Download presentation
Presentation is loading. Please wait.

2
R40: 30 yo man found unconscious, on ambo arrival VT. ROSC after single DC shock In ED conscious, mildly intoxicated Normal bloods, CXR, alcohol 44 12 Lead ECG:

4
Admitted under medicine, monitored Several codes for non sustained VT’s

6
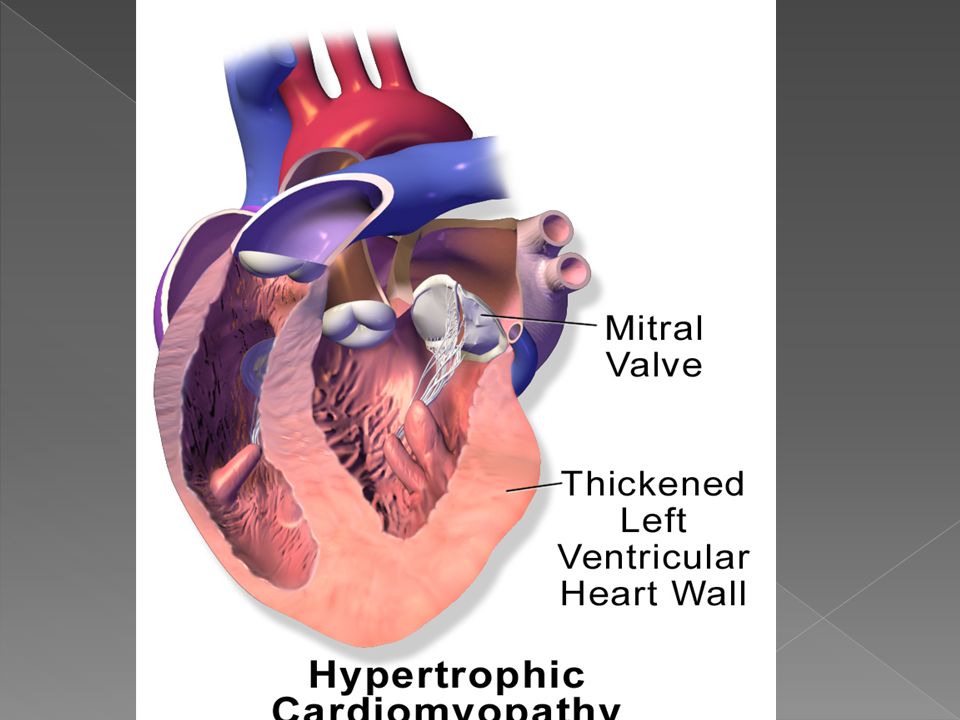
Assymetrical septal hypertrophy 1% of all cardiology FUP clinics Most common genetic cardiac disease Prevalence in adults 0.2% Prim myocardial abnormality w sarcomeric disarray and assym LV hypertrophy

7
50% AD- > 450 mutations Acquired ( athletes, on/off exercise) Unknown ???? environmental
 Unknown environmental")
9
Dynamic LVOTO, ant motion of MV septum ( SAM- systolic anterior motion) hypertrophied septum - subaortic obstruction Pressure overload of LV, diastolic Dysfunction MR Arrhythmia MI Sudden cardiac death
 hypertrophied septum - subaortic obstruction Pressure overload of LV, diastolic Dysfunction MR Arrhythmia MI Sudden cardiac death")
10
Widely variable Subaortic obstr, dynamic, contractility and loading, location LVOTO assoc. with incr. wall stress, fibrosis VT/VF SAM worse with inc. contractility, reduced pre or afterload MI - ? Small CA, partially obliterated by hypertrophy/ too much muscle for small vessells

12
Athletes Concentric, regresses w deconditioning Wall thickness <15 mm LA <40mm LVEDD >45mm 2% of elite athletes HCM ? Asymmetric >15mm LA<45mm LVEDD < 45mm Abn diast function

13
Dyspnoea on exertion (90%) CCF- orthopnea, PND Angina ( 70-80%) Syncope (20%) Palpitations Sudden cardiac death
 CCF- orthopnea, PND Angina ( 70-80%) Syncope (20%) Palpitations Sudden cardiac death")
14
Diagnostic features usually present by 21 years < 12 years: morphological features unlikely

15
Evidence of CCF Jerky pulse Paradoxically split S2 ( if high LVOT gradient) Prominent A wave of JVP (red. RV compliance)
.")
16
ESM betw. apex and sternum SS notch, NOT carotid, quiet-squatting, loud with less pre/after load MR Holosystolic murmur at apex+ axilla AR diastolic decrescendo murmur

18
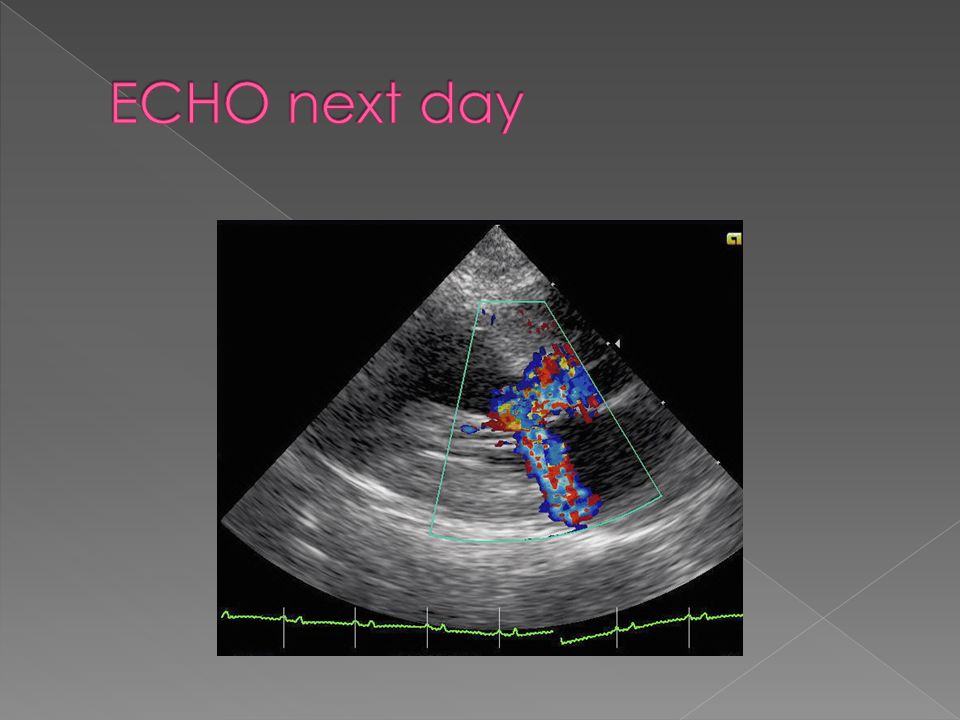
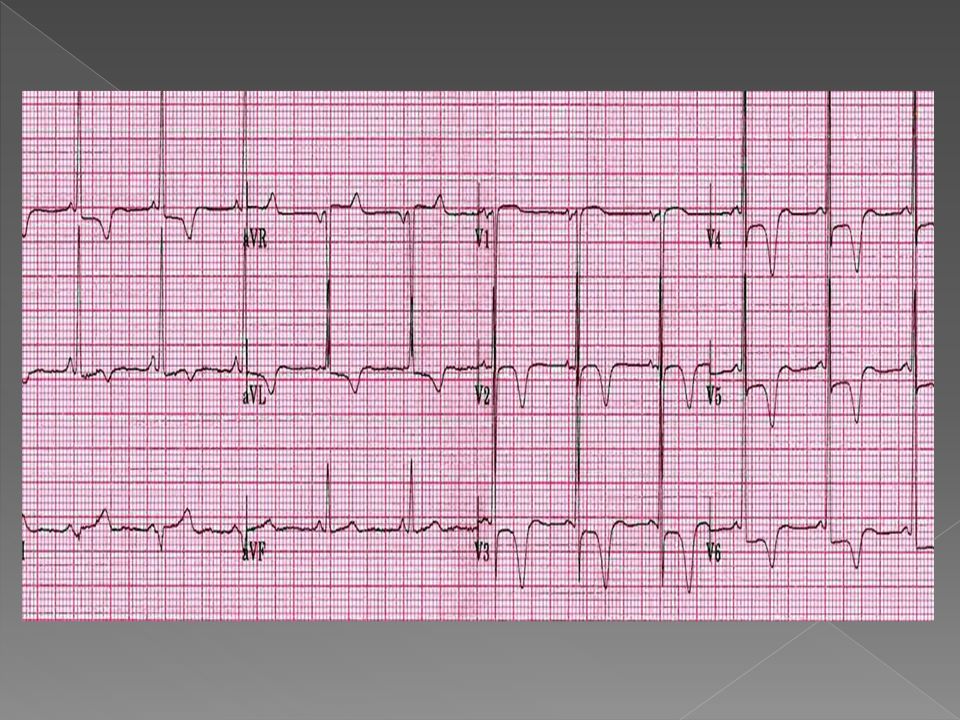
LVH, LAD, deep ant/lat TWI, Dagger like Q waves inf/lat CXR- left atrial enlargement ( or normal) ECHO- septal hypertrophy, SAM, early aortic closure Cardiac catheter( DD CAD, severe MR
 ECHO- septal hypertrophy, SAM, early aortic closure Cardiac catheter( DD CAD, severe MR")
19
Pharmacology B blockers. –ve inotrope, low HR, low O2 demand, longer diastolic filing, less exercise intolerance and dyspnoea disopyramide -ve inotrope

20
Surgical- indic: subaortic gradient >50mmHg Septal myotomy/ myectomy Complication: 2% perforation or CHB, 3% mortality Non surgical ablation (10% CHB) ICD- Arrhythmia ( SCD, FH of, VT/VF, age <30) transplant
 ICD- Arrhythmia ( SCD, FH of, VT/VF, age <30) transplant")
21
31 y/o man BIB ambulance, celebrated his 31 st birthday, fell under influence of alcohol. Ankle fracture dislocation with compromise of foot circulation History: previous VT arrest because of HCM. Missed appointment for ICD insertion….

22
Avoid worsening of subaortic gradient, tachycardia, vasodilatation or inotropes Aim to increase pre/after load, reduce contractility

23
Volume Induction: narcotics, propofol Avoid tachycardia, Inotropes, Calcium, B agonist

Similar presentations




















 CPP = aortic diastolic.>")

