Download presentation
Presentation is loading. Please wait.

1
MULTIPLE ENDOCRINE NEOPLASIA Dr. M. Sofi MD; FRCP (London); FRCPEdin; FRCSEdin
; FRCPEdin; FRCSEdin")
2
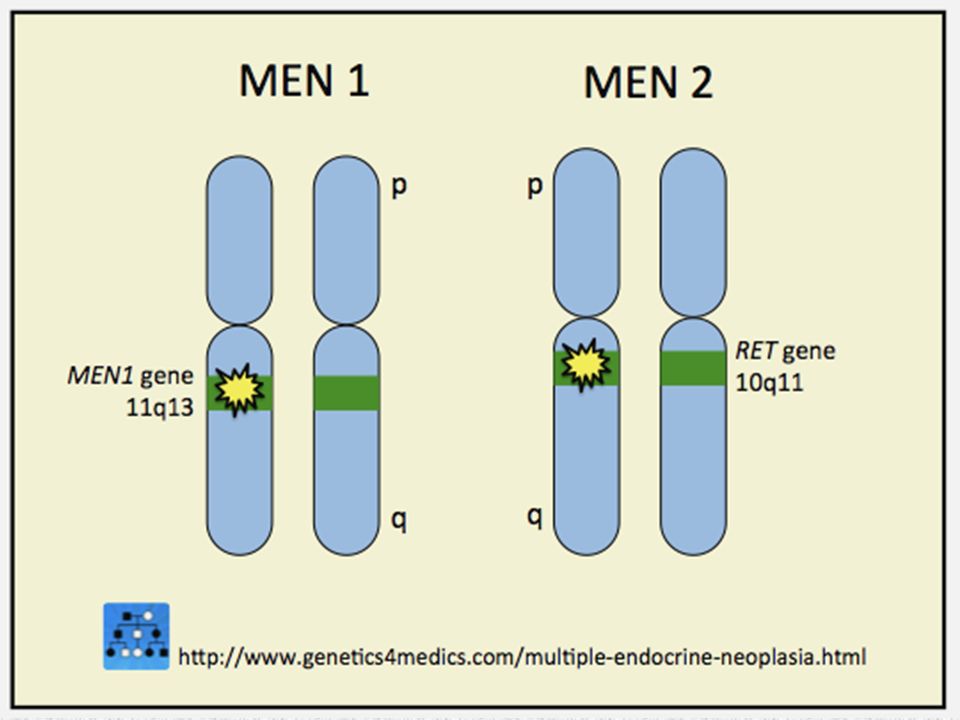
Multiple endocrine neoplasia (MEN) syndromes consist of rare, autosomal dominant mutations in genes that regulate cell growth. Classification recognizes: Type I & type II MEN Type II divided into the Type IIA Type IIB Menin protein: Produced by the MENIN gene, is a tumor suppressor. Loss of this protein allows tumors to arise. Ret protein: Produced by the RET gene proto-oncogene, can be constitutively activated, causing abnormal cell proliferation MULTIPLE ENDOCRINE NEOPLASIA

6
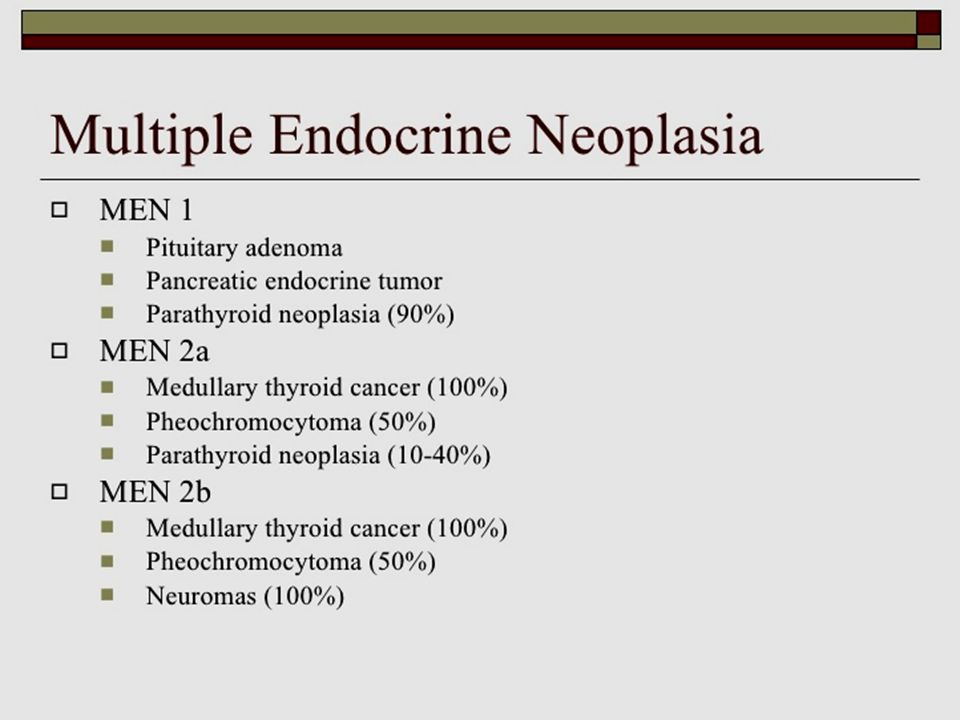
Type 1 MEN is hyperfunctioning following tumors: All 4 parathyroid glands Pancreatic islets gastrinoma insulinoma glucagonoma vasoactive intestinal peptide tumor (VIPoma) pancreatic polypeptide–producing tumor (PPoma) Anterior pituitary prolactinoma, somatotropinoma, corticotropinoma nonfunctioning tumors MULTIPLE ENDOCRINE NEOPLASIA
 pancreatic polypeptide–producing tumor (PPoma) Anterior pituitary prolactinoma, somatotropinoma, corticotropinoma nonfunctioning tumors MULTIPLE ENDOCRINE NEOPLASIA")
7
Type 1 MEN Other associated tumors include: – lipomas, – angiofibromas – located in the adrenal gland cortex (rarely, in the adrenal medulla). Hyperparathyroidism is the most common manifestation of type 1 MEN (80% of presentations) Islet-cell tumors that secrete predominantly gastrin are called gastrinomas; these tumors frequently metastasize Pheochromocytomas are reported in patients with type 1 MEN Thymic and bronchial carcinoid tumors can also be associated with type 1 MEN MULTIPLE ENDOCRINE NEOPLASIA
 Islet-cell tumors that secrete predominantly gastrin are called gastrinomas; these tumors frequently metastasize Pheochromocytomas are reported in patients with type 1 MEN Thymic and bronchial carcinoid tumors can also be associated with type 1 MEN MULTIPLE ENDOCRINE NEOPLASIA.")
8
Type 2A MEN is defined by: Thyroid carcinoma Pheochromocytoma (50 Hyperparathyroidism (20%) Familial MTC is hereditary MTC without other associated endocrinopathies Type 2A MEN (Sipple syndrome) accounts for most cases of type 2 MEN. Type 2 MEN affects about 1 in 40,000 individuals C-cell hyperplasia develops early in life and can be viewed as the precursor lesion for MTC, which often arises multifocally and bilaterally. Less than 25% of patients with type 2A MEN develop hyperparathyroidism Pheochromocytomas are bilateral in 70% of cases and develop on the background of adrenomedullary hyperplasia secondary to an RET germline mutation. MULTIPLE ENDOCRINE NEOPLASIA

9
Type 2B MEN is defined by: MTC Pheochromocytoma. Associated abnormalities include: – Mucosal neuromas – Medullated corneal nerve fibers – Marfanoid habitus MTC is relatively aggressive and frequently occurs in childhood Pheochromocytomas also occur earlier than in patients with type 2A MEN, and patients have the same features arising in the context of adrenomedullary hyperplasia, multifocality, and, often, bilateral involvement MULTIPLE ENDOCRINE NEOPLASIA

10
Type 1 MEN The MENIN gene responsible for type 1 MEN has been localized to chromosome band 11q13; It produces a nuclear protein called menin, a tumor suppressor. The MENIN gene is ubiquitously expressed and is localized to the nucleus of cells There is increasing evidence that menin may act in DNA repair or synthesis. Type 2 MEN The genetic mutation in type 2 MEN occurs in RET proto-oncogene, located on band 10q11.2 This gene defect has been observed in both MEN2A & MEN2B Activation of RET leads to hyperplasia of target cells in vivo. Subsequent secondary events then lead to tumor formation. RET is specifically expressed in neural crest–derived cells. Etiology

11
Type 1 MEN Hyperparathyroidism is most common initial clinical manifestation of type 1 multiple endocrine neoplasia (MEN). Some patients may manifest findings of ZES before they have hyperparathyroidism. Symptoms of gastrinoma may become clinically apparent either with abdominal pain and diarrhea or with complications such as ulcer perforation or bleeding. Type 2A MEN All patients develop MTC on the basis of C-cell hyperplasia. About 50% of patients with MTC manifest pheochromocytomas (usually late in life), and 20% of patients have hyperparathyroidism. Type 2B MEN Pheochromocytomas occur earlier than in patients with type 2A MEN. Clinical presentation
, and 20% of patients have hyperparathyroidism. Type 2B MEN Pheochromocytomas occur earlier than in patients with type 2A MEN. Clinical presentation.")
12
The age of onset of endocrine tumors is usually in the teenage years, but symptoms from these tumors may not appear for several years, and the diagnosis is frequently delayed until the fourth decade of life. Cutaneous tumors may develop prior to the manifestation of overt clinical symptoms resulting from endocrine tumors. The earliest cutaneous tumors appear in the teenage years Clinical presentation MEN Type 1

13
Pancreatic endocrine tumors These occur in about 70% of patients with MEN1. 60% of tumors are gastrinomas and produce ZES PU account for most of the MEN1 morbidity and mortality About 30% are insulinomas. VIPoma (vasoactive intestinal peptide and pancreatic polypeptide-secreting tumor) Duodenal microgastrinoma is very common and probably accounts for almost half of all MEN1-associated gastrinomas. They are usually multiple, with up to 15 separate tumors. Clinical presentation MEN Type 1
 Duodenal microgastrinoma is very common and probably accounts for almost half of all MEN1-associated gastrinomas. They are usually multiple, with up to 15 separate tumors. Clinical presentation MEN Type 1.")
14
Pituitary adenomas Present by screening in 30% of patients, but is found at post-mortem in 50%. Unlike the pancreas and parathyroid, there does not appear to be diffuse pituitary hyperplasia. Prolactinoma producing hyperprolactinaemia occurs in about 30% of cases. They tend to be more aggressive than sporadic cases. Acromegaly, due to excessive human growth hormone (hGH) occurs in about 30%. Adrenocorticotrophic hormone(ACTH) may produce Cushing's syndrome but other functioning tumors are rare. Clinical presentation MEN Type 1
 occurs in about 30%. Adrenocorticotrophic hormone(ACTH) may produce Cushing s syndrome but other functioning tumors are rare. Clinical presentation MEN Type 1.")
15
Skin lesions Occur in nearly 90% of patients, but they can be easily overlooked. Benign tumors include multiple angiofibromas, collagenomas, and lipomas. They should be sought because they can act as markers for this syndrome. Other lesions Lesions in other tissues have been reported, but their relationship remains controversial. Carcinoid tumours of the foregut, midgut, and thymus occur in about 10%, and are often found in the pancreas, but they are rarely symptomatic. Clinical presentation MEN Type 1

16
Screening of first- and second-degree relatives type 1 (MEN1) Diagnosis of MEN1 depends on high level of suspicion in patients with multiple Facial angiofibromas, Collagenomas, and lipomas Features hyperparathyroidism High gastric acid secretion. Investigations include: Hormone hypersecretion Imaging studies for the presence of tumors. DNA testing is available and identifies a mutation in about 80% of patients with familial MEN1. Mutation analysis may be used to confirm the clinical diagnosis, Screen asymptomatic family members. Prenatal diagnosis for pregnancies at increased risk is possible if the disease-causing mutation in a family is known Diagnosis MEN type 1

17
Radiographic views of the hands in a patient with type 1 (MEN1) and primary hyperparathyroidism. These images show subperiosteal bone resorption along the radial aspects of the middle phalanges. Imaging features MEN Syndrome

18
CT scan of the pancreas in a patient with type 1 (MEN1) and a gastrinoma. Image shows a pancreatic head mass (large, white arrow), as well as a low-attenuating lesion in the liver (small, black arrowhead) that indicates metastases. Calcifications of the right renal medullary pyramids (medullary nephrocalcinosis; black arrows) in this nonenhanced CT scan. Imaging features MEN Syndrome
, as well as a low-attenuating lesion in the liver (small, black arrowhead) that indicates metastases. Calcifications of the right renal medullary pyramids (medullary nephrocalcinosis; black arrows) in this nonenhanced CT scan. Imaging features MEN Syndrome.")
19
CTscan image with oral and intravenous contrast in a patient with biochemical evidence of insulinoma. The 3-cm contrast- enhancing neoplasm (arrow) is seen in the tail of the pancreas (P) posterior to the stomach (S) Imaging features MEN Syndrome
 is seen in the tail of the pancreas (P) posterior to the stomach (S) Imaging features MEN Syndrome.")
20
6x5x5 cm adrenal mass arising from right adrenal Imaging features MEN Syndrome

21
The screening of first- and second-degree relatives of patients with (MEN1) is aimed at early detection of parathyroid, pancreatic or pituitary lesions in gene carriers, to reduce the associated morbidity. There is no evidence that screening reduces mortality Identification of affected individuals in 'malignant kindred' with aggressive pancreatic disease may allow curative surgery which would be expected to prolong survival. Screening lowers the age of detection of the syndrome by about 20 years. Screening tests MEN type 1

22
Screening tests are: serum calcium, fasting gastrin, prolactin. Sensitive markers of pancreatic disease are basal and test- meal stimulated pancreatic polypeptide and gastrin, and basal insulin and proinsulin. 80% of affected individuals will have been identified by the 5th decade. Screening of sporadic pancreatic endocrine tumors for evidence of MEN1 is probably justified, especially for gastrinomas or insulinomas. There is little evidence to support screening in those with sporadic pituitary tumors. Screening tests MEN type 1

23
If the condition is confirmed, then genetic counseling is required Pharmacological Diazoxide can be used to inhibit release of insulin, especially in tumors that are beyond surgery. High-dose proton pump inhibitors are required for gastrin-secreting tumors. After surgery to the pituitary, hormone replacement may be required Management

24
Surgical Skin tumors may be removed The surgical approach to pancreatic endocrine tumors in MEN1 is controversial: – Surgical cure is best achieved by removing the pancreas and duodenum with adjacent lymph nodes. There is still a high rate of recurrence but the overall mortality remains low Pituitary tumors: Same as for sporadic pituitary tumors. Parathyroidectomy, subtotal or complete, is practiced for MEN1 but long-term follow-up reveals a high rate of recurrence in MEN1. The treatment of metastatic disease is the same as in sporadic cases. Management

25
The average age of death in individuals with multiple endocrine neoplasia type 1 (MEN1) is significantly lower (55.4 years for men and 46.8 years for women) than that of the general population. Pancreatic endocrine tumors, particularly gastrinomas, become malignant in about 50% of patients with MEN1. Untreated, patients may die from peptic ulcer disease, metastatic endocrine pancreatic carcinoma, or foregut carcinoid malignancy. Pancreatic endocrine tumors associated with MEN1 are less malignant than sporadic tumors and carry a better prognosis, with a median survival of 15 years compared to 5 years for patients with sporadic tumors. This may reflect more indolent disease or earlier diagnosis. Prognosis MEN type 1

26
Patients may present with symptoms related to: – Medullary thyroid carcinoma – Hyperparathyroidism – Pheochromocytoma. Virtually all patients have MCT symptoms may include: hypertension episodic sweating diarrhoea pruritic skin lesions lump in the neck(which may cause compressive symptoms). Clinical presentation MEN Type 2A
. Clinical presentation MEN Type 2A.")
27
25% of MEN Type 2A have Hperparathyroidism and associated hypercalcemia may lead to: Polyuria Polydipsia constipation memory problems depression, nephrolithiasis Cutaneous lichen amyloidosis in multiple endocrine neoplasia type 2A (MEN2A) presents with multiple pruritic, hyperpigmented, lichenoid papules in the scapular area of the back. Clinical presentation MEN Type 2A

28
Patients may present with symptoms related to: – Medullary thyroid carcinoma – Pheochromocytoma. – Neuromas usually predate MTC and phaeochromocytoma. Almost all patients have a Marfan's-like habitus. Neuromas appear as: – Glistening bumps around the lips, tongue, and mouth. – Bumps on the eyelids, which are often thickened Involvement of peripheral motor and sensory nerves can cause a peroneal muscular atrophy (Charcot-Marie-Tooth syndrome) Intestinal ganglioneuromatosis affects about 75% of cases. Delayed puberty is a common feature. Clinical presentation MEN Type 2B
 Intestinal ganglioneuromatosis affects about 75% of cases. Delayed puberty is a common feature. Clinical presentation MEN Type 2B.")
29
MULTIPLE ENDOCRINE NEOPLASIA Mucosal neuromas

30
Screening for pheochromocytoma is 24 hours urine for elevated catecholamines and catecholamine metabolites, especially vanillyl-mandelic acid (VMA). Clinical suspicion or elevated urinary catecholamine values demand an abdominal MRI scan. A metaiodobenzylguanidine (MIBG) scan is useful for localizing pheochromocytomas. Thyroid tumours can be investigated initially by ultrasound and fine-needle aspiration. Diagnosis of multiple endocrine neoplasia type 2
 scan is useful for localizing pheochromocytomas. Thyroid tumours can be investigated initially by ultrasound and fine-needle aspiration. Diagnosis of multiple endocrine neoplasia type 2.")
31
Medullary thyroid carcinoma (MTC) is suspected with an elevated plasma calcitonin concentration. This is a specific and sensitive marker. In provocative testing, calcitonin concentration is measured before and 2 and 5 minutes after intravenous administration of calcium. Parathyroid abnormalities are diagnosed when there are simultaneously elevated serum calcium and parathyroid hormone levels with an elevated urinary calcium to creatinine ratio. Diagnosis of multiple endocrine neoplasia type 2

32
The two types of molecular diagnosis for MEN2 are: Mutation and Linkage analysis of the RET proto-oncogene (chromosomal locus 10q11) Genetic linkage analysis has 98-99% predictive accuracy Screening for early detection of thyroid, parathyroid and adrenal disease, reduces both morbidity and mortality in MEN2: Recurrence of medullary thyroid carcinoma (MTC) should be monitored with – Calcitonin – Carcinoembryonic antigen (CEA) – Provocative calcitonin testing with the pentagastrin stimulation test, with serial measurements of serum calcitonin measured. False-positive and false- negative results have been reported Screening for multiple endocrine neoplasia type 2

33
General principles Identify individuals with germline RET-disease- causing mutations associated with MEN2 before symptoms develop. Reduce morbidity and mortality in the highest-risk Prophylactic thyroidectomy Screening for MTC Phaeochromocytoma screening and parathyroid disease before symptoms develop. Counseling of patients with MEN The treatment for adrenal medullary hyperplasia or phaeochromocytoma is bilateral adrenalectomy. Total thyroidectomy for patients as young as 3 years for MEN2A if they contain the genetic mutation. Hyperparathyroidism: subtotal parathyroidectomy is advised, along with cervical thymectomy because of the increased risk of supernumerary parathyroid glands. Management MEN type 2

34
In MEN 2B, thyroidectomy with lymph node clearance should be performed at the earliest possible age. MTC is biologically aggressive in these patients and has been reported as early as 15/12 age. Patients with the genetic mutation for MEN2B, total thyroidectomy is recommended in infancy. Patients not identified by screening, thyroidectomy should still be performed. Prognosis Patients with MEN2B tend to do worse than those with MEN2A The prognosis is poor with recurrent disease in about 20% of patients in clinically occult but macroscopic MTC It is particularly poor in MEN2B who present with clinically apparent MTC. Their 10-year survival is about 50%, and death from metastatic disease in the mid-twenties is common Management MEN type 2B

35
Initial thyroid lesion in MEN2 is C-cell hyperplasia, which has been found as early as the age of 3 years in MEN2A and may be present at birth in MEN2B. Over the subsequent 5 to 10 years microscopic MTC develops and finally gross tumors become apparent. MTC typically presents as a neck mass or neck pain at about age 15 to 20 years. More than 50% already have cervical lymph node metastases. Inherited MTC accounts for 25% of cases in association with MEN types 2A and 2B, but non-MEN familial MTC also occurs. It may present with a thyroid lump. Diarrhoea may also occur. Metastases may occur, to the lung, liver and bone. Paraneoplastic syndromes are rare but may include Cushing's or carcinoid syndrome. Medullary Thyroid carcinoma

36
Phaeochromocytoma occurs in 50% of MEN2. In patients with MEN2 are usually found in the adrenals About 70% are bilateral, almost all are benign. They produce excessive adrenaline secretion leading to tachycardia, palpitations, hypertension and headache. Investigations include plasma concentrations of free metanephrines, and imaging CT or MRI Positron emission tomography (PET) is also used for diagnosis. Treatment surgical, laparoscopic surgery is increasingly used. Overall, half of the patients with malignant pheochromocytomas remain alive for five years. Pheochromocytoma
 is also used for diagnosis. Treatment surgical, laparoscopic surgery is increasingly used. Overall, half of the patients with malignant pheochromocytomas remain alive for five years. Pheochromocytoma.")
Similar presentations




 are derived from the diffuse neuroendocrine system, which is made up of.>")















. Swedish Medical Student Discovered Parathyroid gland In 1880 Last major organ Identified in humans.>")