spurt FERTILITY AND FINAL HEIGHT

5
Endocrine Regulation Negative feedback: Insert fig. 20.9 Female: Male:
Inhibits GnRH from hypothalamus. Inhibits anterior pituitary response to GnRH. Inhibin secretion inhibits anterior pituitary release of FSH. Female: Estrogen and progesterone. Male: Testosterone. Insert fig. 20.9

6
Onset of puberty The age of onset of puberty -Females ----8-13
Average age of onset: GIRLS 10 to 11 years (range 8 to 13 years) BOYS 11 to 12 years (range 9 to 14 years) F 2- Pubic hair is the first visible physical sign of puberty T 3- The maximum growth velocity occurs ar 12 years T 4- The age of menarche has decreased over the last 3-4 decades due to improved nutrition, general health & life style F 5-Menarche marks the attainment of reproductive maturity
 BOYS 11 to 12 years (range 9 to 14 years) F 2- Pubic hair is the first visible physical sign of puberty. T 3- The maximum growth velocity occurs ar 12 years. T 4- The age of menarche has decreased over the last 3-4 decades due to improved nutrition, general health & life style. F 5-Menarche marks the attainment of reproductive. maturity.")
7
Duration of puberty The time from onset to completion of puberty
Average Y Range Y

8
Factors That Affect Puberty
Genetics Race/Ethnicity Previous nutrition Subcutaneous fat Birth weight Obesity Increased leptin and estrogen production Insulin stimulation of ovaries & uterus

9
Initial signs of puberty
GIRLS – Breast Development BOYS – Testicular Enlargement Volume > 3.0 cm³ Length > 2.5 cm

10
Growth in puberty Insert fig

11
Evaluation of disorder of puberty
CLINICAL ASSESSMENT History Behavioural changes Pubertal staging Skin examination Height measurement / Growth velocity Bone age assessment Hormone study if needed

12
Assessment of Puberty History Parents
onset of puberty Menarche Male Age of first shaving regularly Parental heights (MPH) prenatal and perinatal (exposure to exogenous sex steroids in intrauterine period; birth weight, perinatal asphyxia) Concomitant illnesses, postnatal exposure to sex steroids time of first sign of puberty Thelarche (galactorrhea) Adrenarche/pubarche (body odor, axillary & pubic hair, acne) Gonadarche
 prenatal and perinatal (exposure to exogenous sex steroids in intrauterine period; birth weight, perinatal asphyxia) Concomitant illnesses, postnatal exposure to sex steroids. time of first sign of puberty. Thelarche (galactorrhea) Adrenarche/pubarche (body odor, axillary & pubic hair, acne) Gonadarche.")
13
History Important to include:
Past medical history (history of brain tumor, radiation, chemotherapy, known genetic disorder, chronic disease affecting growth) Eating habits Any evidence of disordered eating Activity level Is exercise excessive or is this an athlete with a high level of training Growth history Previous growth chart can be extremely helpful
 Eating habits. Any evidence of disordered eating. Activity level. Is exercise excessive or is this an athlete with a high level of training. Growth history. Previous growth chart can be extremely helpful.")
14
History Review of Systems
CNS: visual changes/visual field abnormalities, headaches, anosmia Cardiac: congenital anomaly Respiratory: asthma Renal: GI: diarrhea, blood in stools

15
Physical Examination Examination of Growth
Height Weight Pubertal Assessment (Tanner staging) Axillary hair Pubic hair & staging Breast development & staging Genital development & staging skin, hair, thyroid Neurological assessment
 Axillary hair. Pubic hair & staging. Breast development & staging. Genital development & staging. skin, hair, thyroid. Neurological assessment.")
16
Growth charts

17
Staging of pubertal development in girls
(Tanner) B 1-5, Pu 1-5, A 1-5. (B2 – first sign of female puberty)
 B 1-5, Pu 1-5, A 1-5. (B2 – first sign of female puberty)")
18
Staging of pubertal development in boys
(Tanner) G1-5, Pu 1-5, A 1-5, testicular volum > 4 ml – first sign of male puberty
 G1-5, Pu 1-5, A 1-5, testicular volum > 4 ml – first sign of male puberty.")
20
Diagnostic evaluation
Laboratory gonadotropins (FSH, LH) basal and peak after LHRH stimulation (prepubertal LH/FSH<1) estradiol testosteron (basal value and value after LH stimulation) adrenal androgens (17-OHP, A-dion,...) and ACTH bone age Pelvic US (ovarian and uterine size) CT or MRI of adrenals, Brain Vaginoscopy Genetic – karyotype, DNA analysis
 basal and peak after LHRH stimulation (prepubertal LH/FSH<1) estradiol. testosteron (basal value and value after LH stimulation) adrenal androgens (17-OHP, A-dion,...) and ACTH. bone age. Pelvic US (ovarian and uterine size) CT or MRI of adrenals, Brain. Vaginoscopy. Genetic – karyotype, DNA analysis.")
21
Bone age 2 yrs 6 m. 10 yrs 12 yrs

22
Summary:Variants of puberty
Premature thelarché exclude the start of precocious puberty! Premature adrenarché exclude simple virilising form of CAH! Premature menarché exclude vaginal bleeding due to trauma of vagine or rare ovarian cyst! Bone age is not accelerated! FSH and LH levels after LH-RH are normal Gonadal and adrenal steroid levels are normal Pelvic and adrenal ultrasonography is normal Reassurance & f/u

23
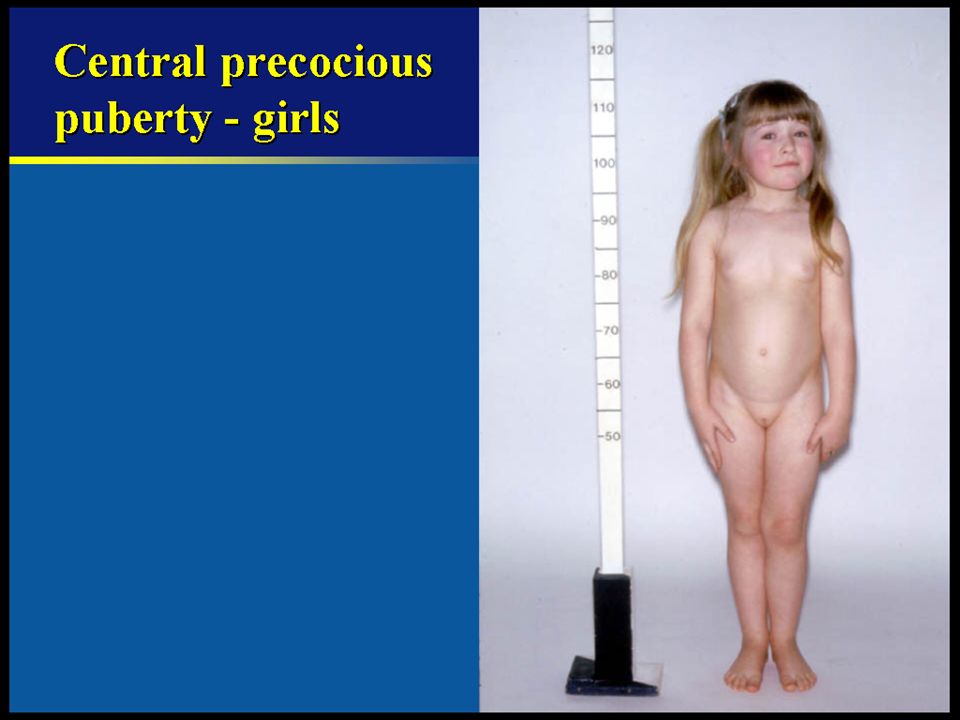
PRECOCIOUS PUBERTY

25
Landmark Case of Precocious Puberty
5 year old Lina Medina of Peru Menses onset age 8 months Breast development age 4 Advanced bone maturation age 5 Was evaluated for abdominal tumor due to increasing abdominal size at age 5 On 5/14/1939 gave birth to a 2.9 kg baby boy

26
Definition of Precocious Puberty
ONSET OF PUBERTY BEFORE -Females years -Males years Lawson Wilkins Pediatric Endocrine Society recommended 7 for white girls/ 6 for back The prevalence is estimated to be between one in 5,000 to 10,000 children annually in the United States.

27
Classification Central (true), gonadotropin-dependent
Early stimulation of hypothalamic-pituitary-gonadal axis. Peripheral, GnRH independent (precocious pseudopuberty) The source of sex steroid may be endogenous or exogenous, gonadal or extragonadal, independent of gonadotropins stimulation.
 The source of sex steroid may be endogenous or exogenous, gonadal or extragonadal, independent of gonadotropins stimulation.")
28
True precocious puberty (central, GnRH dependent)
Idiopatic, constitional sporadic or familial (common) CNS abnormalities Congenital (hydrocephalus, arachnoid cysts, ...) Acquired pathology (posttraumatic, infections, radiation,.. Tumors (LH secreting pituitary microadenoma, glioma – may be associated with neurofibromatosis, hamartoma,.. Reversible forms - space occuping or pressure-associated lesion (abscess, hydrocephalus,...) Adopted children or children emigrating from developping countries - Improved nutrition, environmental stability and psychosocial support
 CNS abnormalities. Congenital (hydrocephalus, arachnoid cysts, ...) Acquired pathology (posttraumatic, infections, radiation,.. Tumors (LH secreting pituitary microadenoma, glioma – may be associated with neurofibromatosis, hamartoma,.. Reversible forms - space occuping or pressure-associated lesion (abscess, hydrocephalus,...) Adopted children or children emigrating from developping. countries. - Improved nutrition, environmental stability and psychosocial support.")
29
True precocious puberty (central, gonadotropin-dependent)
Bone age is accelerated FSH and LH elevation after LH-RH is diagnostic test (LH/FSH > 2) LH LH/FSH ratio < 1 Prepubertal LH LH/FSH ratio > 1 Pubertal MRI of CNS is necessary to exclude the neoplasia
 LH LH/FSH ratio < 1 Prepubertal. LH LH/FSH ratio > 1 Pubertal. MRI of CNS is necessary to exclude the neoplasia.")
32
Treatment of true precocious puberty
Purpose of treatment To prevent psychosocial distress To improve final height outcome Treat the underlying cause GnRH analogue Lupron depot ped, leuprolide acetate Desensitizes the pituitary Blocks LH and FSH secretion Prevents continued sexual development for the duration of the treatment Growth may almost stop while on therapy ± addition of growth hormone remains controversy

33
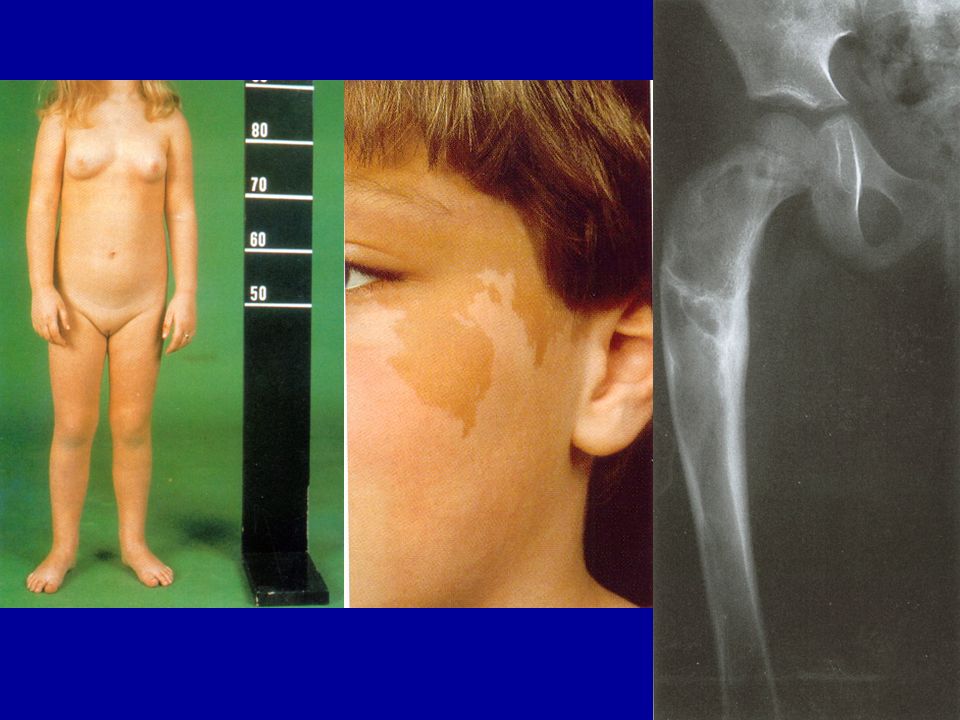
Precocious pseudopuberty in girls (gonadotropin-independent)
McCune - Albright syndrome Ovarian cysts Isolated follicular cysts with E2 production. Self-limiting with spontaneous regression. Ovarian tumors Acceleration of bone age FSH and LH are low after LH-RH stimulation Estrogens are elevated

35
Precocious pseudopuberty in boys (gonadotropin-independent)
Congenital adrenal hyperplasia (CAH) Undiagnosed or inadequately treated simple virilising form of CAH caused by 21-hydoxylase deficiency. Neonatal screening? Testotoxicosis Activating mutation of LH receptor. AD inheredited. Tumors Gonadal (testosterone-secreting Leydig cell tumor) Adrenal (adenoma, carcinoma) Exogenous androgens (anabolic steroids – iatrogene, doping) McCune Albright Syndrome Acceleration of bone age FSH and LH are low after LH-RH stimulation Testicular or adrenal steroids are elevated
 Undiagnosed or inadequately treated simple virilising form of CAH caused by 21-hydoxylase deficiency. Neonatal screening Testotoxicosis. Activating mutation of LH receptor. AD inheredited. Tumors. Gonadal (testosterone-secreting Leydig cell tumor) Adrenal (adenoma, carcinoma) Exogenous androgens (anabolic steroids – iatrogene, doping) McCune Albright Syndrome. Acceleration of bone age. FSH and LH are low after LH-RH stimulation. Testicular or adrenal steroids are elevated.")
36
21-OH CAH: DeHydroEpiAndrosterone Desmolase Cholesterol Desmolase
17 a OH Pregnenlolone 17 OH Pregnenlolone DeHydroEpiAndrosterone 3 B HSD 3 B HSD 3 B HSD Androstendione 17 a OH Progesterone 17 OH Progesterone Testosterone Estradiol 21 OH 21 OH 90 % of CAH 50-70 % salt wasting Female = ambiguous, Hyperpig Male = virlization Desoxycorticosterone 11 Desoxycortisol 11 OH Depend on the degree 11 OH Treatment Hydrocortisone Fludrocortisone Corticosterone Cortisol 18 OH 18 OH Corticosterone Aldosterone

37
Non classic CAH .

38
Precoccious puberty-treatment
Gonadotropin-dependent PP Idiopathic GnRH (LH-RH) analog to block LH-RH receptor of pituitary gland Organic – tumor or cysts Surgery Gonadotropin independent (pseudopuberty) -treat underline cause testicular, ovarian or adrenal tumors –surgery CAH – substitution of corticosteroids
 analog to block LH-RH receptor of pituitary gland. Organic – tumor or cysts. Surgery. Gonadotropin independent (pseudopuberty) -treat underline cause. testicular, ovarian or adrenal tumors –surgery. CAH – substitution of corticosteroids.")
39
Delayed puberty .

40
Delayed puberty - definition
Initial physical changes of puberty are not present by age 13 years in girls (or primary amenorhoe at y) by age 14 years in boys
 by age 14 years in boys.")
41
Types of delayed puberty
Gonadotropin dependent Hypogonadotropic hypogonadism Low LH/FSH Central, chronic disease Gonadotropin independent Hypergonadotropic hypogonadism High LH/FSH Peripheral cause (gonads)
")
42
GnRH or gonadotropin dependent
Idiopathic sporadic or familial (associated with constitutional growth delay) Chronic diseases with bone age delay and growth retardation due to different pathophysical mechanismes (malnutrition, anemia, acidosis, hypoxia,...anorexia nervosa, cystic fibrosis, chronic renal insuficiency,..) Psychosocial deprivation
 Chronic diseases. with bone age delay and growth retardation due to different. pathophysical mechanismes (malnutrition, anemia, acidosis, hypoxia,...anorexia nervosa, cystic fibrosis, chronic renal insuficiency,..) Psychosocial deprivation.")
43
GnRH or gonadotropin dependent
Hypogonadotropic hypogonadism Gonadotropin deficiency LH only (fertile eunuch syndrome) FSH and LH - Congenital (genetic, syndromes) - Kallman syndrome –mutation of KAL gene, mutation of DAX1 gene, Prader-Willi syndrome ,... - Acquired - cranial irradiation, hemosiderosis, granulomtous disease Associated with others pituitary hormones deficiencies - Congenital – empty sella syndrome, genetic-transcription factors, disruption of pituitary stalk (breech delivery),... - Acquired – tumors, inflamation, irradiation, trauma....
 FSH and LH. - Congenital (genetic, syndromes) - Kallman syndrome –mutation of KAL gene, mutation of DAX1 gene, Prader-Willi syndrome ,... - Acquired - cranial irradiation, hemosiderosis, granulomtous disease. Associated with others pituitary hormones deficiencies. - Congenital – empty sella syndrome, genetic-transcription factors, disruption. of pituitary stalk (breech delivery),... - Acquired – tumors, inflamation, irradiation, trauma....")
44
Kallmann Syndrome

45
Kallman Syndrome A syndrome of isolated gonadotropin deficiency
1/10,000 males, 1/50,000 females KAL-1 gene Present with ANOSMIA or HYPOSMIA Can also be associated with harelip, cleft palate, and congenital deafness

46
Syndromes Associated with Pubertal Delay
Prader-Willi syndrome Laurence Moon syndrome Septo-optic dysplasia Bardet-Biedl syndrome

47
Gonadotropin independent (hypergonadotrophic)
Boys Congenital Anorchia Chromosomal abnormalities (Klinefelter syndrome, Noonan syndrome…) Disorders in androgen synthesis or action Acquired Autoimunne inflamation (APS) Radio or chemotherapy Traumatic Surgery
 Disorders in androgen synthesis or action. Acquired. Autoimunne inflamation (APS) Radio or chemotherapy. Traumatic. Surgery.")
48
Klinefelter’s Syndrome
45 XXY most common (2/3), Tall in childhood, with euchanoid body habitus More female type fat distribution puberty is delayed Small testicles & gynecomastia 90-100% are infertile
, Tall in childhood, with euchanoid body habitus. More female type fat distribution. puberty is delayed. Small testicles & gynecomastia % are infertile.")
49
Klinefelter's syndrome
A 19-year-old phenotypic male with chromatin-positive seminiferous tubule dysgenesis (Klinefelter's syndrome). The karyotype was 47,XXY, gonadotropin levels were elevated, and testosterone levels were low normal. Note normal virilization with long legs and gynecomastia (B, C). The testes were small and firm and measured 1.8 × 0.9 cm. Testicular biopsy revealed a severe degree of hyalinization of the seminiferous tubules and clumping of Leydig cells. D, A 48-year-old male with 47,XXY Klinefelter's syndrome with severe leg varicosities. (Williams Textbook of Endocrinology, 10th ed, 2003)
. The karyotype was 47,XXY, gonadotropin levels were elevated, and testosterone levels were low normal. Note normal virilization with long legs and gynecomastia (B, C). The testes were small and firm and measured 1.8 × 0.9 cm. Testicular biopsy revealed a severe degree of hyalinization of the seminiferous tubules and clumping of Leydig cells. D, A 48-year-old male with 47,XXY Klinefelter s syndrome with severe leg varicosities. (Williams Textbook of Endocrinology, 10th ed, 2003)")
50
Gonadotropin independent (hypergonadotrophic hypogonadism)
Girls Congenital Billateral ovarian torsion Chromosomal abnormalities (Turner syndrome, pure gonadal dysgenesis, Noonan syndrome…) Acquired Autoimunne inflamation (APS) Radio or chemotherapy Traumatic Surgery
 Acquired. Autoimunne inflamation (APS) Radio or chemotherapy. Traumatic. Surgery.")
51
Turner syndrome Karyotype 45,X (60%)
(45,X/46,XX, structural abnormalities of X chromosome) Incidence 1/2000 Short stature (final height cm)/ web neck Gonadal dysgenesis - streak gonad Autoimmune : Hashimoto’s thyroditis, Addison’s ds Mild insulin resistance & Essential hypertension hearing loss /No mental defect Impairment of cognitive function : mathematical ability↓ Visual–motor coordination, spatial-temporal processing↓ Y chromosome predisposed to gonadoblastoma H. Turner, 1938
 Incidence 1/2000. Short stature (final height cm)/ web neck. Gonadal dysgenesis - streak gonad. Autoimmune : Hashimoto’s thyroditis, Addison’s ds. Mild insulin resistance & Essential hypertension. hearing loss /No mental defect. Impairment of cognitive function : mathematical ability↓ Visual–motor coordination, spatial-temporal processing↓ Y chromosome predisposed to gonadoblastoma. H. Turner,")
52
Investigation of Delayed Puberty
Investigations depend on clinical presentation, but may include Bone age Hormone levels (IGF-1, FSH, LH, estradiol, testosterone, DHEAS, prolactin, TSH) Karyotype Hormone stimulation tests GnRH stimulation test GH stimulation test Imaging MRI brain if gonadotropins low & no obvious cause of hypogonadotropic hypogonadism US or MRI pelvis
 Karyotype. Hormone stimulation tests. GnRH stimulation test. GH stimulation test. Imaging. MRI brain if gonadotropins low & no obvious cause of hypogonadotropic hypogonadism. US or MRI pelvis.")
53
Treatment of delayed Puberty
Treat underline cause Time of therapy initiation may vary and individualized Testosterone supplementation Estrogen for girls

Similar presentations










 By: Anna Heideman & Angela Mullins.>")






>")





