Download presentation
Presentation is loading. Please wait.

1
By: Brittney Mathis RN, BSN

2
Transient concussion=full recovery Contusion Laceration Compression Complete transection (SEVERING)-patient paralyzed below level of injury Primary injury-from initial insult and permanent Secondary-ischemia, hypoxia, edema, and hemorrhagic lesions=destruction of myelin and axons
-patient paralyzed below level of injury Primary injury-from initial insult and permanent Secondary-ischemia, hypoxia, edema, and hemorrhagic lesions=destruction of myelin and axons")
3
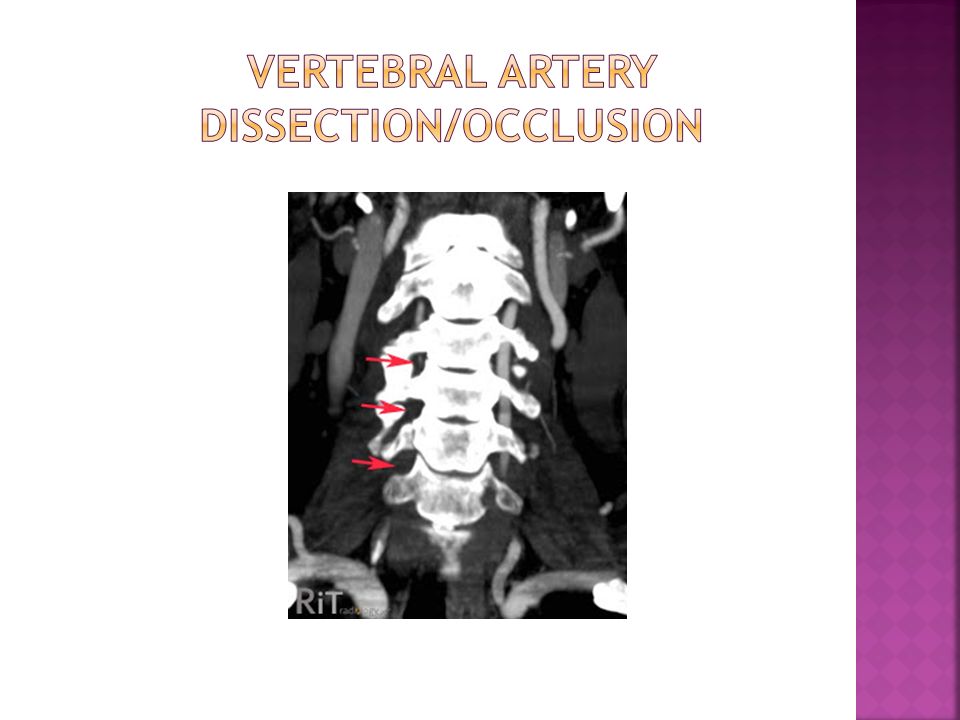
Unstable burst fracture of the atlas caused by severe axial compression (C1) Cause-diving injury Associated injuries may include damage to the vertebral artery traversing the foramen transversarium
 Cause-diving injury Associated injuries may include damage to the vertebral artery traversing the foramen transversarium")
4
Causes-motor vehicle crashes and diving Disrupt ligaments of posterior column, displacing vertebral body posteriorly into spinal canal Neurologic injury common Quadriplegia, loss of pain, and temperature sensation Most common at C5

7
A Complete: No motor or sensory function is preserved in the sacral segments S4 to S5 B Incomplete: Sensory but not motor function is preserved below the neurologic level, and includes the sacral segments S4 to S5 C Incomplete: Motor function is preserved below the neurologic level, and more than half of key muscles below the neurologic level have a muscle grade of less than 3 D Incomplete: Motor function is preserved below the neurologic level, and at least half of key muscles below the neurologic level have a muscle grade of 3 or greater E Normal: Motor and sensory function are normal

8
Frequent Neurological Exams q1-2 hours or as ordered Continuous Cardiac Monitor-bradycardia and asystole common IV steroids Pepcid/Prevacid/Protonix Blood sugar monitoring <140 Increased blood pressure MAP >85 Dopamine Phenylephrine NEVER Norepinephrine (Levophed)! (Department of Orthopaedic Surgery, 2011)
.")
9
Respiratory Management Continuous oxygen saturation monitoring I.S. use and education Aggressive coughing and deep breathing DVT prophylaxis Foley with strict I&O Bowel Regimen

10
From loss of autonomic nervous system Hypotension-decreased cardiac output, venous pooling in extremities, peripheral vasodilation Bradycardia Thermodysregulation (Krassioukov et al., 2007)
")
11
Spinal back board Head in neutral position Cervical collar Log rolling

12
While awaiting long term cervical spinal stabilization, such as Aspen Collar, Philadelphia Collar, or halo, patient should remain on flat surface in neutral position. If patient’s head of bed needs to be elevated, place patient in reverse Trendelenburg.

13
1. This is a 4 (minimum) or 5 person technique depending on the needs of the patient 1 to hold to the patient’s head (in charge of the log roll) 2 (or 3) to support the chest, abdomen and lower limbs 1 to carry out the planned activity (pressure care) 2. Prepare the patient Explain the procedure to the patient regardless of conscious state Request that they lay still and resist assisting Secure all lines, drains and tubes Ensure that the patient is in neutral alignment (straight) 3. Prepare your environment Ensure that the current collar is well fitting prior to the log roll Assemble all necessary equipment i.e. hygiene equipment, wedge for side lying etc Ensure that the log rolling team is correctly positioned 1. Person 1 supports upper body hands on shoulder and hip 2. Person 2 supporting abdomen and lower legs hands on hip and lower legs 3. If 3rd person required more support can be given to lower body (The Royal Melbourne Hospital, 2013)
 or 5 person technique depending on the needs of the patient 1 to hold to the patient’s head (in charge of the log roll) 2 (or 3) to support the chest, abdomen and lower limbs 1 to carry out the planned activity (pressure care) 2. Prepare the patient Explain the procedure to the patient regardless of conscious state Request that they lay still and resist assisting Secure all lines, drains and tubes Ensure that the patient is in neutral alignment (straight) 3. Prepare your environment Ensure that the current collar is well fitting prior to the log roll Assemble all necessary equipment i.e. hygiene equipment, wedge for side lying etc Ensure that the log rolling team is correctly positioned 1. Person 1 supports upper body hands on shoulder and hip 2. Person 2 supporting abdomen and lower legs hands on hip and lower legs 3. If 3rd person required more support can be given to lower body (The Royal Melbourne Hospital, 2013).")
14
Should be preformed every four hours Assess for skin breakdown and pressure points Wash and completely dry skin under collar with each assessment Male patients need to be regularly shaved to prevent skin irrigation (The Royal Melbourne Hospital, 2013)
")
16
(Aspen Medical Products, 2004)
")
17
Maintain head in desired position. Place the sizing guide against head at the highest point of the shoulder muscle. Draw an imaginary line from chin bottom to sizing guide then select collar size. (Aspen Medical Products, 2004)
.")
18
Roll up the back panel Roll the front panel sides inward (Aspen Medical Products, 2004)
")
19
Flare sides of the front panel outward. Place chin piece directly under the chin. Generally, the chin should not extend beyond the edge of the plastic. Push the sides of the front panel up over shoulder muscles around the neck (Aspen Medical Products, 2004)
.")
20
While holding the front panel with one hand, center the back panel and attach both sides to the front. While holding the front panel in place with one hand, pull outward then secure the back panel Velcro straps to the front of the collar. (Aspen Medical Products, 2004)
.")
21
The patient’s chin should be flush with the end of the collar chin piece. The inner trach bar should not be touching the airway. If it does, refit with the next taller size. All slack should be removed from the collar back. The back panel should be centered. From the front the back Velcro straps should be symmetrical. (Aspen Medical Products, 2004)
.")
22
Which of the following should be the nurse’s primary concern when caring for a client who had a recent C4 injury? A. Spinal shock B. Paralytic ileus C. Stress ulcer D. Respiratory compromise

23
D. Using the airway, breathing, and circulation (ABC) priority setting framework, the greatest risk to the client with an SCI at the level of C4 is respiratory compromise secondary to involvement of the phrenic nerve. Maintenance of an airway and provision of ventilator support, as needed, is the priority intervention. Spinal shock, paralytic ileus, and stress ulcers are also of concern, but are not the highest priority.
 priority setting framework, the greatest risk to the client with an SCI at the level of C4 is respiratory compromise secondary to involvement of the phrenic nerve. Maintenance of an airway and provision of ventilator support, as needed, is the priority intervention. Spinal shock, paralytic ileus, and stress ulcers are also of concern, but are not the highest priority..")
24
A nurse is caring for a college student who experienced a T12 fracture while playing football resulting paraplegia. The client has no muscle control of his lower limbs, bowel, bladder, or genital area. The client is 1 week postoperative following spinal stabilization surgery. During the acute phase following SCI prevention of which of the following should be the nurse’s highest priority when planning care for the client? A. Further damage to the spinal cord B. Contractures of the hands and extremities C. Skin breakdown of areas that lack sensation D. Postural hypotension when placing the client in a wheelchair

25
A. The greatest risk to the client during the acute phase of a SCI is further damage to the spinal cord. Therefore, when planning care the priority should be the prevention of further damage to the spinal cord. This should be done through the use of corticosteroids, minimal movement of the client until spinal stabilization is accomplished through either traction or surgery, and adequate oxygenation of the client to decrease ischemia of the spinal cord. Preventing contractures, skin breakdown, and postural hypotension are important, but they are not the highest priority.

26
A patient with a C7 spinal cord injury undergoing rehabilitation tells you he must have the flu because he has a bad headache and nausea. What is your initial action? A. Call the physician. B. Check the patient's temperature. C. Take the patient's blood pressure. D. Elevate the head of the bed to 90 degrees

27
C. Take the patient's blood pressure. Autonomic dysreflexia is a massive, uncompensated cardiovascular reaction mediated by the sympathetic nervous system. Manifestations include hypertension (up to 300 mm Hg systolic), throbbing headache, marked diaphoresis above the level of the lesion, bradycardia (30 to 40 beats/minute), piloerection, flushing of the skin above the level of the lesion, blurred vision or spots in the visual fields, nasal congestion, anxiety, and nausea. It is important to measure blood pressure when a patient with a spinal cord injury complains of a headache.
, throbbing headache, marked diaphoresis above the level of the lesion, bradycardia (30 to 40 beats/minute), piloerection, flushing of the skin above the level of the lesion, blurred vision or spots in the visual fields, nasal congestion, anxiety, and nausea. It is important to measure blood pressure when a patient with a spinal cord injury complains of a headache..")
28
A nurse is caring for client who experienced a cervical spine injury 24 hr ago. Which of the following types of medications prescribed for the client by the provider should the nurse question? A. Glucocorticoids B. Plasma expanders C. H2 antagonists D. Muscle relaxants

29
D. The client will still be in spinal shock 24 hr following the injury. The client will not experience muscle spasms until after the spinal shock has resolved, making muscle relaxants unnecessary at this time. The other medications are appropriate to provide at this time.

31
Aspen Medical Products. (2004, October). Aspen collar sizing guide. Retrieved from http://www.aspenmp.com/images/product-downloads/aspen-collar/aspen-collar- sizing-guide.pdf Department of Orthopaedic Surgery. (2011). Cervical spine injury management guidelines. Retrieved from http://orthosurg.ucsf.edu/oti/patient- care/divisions/spine/resources/cervical-spine-injury-management-guidelines/http://orthosurg.ucsf.edu/oti/patient- care/divisions/spine/resources/cervical-spine-injury-management-guidelines/ Krassioukov, A. V., Karlsson, A., Wecht, J. M., Wuermser, L., Mathias, C. J., & Marino, R. J. (2007). Assessment of autonomic dysfunction following spinal cord injury: Rationale for additions to international standards for neurological assessment. Journal of Rehabilitation Research & Development, 44(1), 103-112. Retrieved from http://www.rehab.research.va.gov/jour/07/44/1/pdf/Krassioukov.pdf http://www.rehab.research.va.gov/jour/07/44/1/pdf/Krassioukov.pdf Pellico, L. H. (2013). Nursing management: Patients with chest and lower respiratory tract disorders. In Focus on adult health medical-surgical nursing3 (pp. 312-322). China: Wolters Kluwer: Lippincott Williams & Wilkins. Pimentel, L., & Diegelmann, L. (2010). Evaluation and management of acute cervical spine trauma. Emergency medicine clinics of north america, 28(4), 719- 738. doi:10.1016/j.emc.2010.07.003 The Royal Melbourne Hospital. (2013). cervical spine guideline. Retrieved from http://clinicalguidelines.mh.org.au/brochures/TRM03.01.pdf
. Cervical spine injury management guidelines. Retrieved from care/divisions/spine/resources/cervical-spine-injury-management-guidelines/ care/divisions/spine/resources/cervical-spine-injury-management-guidelines/ Krassioukov, A. V., Karlsson, A., Wecht, J. M., Wuermser, L., Mathias, C. J., & Marino, R. J. (2007). Assessment of autonomic dysfunction following spinal cord injury: Rationale for additions to international standards for neurological assessment. Journal of Rehabilitation Research & Development, 44(1), Retrieved from Pellico, L. H. (2013). Nursing management: Patients with chest and lower respiratory tract disorders. In Focus on adult health medical-surgical nursing3 (pp ). China: Wolters Kluwer: Lippincott Williams & Wilkins. Pimentel, L., & Diegelmann, L. (2010). Evaluation and management of acute cervical spine trauma. Emergency medicine clinics of north america, 28(4), doi: /j.emc The Royal Melbourne Hospital. (2013). cervical spine guideline. Retrieved from")
Similar presentations







 Service Delivery 2.>")














