Download presentation
Presentation is loading. Please wait.

1
Urinary Tract Infections

2
The frequent flushing action of urine.
Urinary tract infections (UTI) are the most common bacterial infection Over 50% of all women experience at least one lifetime UTI. One in ten women experience frequent recurrent infections for at least some period. Nosocomial UTI accounts for about 40% of all infections acquired in acute care facilities. Physical and chemical barriers that protect the urinary tract from infection: The frequent flushing action of urine. Urine acidity ( pH 4.5-8*). The prostatic secretions (lysozyme and IgA). N * Acid base balance.
 are the most common bacterial infection. Over 50% of all women experience at least one lifetime UTI. One in ten women experience frequent recurrent infections for at least some period. Nosocomial UTI accounts for about 40% of all infections acquired in acute care facilities. Physical and chemical barriers that protect the urinary tract from infection: The frequent flushing action of urine. Urine acidity ( pH 4.5-8*). The prostatic secretions (lysozyme and IgA). N. * Acid base balance.")
3
Risk factors of urinary tract infection in both sexes:
Diabetes mellitus. Indwelling urinary catheter or nephrostomy. Urinary tract obstruction: tumor, calculi or congenital structural abnormalities. Poor hygiene. UTI is more common in women due to: Anatomy: short female urethra, and proximity of the urethra to the anus. Lack of antibacterial prostatic secretions. Bacterial invasion by sexual intercourse. Pregnancy. N * Acid base balance.

4
Urinary catheter and nephrostomy tube

5
Classification of UTI:
Upper UTI: Kidney infection (pyelonephritis, tubulointerstitial nephritis, glomerulonephritis, renal abscess). Lower UTI: Urinary bladder infection (cystitis). Prostatic infection in men. Urethral infections (urethritis) classified as sexually transmitted diseases.
. Lower UTI: Urinary bladder infection (cystitis). Prostatic infection in men. Urethral infections (urethritis) classified as sexually transmitted diseases.")
6
Types of Pyelonephritis:
Pyelonephritis: Pyelum: Renal pelvis. Nephro: kidney Acute inflammation of renal pelvis and medullary tissue due to bacterial invasion. Types of Pyelonephritis: Acute non complicated (non-obstructive) pyelonephritis. Complicated (chronic) pyelonephritis: Underlying structural or functional abnormalities of the kidney. Could be associated with obstruction of renal pelvis or tissue dysfunction or renal abscess. N
 pyelonephritis. Complicated (chronic) pyelonephritis: Underlying structural or functional abnormalities of the kidney. Could be associated with obstruction of renal pelvis or tissue dysfunction or renal abscess. N.")
7
n Biofilm: A layer of bacteria with their extracellular substances, and urine components (protein, calcium, Mg+2). It contaminate the draining bags and grow along the exterior and internal catheter surface. Biofilm is strongly associated with establishment of complicated pyelonephritis.

8
Recurrent infection: either reinfection or relapse
When a new organism is isolated or a previously isolated organism is reintroduced into the urinary tract from the colonizing gut or genital flora. Relapse: The bacteria persist within the urinary tract due to presence of a stone or an indwelling urologic devices (biofilm). N
. N.")
9
Etiology of Pyelonephritis and TIN:
Escherichia coli. The most common cause of UTI (85-90%). Staphylococcus saprophyticus. The second causative agent of UTI (5-20%). Other genera of Enterobacteriaceae : Klebsiella, Enterobacter, Proteus, and Serratia. Pseudomonas aeruginosa and Enterococcus faecalis. Hospital-acquired infection.
. Staphylococcus saprophyticus. The second causative agent of UTI (5-20%). Other genera of Enterobacteriaceae : Klebsiella, Enterobacter, Proteus, and Serratia. Pseudomonas aeruginosa and Enterococcus faecalis. Hospital-acquired infection.")
10
Source of infecting organisms: Ascending rout (the most common):
Pathogenesis: Source of infecting organisms: Ascending rout (the most common): The colonizing flora from the periurethral area, gut flora or in woman vaginal flora. Contaminated urologic devices. Descending rout (not common): Hematogenous spread.
: The colonizing flora from the periurethral area, gut flora or in woman vaginal flora. Contaminated urologic devices. Descending rout (not common): Hematogenous spread.")
11
The infection usually starts as lower UTI.
The most common bacteria is uropathogenic Escherichia coli. E. coli adhere to mannosylated glycoproteins that line the bladder mucosa by the mannose sensitive fimbria FimH. It then ascend to the kidney by one of these routs: Reflux of infected urine up the ureter. Short intravesical ureter. Incompetent ureteral sphincters. Polymorph nuclear (PMN) cells influx up the ureter.
 cells influx up the ureter.")
12
Damage of interstitial tissue due to:
The bacteria then enter through the papillae into the renal parenchyma. P fimbria and K polysaccharide of the bacteria adhere to the glycosphingolipid disaccharide receptor on the interstitial tissue surrounding the tubules and renal cells in the medulla. Damage of interstitial tissue due to: Microbial virulence: Hemolysin, and urease activity. Cellular infiltration & cytokines production; inflammation (toxic O2 radicals, and lysozymes). Activation of clotting factors; ischemia. Tubulointerstitial nephritis (TIN). N
. Activation of clotting factors; ischemia. Tubulointerstitial nephritis (TIN). N.")
13
N

14
Pathogenesis: N

15
Types of Tubulointerstitial Nephritis:
Acute TIN: Inflammatory infiltrate and edema affecting the renal interstitial tissue. Often develops over days to months. Over 95% of cases result from an allergic drug reaction or infection. Renal abscess (uncommon complication) mainly caused by bacteremic spread of infection from other body site, and could be illustrated microscopically in some cases.
 mainly caused by bacteremic spread of infection from other body site, and could be illustrated microscopically in some cases.")
16
Interstitial Renal Abscesses :
- Necrosis contains neutrophils, and germ (bacteria) colonies, hematoxylinophils*. - Tubules are damaged and may contain neutrophil casts. - In early stages, the glomeruli and vessels are normal. Hematoxylin→ purple
 colonies, hematoxylinophils*. - Tubules are damaged and may contain neutrophil casts. - In early stages, the glomeruli and vessels are normal. Hematoxylin→ purple.")
17
n Chronic TIN: Gradual interstitial infiltration and fibrosis, tubular atrophy and dysfunction, and a gradual deterioration of renal tissue, usually over years. Glomerular involvement is much more common in chronic nephritis than acute type. Causes: immunologically mediated disorders, infections, and drug interaction.

18
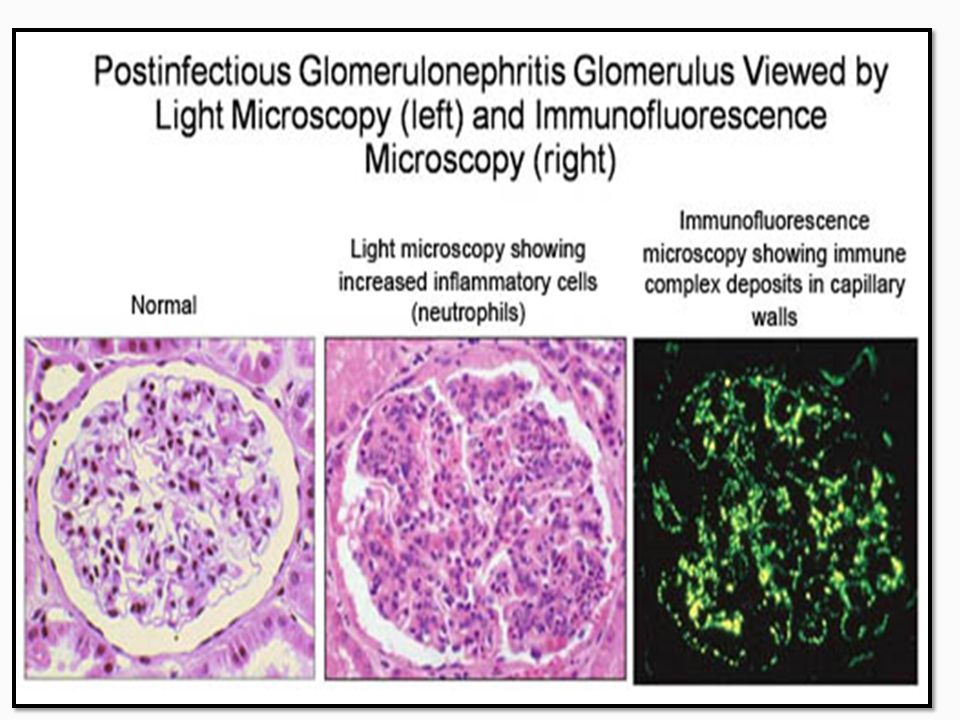
Glomerulonephritis : GN:
-Inflammation of the glomeruli of the nephron. -Types: Infective and non infective. Infective: Source of infection: Hematogenous dissemination (antigen). Pathologic feature: One or more renal cortical abscesses. Pathogenesis: Insoluble antigens trapped in the glomerulus. Antibodies and complement attack the antigen and the structural components of the kidney. Inflammatory destruction of the glomeruli.
. Pathologic feature: One or more renal cortical abscesses. Pathogenesis: Insoluble antigens trapped in the glomerulus. Antibodies and complement attack the antigen and the structural components of the kidney. Inflammatory destruction of the glomeruli.")
19
Types of soluble antigen: Endogenous: Self antigen (SLE). Exogenous:
Non-Infective GN: Soluble antigen in blood stream; reacts with the antibodies (immuncomplex). Serum sickness disease: Precipitation of complexes in the glomeruli; inflammatory destruction. Types of soluble antigen: Endogenous: Self antigen (SLE). Exogenous:
. Serum sickness disease: Precipitation of complexes in the glomeruli; inflammatory destruction. Types of soluble antigen: Endogenous: Self antigen (SLE). Exogenous:")
20
Exogenous: Drugs, toxoid, or serum. Infectious agent antigen: post-streptococcal glomerulonephritis: Anti-Streptolysin-O complexes. Other infections: Bacterial: Staphylococci, Streptococcus pneumoniae, Klebsiella, Yersinia enterocolitica, Treponema, Salmonella Parasites: Malaria, schistosoma, and toxoplasma Viral: Hepatitis, and EBV Fungal: Candida. n

22
Upper urinary tract infection:
Pyelonephritis, TIN, renal abscess & glomerulonephritis. Symptoms & Sings of Upper UTI: Costovertebral angle pain (loin pain, flank pain) and tenderness, usually unilateral but can be bilateral. Fever, nausea, vomiting hematuria. Symptoms of lower tract infection may or may not be present.
 and tenderness, usually unilateral but can be bilateral. Fever, nausea, vomiting. hematuria. Symptoms of lower tract infection may or may not be present.")
23
Laboratory Diagnosis: Urine analysis:
Physical (macroscopic; color), Chemical (glucose, nitrite and proteins) Microscopic proprieties (WBCs, RBCs and casts). Urine culture.
, Chemical (glucose, nitrite and proteins) Microscopic proprieties (WBCs, RBCs and casts). Urine culture.")
24
Physical properties (macroscopic appearance & color):
Urine analysis: Physical properties (macroscopic appearance & color): Turbidity or white or milky* color: pus in urine (pyuria) infection. Red color: RBCs in urine: (Hematuria): kidney stones, infections or tumors. Chyluria
: Turbidity or white or milky* color: pus in urine (pyuria) infection. Red color: RBCs in urine: (Hematuria): kidney stones, infections or tumors. Chyluria.")
26
Chemical properties: Glucose in urine (glycosuria):
considered as a risk factor for bacterial infection; bacteria utilize glucose during binary fission. Nitrite in urine (nitrituria): Enterobacteriaceae species reduce nitrate to nitrite nitritiuria indicates the presence of coliform bacteria (Enterobacteriaceae) in urine. Proteins: N
: Enterobacteriaceae species reduce nitrate to nitrite. nitritiuria indicates the presence of coliform bacteria (Enterobacteriaceae) in urine. Proteins: N.")
27
Protein in urine (Proteinuria):
Traces of protein are found in pyelonephritis, and lower UTI: pus cells or bacterial origin and is accompanied by pyuria. Large amounts of protein is found in interstitial nephritis and glomerulonephritis accompanied by hematuria, lower number of pus in urine.

29
Microscopic properties: WBCs: Normal: 2-3 /HPF RBCs: Normal: 3-4 /HPF.
Casts*: Granular, fatty, hemoglobin, and RBCs cast: Acute glomerulonephritis due to immune system response. WBCs cast: acute pyelonephritis, acute tubulointerstitial nephritis due to infection. Urinary casts: cylindrical structures formed in the distal tubules and collecting ducts, then dislodge and pass into the urine. They are formed via precipitation of mucoprotein which is secreted by renal tubule cells, and sometimes also by albumin in conditions of proteinuria.

30
RBCs cast Hemoglobin cast Fatty cast

31
Infective TIN and Infective or Non-infective GN:
Immune-GN Infective -GN Pyuria +++++ + Low number Urine Culture Positive or negative negative Nitrite in urine & Hematuria Hemoglobinuria Usually negative ++++ Proteinuria Trace from pus and bacteria or tubular origin. +++++ (kidney origin) Casts WBCs Cast ((Neutrophil cast Hemoglobin or RBCs Casts.
 Casts. WBCs Cast. ((Neutrophil cast. Hemoglobin or RBCs. Casts.")
Similar presentations













>")



 by the age of 30 years, and over 50% have.>")



