Download presentation
Presentation is loading. Please wait.

1
Anaphylaxis: Dr Rasol Molatefi, Fellow Of Allergy And Clinical Immunology

3
Definition: Risk factors: Causes: Pathophysiology: Signs and symptoms: Treatment: Follow up:

4
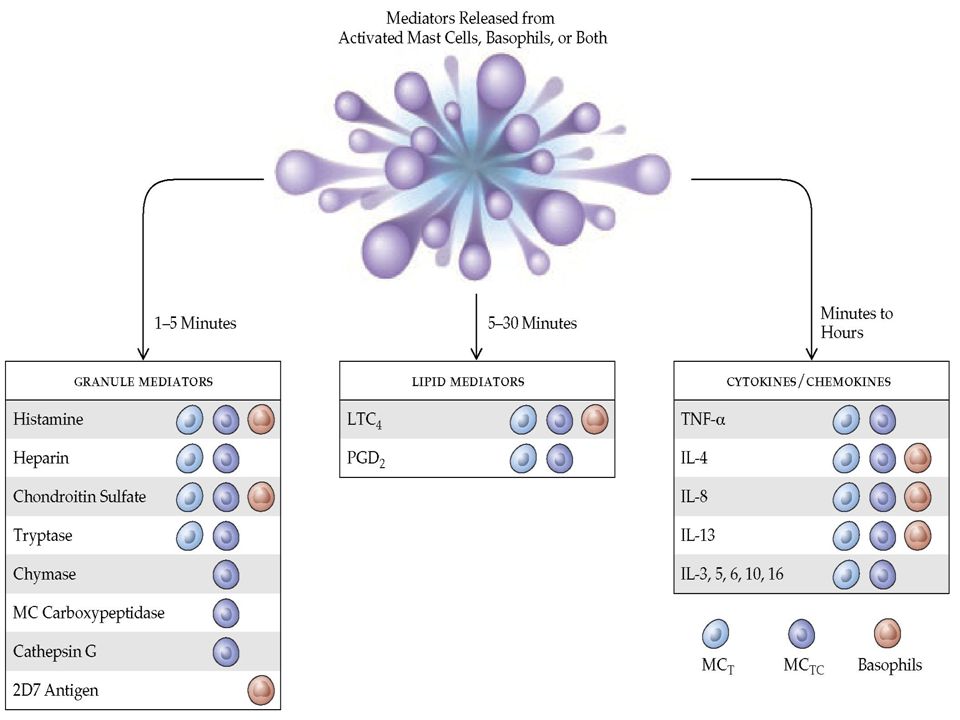
Immunopathology: types 1 : IgE Mediated 2: IgG and IgM mediated 3: Immune complex mediated 4: T Cell mediated 5: activating or inactivating Ab 6: Tc mediated 7: Granuloma formation

8
Prevalence: USA : 0.5 – 2 % in life time Prevalence is increasing Iran: ?

9
Risk factors: Age: adults ;radio contrast media, plasma expanders, anesthetics Socioeconomic Status Gender Route of Administration Constancy of Administration Time since last Reaction Atopy Geographic Location Asthma Exercise, inflammation, alcohol, NSAID Mastocytosis

10
Causes: Food: Drugs: Antibiotics, NSAIDs, … Latex Perioperative anaphylaxis : Muscle relaxants account for 62% and latex 16%;… Radiocontrast media Hymenoptera stings Antisera Hemodialysis Biologic agents: ……mab Idiopathic anaphylaxis: 2/3 of adults, minority of children

12
Drug allergy risk factor: Dose Route Intermittent Inflammation state History / cross reaction Gene Multiple drug use

13
Time: Ingestion: 5 - 30 min. P.O.: 30 min – 2 hour Biphasic: Protracted:

14
Signs and symptoms: Skin: flushing, itching, urticaria, angioedema Respiratory: dysphonia, cough, stridor, wheezing, dyspnea, chest tightness, asphyxiation, death GI: nausea, vomiting, bloating, cramping, diarrhea Cardiovascular: tachycardia, hypotension, dizziness, collapse, death Upper respiratory tract: Rhinitis, congectivitis Genitalia: pruritus Organ failure: Other: feeling of impending doom, metallic taste Infants: Un common: syncope, fibrinolysis, DIC, adrenal hemorrhage

15
Frequency of signs and symptoms:

16
Risk factor for death: Severety Age Comorbidity More Acute onset Injection Unavailability of epinephrin

23
No skin signs: risk factors Infants Severe forms Perioperative, Fire ant Mastocytosis

25
Hypotension: causes Hypovolemic Diffusional Heart failure Vagal tone Collapse : 5 min for injection 15 min for sting 30 min for food

26
Definition: first scenario no allergy history 1. Acute onset of an illness (minutes to several hours) with involvement of the skin, mucosal tissues, or both (e.g., generalized hives, pruritus or flushing, swollen lips-tongue-uvula) And at least one of the following: a. Respiratory compromise (e.g., dyspnea, wheeze, bronchospasm, stridor, reduced PEF, hypoxemia) b. Reduced BP or associated symptoms of end- organ dysfunction (e.g., hypotonia [collapse], syncope, incontinence)
 with involvement of the skin, mucosal tissues, or both (e.g., generalized hives, pruritus or flushing, swollen lips-tongue-uvula) And at least one of the following: a. Respiratory compromise (e.g., dyspnea, wheeze, bronchospasm, stridor, reduced PEF, hypoxemia) b. Reduced BP or associated symptoms of end- organ dysfunction (e.g., hypotonia [collapse], syncope, incontinence).")
27
Definition: second scenario: exposure to likely allergen. a. Involvement of skin-mucosal tissue (e.g., generalized hives, itch-flush, swollen lips-tongue-uvula) b. Respiratory compromise (e.g., dyspnea, wheeze bronchospasm, stridor, reduced PEF, hypoxemia) c. Reduced BP or associated symptoms of end-organ dysfunction (e.g., hypotonia [collapse], syncope, incontinence) d. Persistent gastrointestinal symptoms (e.g., crampy abdominal pain, vomiting)
 b. Respiratory compromise (e.g., dyspnea, wheeze bronchospasm, stridor, reduced PEF, hypoxemia) c. Reduced BP or associated symptoms of end-organ dysfunction (e.g., hypotonia [collapse], syncope, incontinence) d. Persistent gastrointestinal symptoms (e.g., crampy abdominal pain, vomiting).")
28
Definition: third scenario: known allergen Reduced BP after exposure to known allergen for that patient (minutes to several hours): a. Infants and children: low systolic BP (age specific) or greater than 30% decrease in systolic BP* b. Adults: systolic BP less than 90 mm Hg or greater than 30% decrease from their baseline
 or greater than 30% decrease in systolic BP* b. Adults: systolic BP less than 90 mm Hg or greater than 30% decrease from their baseline.")
30
D.D.: flushing Wet: menopausal women, spicy foods dry flush: carcinoid syndrome, pancreatic tumors, thyroid medullary carcinoma Alcohol-induced flushing: aldehyde accumulation ± drug: cephalosporin's, disolfiram, griseofulvin ± disease: menopause, malignancy, hyper eo, mastocytosis, …

31
D.D.: Monosodium glutamate: Chinese restaurant

32
D.D.: Scomboroidosis

33
Laboratory: Tryptase beta Histamin ……… Post mortem: tryptase, specific IgE

34
Treatment : Removal of the inciting antigen, if possible (eg, stop infusion of a suspect medication) Call for help Intramuscular injection of epinephrine Placement of the patient in the supine position with the lower extremities elevated, or if dyspneic or vomiting, placement of the patient semi-recumbent with lower extremities elevated Supplemental oxygen Volume resuscitation with intravenous fluids
 Call for help Intramuscular injection of epinephrine Placement of the patient in the supine position with the lower extremities elevated, or if dyspneic or vomiting, placement of the patient semi-recumbent with lower extremities elevated Supplemental oxygen Volume resuscitation with intravenous fluids")
35
TREATMENT ERRORS: Epinephrine should be administered as soon as possible once anaphylaxis is recognized. Delayed administration has been implicated in contributing to fatalities. H1 antihistamines are useful for relieving itching and urticaria. They do NOT relieve stridor, shortness of breath, wheezing, gastrointestinal symptoms and signs, hypotension or shock, and should not be substituted for Epinephrine Bronchodilator treatment with nebulized Albuterol should be given in individuals with severe bronchospasm, as an adjunctive treatment to Epinephrine. However, albuterol does NOT prevent or relieve upper airway edema, hypotension or shock and should not be substituted for epinephrine in the treatment of anaphylaxis. Glucocorticoids theoretically reduce the late phase response. They do not relieve the initial symptoms of anaphylaxis.

38
Observational period: Can be discharged after complete resolution of symptoms Some patients should be under observe for longer period: 8 to 24 hours after resolution of symptoms: Moderate to severe reaction Episode in asthmatic patient with wheezing Ingested antigen with possibility of continued absorption Previous history of biphasic response

39
In discharge: patient should know They have experienced anaphylaxis or "killer allergy," which is a life-threatening condition. Symptoms of the current episode may recur up to three days after the initial onset of symptoms. They should self-inject epinephrine, and call emergency medical services or get to the nearest emergency facility at the first sign of recurrence of symptoms. They are at risk for repeat episodes of anaphylaxis in the future. Prednisolone, Anti H 1+ 2 for few days !!

42
When administer Epipen at home: Signs of anaphylaxis After use of allergen: if there is history of very severe anaphylaxis

44
Drugs that should not be used in patients with Anaphylaxis history: Adrenergic blocker ACE inhibitor Angiotensin receptor blockers: losartan MAO inhibitor: tranylcypromine, moclobemide, phenelzine Some tricyclic antidepressants: imipramine

Similar presentations





























 type I.>")







