Download presentation
Presentation is loading. Please wait.

1
DEVELOPMENTAL DISTURBANCES OF ORAL TISSUES Prf. Dr. Gamal Fatah-ALLAH

2
Titles I- Developmental Disturbances of The tongue. II- Developmental Disturbances of The Oral mucosa IV- Developmental Disturbances of The lip. V- Developmental Disturbances of The Jaws. VI- Developmental Disturbances of The Salivary glands. VII- Developmental Disturbances of The face. VIII- Syndromes associated with abnormalities of oral tissues: http://www.kck.usm.my/ppsg/histology/DF_28.htm

3
Development of tongue First pharyngeal arch – A pair of lateral swellings from mandibular arch and meet in the middle line (median sulcus). – Tuberculum impar: central swelling in-front of foramen cecum in midline (atrophied) Second pharyngeal arch: – Copula (hypobranchial eminence) form the posterior part of tongue.
 Second pharyngeal arch: – Copula (hypobranchial eminence) form the posterior part of tongue..")
4
Normal Structure of the Tongue http://www.kck.usm.my/ppsg/histology/DF_28.htm

6
1- Aglossia An extremely rare Failed embryogenesis of the lateral lingual swellings and tuberculum impar from the fourth to eighth gestational weeks. May occur as – An isolated disorder – Association with other congenital deformities like microstomia, micrognathia.

7
2- Microglossia A condition where the size of the tongue is abnormally small. Difficulties related to speech and swallowing are common.

8
3- Macroglossia Congenital Muscular hypertrophy. Vascular malformations (lymphangioma & hemangioma). Facial hemihypertrophy (Half of the tongue is enlarged). Cretinism. Down syndrome. Acquired Acromegaly. Myxedema. Diabetes. Tumor; Carcinoma. Amyloidosis. Chronic steroid therapy.
. Facial hemihypertrophy (Half of the tongue is enlarged). Cretinism. Down syndrome. Acquired Acromegaly. Myxedema. Diabetes. Tumor; Carcinoma. Amyloidosis. Chronic steroid therapy..")
9
Congenital Macroglossia muscular hypertrophy The strong muscles of the tongue press on the teeth leading to spacing of teeth & malocclusion.

10
Congenital Macroglossia Lymphangioma the tongue is pebbly multiple superficial dilated lymphatic channels.

11
Acquired Macroglossia Pressure on teeth, giving it a scalloped appearance. The scallops reflect the shape of the interdental spaces.

13
4- Benign Migratory Glossitis (Geographic Tongue) Atrophic patches on the dorsal surface of the tongue. Other names: wandering rash, erythema migrans or glossitis areata exfoliativa & benign migratory glossitis.

14
Geographic Tongue Etiology &pathogenesis The exact cause for the condition remains unknown It tends to occur with more intensity in cases of emotional stress. Pathogenesis: Changes in the papillary covering of the tongue. In the center of the patch the filiform papillae are atrophied or desquamated; The fungiform papillae persist (appear as red dots).
..")
15
Clinical Features of Geographic Tongue Females are twice as affected as males. It apears as: rounded, oval or irregular red patches with whitish or yellowish margins. Red dots may be seen (persistence of fungiform papillae). Number: One or several patches may be seen. Coalescence of patches may occur. May be associated with fissured tongue. Fate: They persist for a short time, regress spontaneously But reappear over time (migration).
. Number: One or several patches may be seen. Coalescence of patches may occur. May be associated with fissured tongue. Fate: They persist for a short time, regress spontaneously But reappear over time (migration)..")
16
Typical geographic tongue The patch is red & the center of the patch shows red dots (persistence of fungiform papillae). The periphery of the patch are raised

17
Microscopic examination of geographic tongue Atrophy of filiform papillae The margins show hyperkeratosis and acanthosis. Acute inflammatory cells within epithelium.

18
5- Fissured Tongue Also known as plicated or scrotal tongue. Characterized by folds and fissures in the dorsal surface of the tongue. The fissures are of variable depth and usually extend laterally from a median groove.

19
Causes of fissured tongue Age: – It increases with age – very rarely to be seen in young children. Chronic trauma. Vitamin deficiencies. Associates geographic tongue. Associated syndromes: – Melkerson-Rosenthal syndrome – Down syndrome

20
Clinical Features of Fissured Tongue Patterns: 1- 4 patterns of fissures: Irregular Transverse Cerebriform Foliaceous. It may be – with ulceration at the base (true fissure) with necrotic debris. – No ulceration at the base, it is a furrow (Groove) but the bacteria can accumulate (malodor).
 with necrotic debris. – No ulceration at the base, it is a furrow (Groove) but the bacteria can accumulate (malodor)..")
22
Melkerson-Rosenthal Syndrome Characterized by fissured tongue, facial Swelling & facial paralysis.

23
6- Median Rhomboid Glossitis The presence of red patch (rounded or oval in shape) on the dorsal surface of the tongue just anterior to circumvallate papillae in the midline.
 on the dorsal surface of the tongue just anterior to circumvallate papillae in the midline.")
24
Etiology Two proposed theories either – Acquired (nowadays more accepted): Fungal infection caused by Candida albicans – Developmental: Persistence of tuberculum impar during embryogenesis.
: Fungal infection caused by Candida albicans – Developmental: Persistence of tuberculum impar during embryogenesis.")
25
Clinical Features of Median Rhomboid Glossitis Mainly in adults and rarely in children. May be – Flat, slightly raised or lobulated. It is usually asymptomatic or may cause a slight burning sensation associated with spicy foods.

26
Appear as ovoid or rhomboid-shaped reddish patch on the dorsal surface of the tongue anterior to circumvallate papillae (V-shaped sulcus terminalis).
.")
27
Microscopic features of Median Rhomboid Glossitis Absence of filiform papillae (depapillated area). Hyperplasia of surface epithelium with acanthosis called (pseudoepitheliomatous hyperplasia) of the covering epithelium.
 of the covering epithelium..")
28
7- Hairy Tongue Filiform papillae of the tongue: – Actual hypertrophy – Failure of desquamation of the. Etiology: – Smoking. – Anemia and gastric troubles. – Broad spectrum antibiotics. – Head and neck irradiation after cancer.

29
Hairy tongue The dorsal surface of the tongue appears yellowish-white or brown or even black (depending on diet, oral hygiene and types of bacteria inhabiting these papillae). Some patients may complain from gagging sensation, when the papillae touch the soft palate.

31
8-Tongue-Tie (Ankyloglossia) The lingual frenulum is attached close to the tongue tip, resulting in reduced tongue movement.
 The lingual frenulum is attached close to the tongue tip, resulting in reduced tongue movement.")
32
Ankyloglossia caused by short lingual frenulum that prevents the tongue from protruding.

33
9-Tongue Hypermobility Caused by abnormal long frenulum which may allow the tongue to slip back and obstruct the airway causing suffocation.

34
10- Bifid (Cleft) Tongue The tongue is divided longitudinally for a certain distance with a groove or split (running lengthwise along the tip of the tongue). Also called cleft tongue, diglossia. Types: complete & partial clefts.

35
Complete Cleft Tongue Extremely rare, presents as a cleft starting from the tip of tongue and proceeding to some distance in the direction of the median sulcus.

36
Partial Cleft Tongue More common than complete cleft and is manifested as a deep groove in the midline of the dorsal surface of the tongue.

38
11- Lingual Thyroid Nodule Ectopic thyroid tissue located at the base of the tongue in the area of foramen cecum. Due to failure of the thyroid anlage to migrate to its position in the neck during the early stages of development (4 th week of intrauterine life).
..")
39
Development of Thyroid Gland The thyroid gland develops at 4 th week of IUL, just behind the tuberculum impar (foramen cecum). Then grows downward to the neck.

40
Clinical Features of Lingual Thyroid Nodule Discovered in adults or early adults or at any age. Appears clinically as asymptomatic midline, purplish swelling in or near the base of the tongue in the area of the foramen cecum. It may cause dysphagia. The proper diagnosis can be made by using scintigraphy (scintiscan) for radioactive iodine.
 for radioactive iodine..")
41
Clinical Features of Lingual Thyroid Nodule Appears clinically as asymptomatic midline, purplish swelling in or near the base of the tongue in the area of the foramen cecum.

42
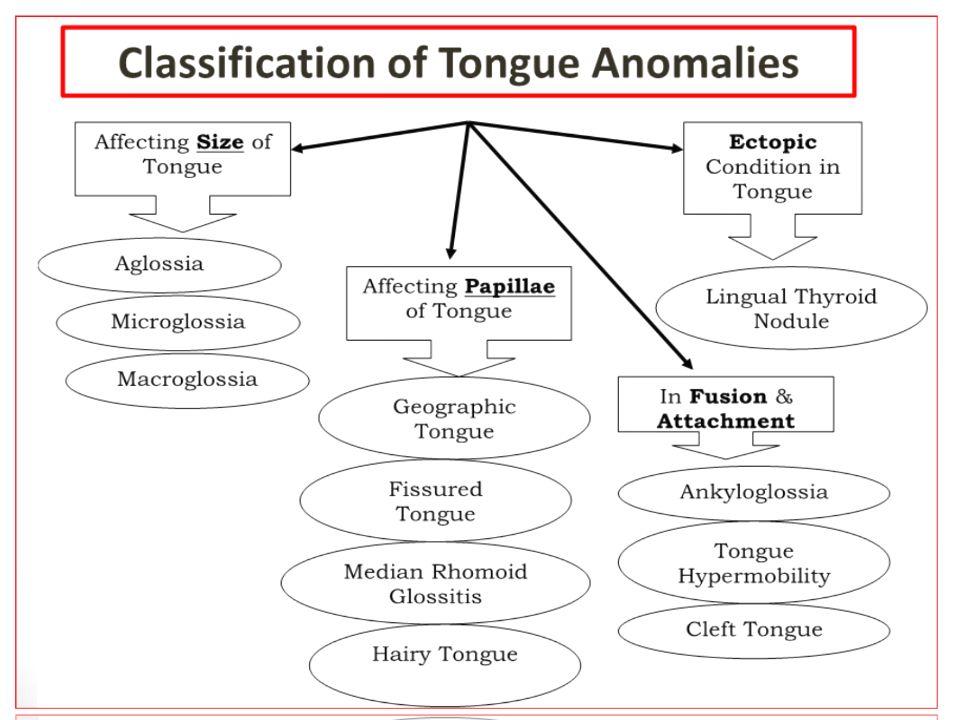
Main Points Discussed in this Lecture 1.Aglossia, microglossia & macroglossia (congenital & acquired). 2.clinical features of geographic tongue & its different names. 3.Pathogenesis, clinical & microscopic appearance of median rhomboid glossitis. 4.Causes & clinical features of fissured tongue. 5.Pathogenesis & appearance of hairy tongue. 6.Causes & clinical features of ankyloglossia. 7.Cause & appearance of tongue hypermobility. 8.Pathogenesis & types of bifid tongue. 9.Pathogenesis & clinical appearance of lingual thyroid nodule.

Similar presentations