Download presentation
Presentation is loading. Please wait.

2
The lateral-flow assay (LFA) or lateral flow immunochromatographic assay, introduced in 1988 by Unipath, is the commonest commercially available POC diagnostic format. Point-of-care (POC) diagnostics, in vitro diagnostic (IVD) tests that do not involve the use of laboratory sta ff and facilities to provide the result.
 diagnostics, in vitro diagnostic (IVD) tests that do not involve the use of laboratory sta ff and facilities to provide the result..")
3
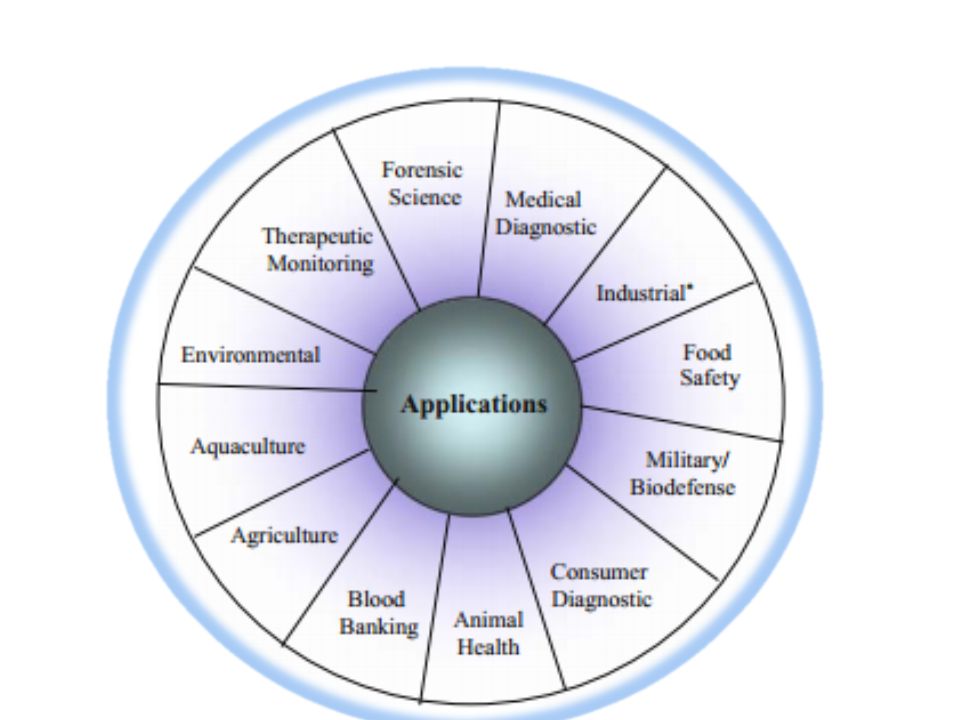
Lateral flow (immuno)assays are currently used for qualitative, semiquantitative and to some extent quantitative monitoring in resource-poor or non- laboratory environments. LFA devices used for pregnancy (using hCG levels) and ovulation confirmation, screening for infectious diseases and drugs of abuse, and for measurement of protein markers in blood to aid rapid clinical diagnostics of life-threaten ing events such as heart attack, stroke, and deep-vein thrombosis.
 and ovulation confirmation, screening for infectious diseases and drugs of abuse, and for measurement of protein markers in blood to aid rapid clinical diagnostics of life-threaten ing events such as heart attack, stroke, and deep-vein thrombosis..")
5
The best-known and common application is the pregnancy test Results usually come within 10–20 min. The current generation of LFAs has high sensitivity, selectivity and ease of use LFIAs use of nearly the same components as in enzyme immunoassays was reported

6
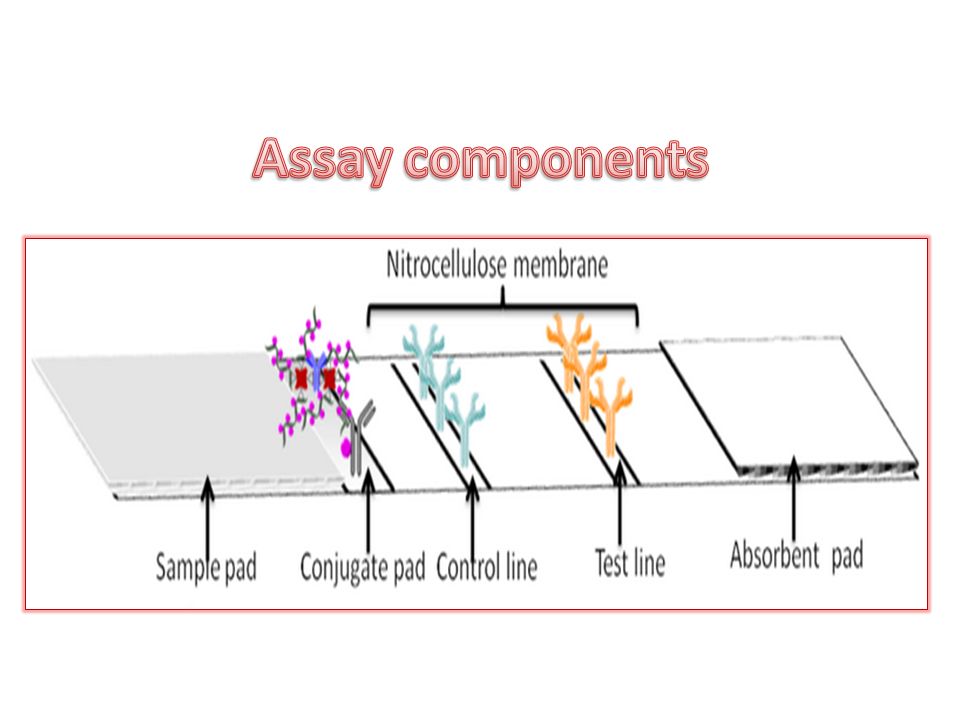
1. The Membrane/Analytical Region: to bind proteins at the test and control areas and to maintain their stability and activity over the shelf-life of the product. Nitrocellulose membranes are traditionally used, other materials such as nylon and polyvinylidene fluoride (PVDF) membranes are introduced but with limited success. Characteristics of nitrocellulose membranes include: relatively low cost, true capillary flow characteristics, high protein-binding capacity, relative ease of handling
 membranes are introduced but with limited success. Characteristics of nitrocellulose membranes include: relatively low cost, true capillary flow characteristics, high protein-binding capacity, relative ease of handling.")
8
2. The Conjugate Pad: The role of the conjugate pad in a lateral flow immunoassay is to accept the conjugate, hold it stable over its entire shelf life, and release it efficiently and reproducibly when the assay is run. Because of the nature of the materials used, it is often necessary to pre-treat conjugate pads to ensure optimal release and stability. Pretreatment is performed by immersion of the pad in aqueous solutions of proteins, surfactants, and polymers, followed by drying.

9
The addition of conjugates to the treated pad is a critical step for the final performance of the test. Two methods are typically used: – The first is immersion of the treated conjugate pad into the conjugate suspension. – The second is dispensing with quantitative non- contact dispensers The most commonly used labels include colloidal gold and monodisperse latex, tagged with either a visual or a fluorescent dye

10
3. The Sample Pad The role of the sample pad is to accept the sample, treat it such that it is compatible with the assay, and release the analyte with high efficiency. Sample treatments include: – filtering out of particulates or red blood cells – changing the pH of the sample, actively binding sample components that can interfere with the assay – and disrupting matrix components, such as mucins, in order to release the analyte to the assay.

11
Sample types can be as diverse as whole blood, serum, plasma, urine,.....and sputum depending on application area 5. Backing Materials All components of the lateral flow assay are laminated to the backing material to provide rigidity and easy handling of the strip The backing material is coated with a pressure-sensitive adhesive to hold the various components in place. The backing materials are typically polystyrene or other plastic materials coated with a medium to high tack adhesive.

12
6. Labels for Detection The most commonly used particulate detector reagents in lateral flow systems are colloidal gold and monodisperse latex. Latex particles coupled with a variety of detector reagents, such as colored dyes, fluorescent dyes, and magnetic or paramagnetic components, are available commercially. 7. The Wick The wick is the engine of the strip. It is designed to pull all of the fluid added to the strip into this region and to hold it for the duration of the assay It should not release this fluid back into the assay or false positives can occur. It is made of a high-density cellulose.

16
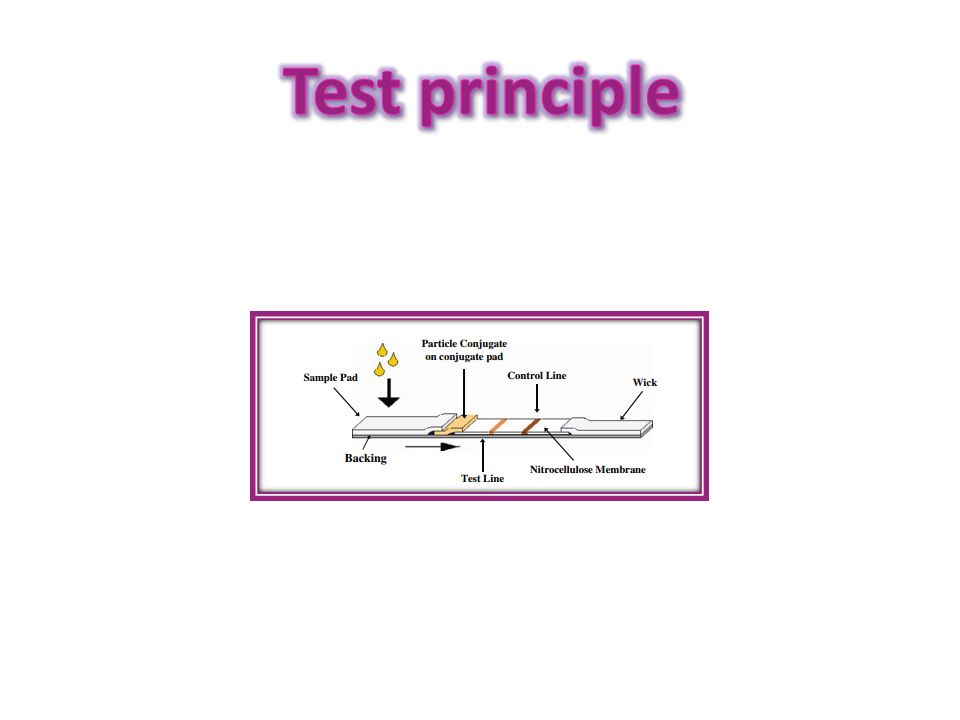
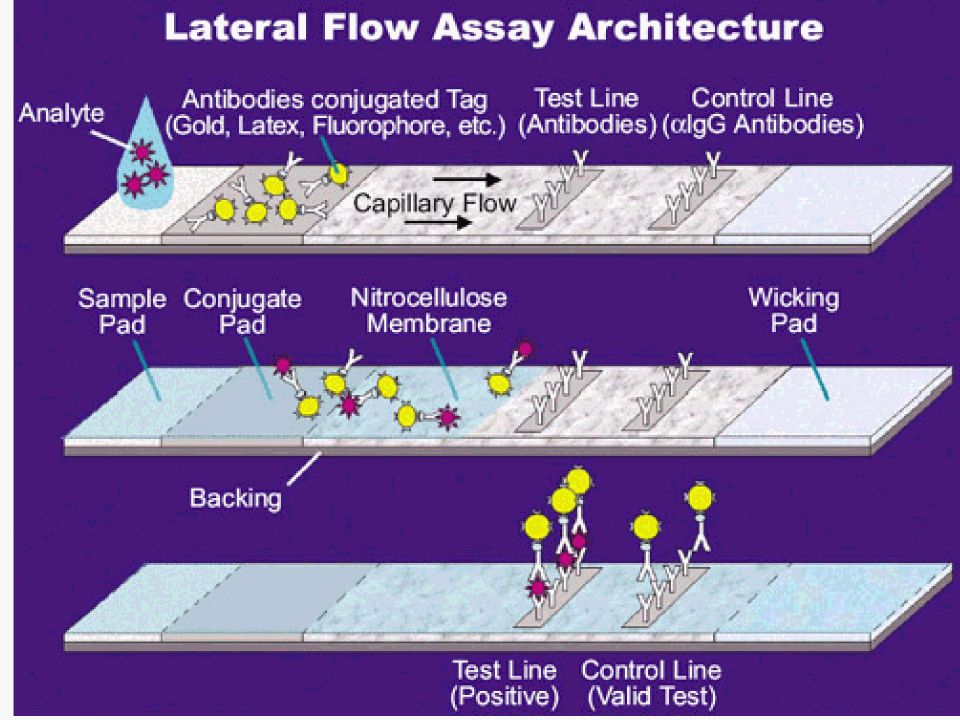
The assay consists of several zones, typically constituted by segments made of different materials. When a test is run, sample is added to the proximal end of the strip, the sample pad. The sample migrates through this region to the conjugate pad, where a particulate conjugate has been immobilized.

17
The particle can typically be colloidal gold, or a colored, fluorescent, or paramagnetic monodisperse latex particle, This particle has been conjugated to one of the specific biological components of the assay, either antigen or antibody depending on the assay format. The sample re-mobilizes the dried conjugate, and the analyte in the sample interacts with the conjugate as both migrate into the next section of the strip, which is the reaction matrix.

18
This reaction matrix is a porous membrane, onto which the other specific biological component of the assay has been immobilized. These components are typically proteins, either antibody or antigen, which have been laid down in bands in specific areas of the membrane where they serve to capture the analyte and the conjugate as they migrate by the capture lines

19
Excess reagents move past the capture lines and are entrapped in the wick or absorbent pad. Results are interpreted on the reaction matrix as the presence or absence of lines of captured conjugate, read either by eye or using a reader The control line e typically comprises a species-specific anti-immunoglobulin antibody, specific for the antibody in the particulate conjugate.

24
hCG semiquantitative measurement ?!! A simple strip design can give satisfactory semiquantitative results, a feature exploited by the recently developed “digital” pregnancy test system wherein measurement of optical density on the capture zone is used to estimate the hCG concentration in the sample, providing both an indication of pregnancy and an estimate of the time since implantation

25
Relative ease of manufacture. Stable shelf lives of 12–24 months often without refrigeration Ease of use. Can handle small volumes of multiple sample types Can be integrated with on board electronics, reader systems, and information systems Can have high sensitivity, specificity, good stability Relatively low cost Market presence and acceptance – minimal education required for users and regulators

26
Unclear patent situation Miniaturization of sample volume requirements below microliter level Multiplexing: simultaneous analysis of multiple markers difficult Integration with on board electronics and built-in QC functions challenging Sensitivity issues in some systems Test-to-test reproducibility challenging – limits applications in quantitative systems

27
Human chorionic gonadotropin (hCG) is a glycoprotein hormone secreted by the developing placenta shortly after fertilization. In normal pregnancy, hCG can be detected in serum as early as 7 days following conception. The concentration of hCG continues to rise rapidly, frequently exceeding 100 mIU/ml by the first missed menstrual period and peaking in the 30-200,000 mIU/ml range by 10-12 weeks into pregnancy

28
hCG can also be detected in urine as early as 14 days after conception (approximately 28 days since the last menstrual cycle), doubling in concentration about every two days until it peaks at approximately 8-10 weeks after the last menstrual period Recent studies suggest that urine hCG concentrations are approximately one half of, or less than one-half of corresponding serum hCG concentrations. The appearance of hCG soon after conception and its subsequent rise in concentration during early gestational growth make it an excellent marker for the early detection of pregnancy.

29
Human chorionic gonadotropin can be used as a tumor marker as its β subunit is secreted by some cancers including hydatidiform mole formation, testicular cancer. In a normal pregnancy, the β-HCG level doubles every 48- 72 hours until it reaches 10,000-20,000mIU/mL. In ectopic pregnancies, β-HCG levels usually increase less. Mean serum β-HCG levels are lower in ectopic pregnancies than in healthy pregnancies. No single serum β-HCG level is diagnostic of an ectopic pregnancy. Serial serum β-HCG levels are necessary to differentiate between normal and abnormal pregnancies and to monitor resolution of ectopic pregnancy once therapy has been initiated.

30
An ectopic pregnancy, or eccysis, is a complication of pregnancy in which the embryo implants outside the uterine cavity. An ectopic pregnancy is a potential medical emergency, and, if not treated properly, can lead to death.

31
Rapid Pregnancy Test is a qualitative, two-site sandwich immunoassay(6-7) for the determination of human chorionic gonadotropin (hCG) in urine, serum or/and plasma. The membrane is pre-coated with anti-alpha hCG capture antibody on the test band region and anti- species on the control band region. During testing, the specimen is allowed to react with the colored conjugate (e.g mouse anti-hCG monoclonal antibody - colloid gold conjugate) which was pre-dried on the test strip.
 which was pre-dried on the test strip..")
32
The mixture then moves upward on the membrane chromatographically by capillary action. For a positive result, a pink-colored band with the specific antibody-hCG-colored conjugate complex will form in the test band region of the membrane. Absence of this pink-colored band in the test band region suggests a negative result.

33
Regardless of the presence of hCG, as the mixture continues to move across the membrane to the immobilized goat anti-mouse, a pink-colored band at the control band region will always appear. The presence of this pink-colored band serves as 1. verification that sufficient volume is added 2. that proper flow is obtained 3. as a control for the reagents.

34
Test device, patient’s samples, and controls should be brought to room temperature (20-30°C) prior to testing. Do not open pouches until ready to perform the assay. 1. Remove the test device from its protective pouch (bring the device to room temperature before opening the pouch to avoid condensation of moisture on the membrane). Label the device with patient or control identification. 2. Draw sample to the line marked on the pipette (approximately 0.2 ml). Dispense entire contents into the sample well.
. Label the device with patient or control identification. 2. Draw sample to the line marked on the pipette (approximately 0.2 ml). Dispense entire contents into the sample well..")
35
3. Wait for pink-colored bands to appear. Depending on the concentration of hCG, positive results may be observed as soon as 40 seconds. However, to confirm negative results, the complete reaction time of 4 minutes is required. Do not interpret results after 10 minutes.

36
POSITIVE: Two distinct pink-colored bands appear, one in the patient test region (T) and one in the control region (C). NEGATIVE: Only one pink-colored band appears in the control region (C). No apparent pink band appears in the patient test region (T). INVALID: A total absence of pink-colored bands in both regions is an indication of procedural error or that test reagent deterioration has occurred.
. No apparent pink band appears in the patient test region (T). INVALID: A total absence of pink-colored bands in both regions is an indication of procedural error or that test reagent deterioration has occurred..")
37
False negative,if the test performed too early (not enough HCG). False positive,if female taken medication contains HCG.

38
Negative test results in patients suspected to be pregnant should be retested with a sample obtained 48 to 72 hours later, or by performing a quantitative assay. When testing with a urine specimen, the first morning specimen would contain the highest concentration of hCG. The shade of pink in the test band region (T) will vary depending on the concentration of hCG present. However, neither the quantitative value nor the rate of increase can be determined by a qualitative test.
 will vary depending on the concentration of hCG present. However, neither the quantitative value nor the rate of increase can be determined by a qualitative test..")
41
A procedural control is included in the test. A colored band appearing on the control region (C) is considered an internal positive procedural control, indicating proper performance and reactive reagents. A clear background in the results window is considered an internal negative procedural control. If the test has been performed correctly and reagents are working properly, the background will clear to give a discernible result.
 is considered an internal positive procedural control, indicating proper performance and reactive reagents. A clear background in the results window is considered an internal negative procedural control. If the test has been performed correctly and reagents are working properly, the background will clear to give a discernible result..")
42
1.A number of conditions other than pregnancy including trophoblastic disease and certain nontrophoblastic neoplasms cause elevated levels of hCG. These diagnoses should be considered if appropriate to the clinical evidence. 2.If a urine specimen is too dilute (i.e. low specific gravity) it may not contain representative levels of hCG. If pregnancy is still suspected, a first morning urine should be obtained from the patient 48-72 hours later and tested or test a serum sample.
 it may not contain representative levels of hCG. If pregnancy is still suspected, a first morning urine should be obtained from the patient hours later and tested or test a serum sample..")
43
3.As with all diagnostic tests, a definitive clinical diagnosis should not be based on the results of a single test, but should only be made by a physician after all clinical and laboratory findings have been evaluated. 4.Immunologically interfering substances such as those used in antibody therapy treatments may invalidate the test result.

44
The hCG hormone is measured in milli- international units per milliliter (mIU/ml). An hCG level of less than 5mIU/ml is considered negative for pregnancy, and anything above 25mIU/ml is considered positive for pregnancy. An equivocal test of between 5 and 25 mIU/cc requires a repeat within 2-3 days. If if goes higher then that's a good sign, but if it goes lower or stays about the same then that's a sign that the pregnancy has failed

45
hCG levels in weeks from LMP (gestational age) 3 weeks LMP: 5 – 50 mIU/ml 4 weeks LMP: 5 – 426 mIU/ml 5 weeks LMP: 18 – 7,340 mIU/ml 6 weeks LMP: 1,080 – 56,500 mIU/ml 7 – 8 weeks LMP: 7, 650 – 229,000 mIU/ml 9 – 12 weeks LMP: 25,700 – 288,000 mIU/ml 13 – 16 weeks LMP: 13,300 – 254,000 mIU/ml 17 – 24 weeks LMP: 4,060 – 165,400 mIU/ml 25 – 40 weeks LMP: 3,640 – 117,000 mIU/ml Non-pregnant females: <5.0 mIU/ml Postmenopausal females: <9.5 mIU/ml
 3 weeks LMP: 5 – 50 mIU/ml 4 weeks LMP: 5 – 426 mIU/ml 5 weeks LMP: 18 – 7,340 mIU/ml 6 weeks LMP: 1,080 – 56,500 mIU/ml 7 – 8 weeks LMP: 7, 650 – 229,000 mIU/ml 9 – 12 weeks LMP: 25,700 – 288,000 mIU/ml 13 – 16 weeks LMP: 13,300 – 254,000 mIU/ml 17 – 24 weeks LMP: 4,060 – 165,400 mIU/ml 25 – 40 weeks LMP: 3,640 – 117,000 mIU/ml Non-pregnant females: <5.0 mIU/ml Postmenopausal females: <9.5 mIU/ml")
46
Miscarrige and hCG hCG levels at the moment of miscarriage vary depending on how advanced the pregnancy was. For instance, hCG levels at six weeks, two weeks after the first missed period, range from 1,080 mI /mL to 56,500 mI/U. When hCG levels are not the ideal ones, or do not increase at the pace they should, something might be happening. If levels do not decrease after a miscarriage, the hCG- producing tissue is still present in the body. The woman’s menstrual cycle will not come back until the hormone is not produced anymore, which might complicate things. menstrual cycle

47
. The menstrual cycle should be back to normal around 4 to 6 weeks after a miscarriage. The higher the levels of hCG are, the longer it will take them to get back to the initial levels. After a miscarriage, placental tissue is removed or eliminated through a surgical curettage. Since the placenta is not producing hCG, the levels will eventually be reduced to less than 5mIU/mL, which is considered to be a negative hCG.

Similar presentations






BB Austin Community College>")
>")



 are gamma globulin proteins that are.>")







>")
 is produced during pregnancy. It is made by cells that form.>")

