Download presentation
Presentation is loading. Please wait.

1
Prof. Dr. Serdar ÖZTEZCAN Heart Diseases and Cardiac Markers

2
Heart Disease Heart disease is a common and debilitating condition that effect millions of patient each year; however obtaining an accurate and timely diagnosis remain difficult During the 20th century, heart disease become the leading cause of morbidity and mortality in developed nations Technology has had a causal role, allowing people to live longer enabling a sedentary and consumptive life style It is important to differentiate patients need further procedures, such as bypass grafting, angioplasty or thrombolytic therapy can safely be managed medically

3
Angina Pectoris Angina (acute myocardial ischemia) is chest pain due to insufficient blood supply to the heart muscle that results from coronary artery disease Angina can be described as a discomfort, heaviness, pressure, aching, burning, fullness, squeezing or painful feeling in your chest It can be mistaken for indigestion or heartburn Angina is usually felt in the chest, but may also be felt in the shoulders, arms, neck, throat, jaw or back
 is chest pain due to insufficient blood supply to the heart muscle that results from coronary artery disease Angina can be described as a discomfort, heaviness, pressure, aching, burning, fullness, squeezing or painful feeling in your chest It can be mistaken for indigestion or heartburn Angina is usually felt in the chest, but may also be felt in the shoulders, arms, neck, throat, jaw or back")
4
Angina Pectoris Atypical pain is the rule rather than the exception Up to 22% of patients with AMI describe their symptoms as sharp, stabbing in nature Atypical chest pain is more common in women than men Chest pain at rest but not during exercise does not decrease the likelihood of disease in women as it does men Patients predisposed to sensory impairment due to diabetes, advanced age, or altered mental status are especially likely to present in atypical ways Up to 1/3 of AMIs may be silent

5
Why? Because of wide spinal cord distribution of the cardiac pain fibers, the cerebral cortex often misinterprets the location and origin of the pain.Therefore, myocardial ischemia is easily confused with pain from other structures in the chest

6
Acut Coronary Syndrome The most important disease affecting the heart is coronary artery disease (CHD/CAD) which can lead to an acute blockage of coronary blood flow known as an acute coronary sendrom (ACS) ACS with frank necrosis of any amount of myocardium is known as myocardial infarction (MI) When the blockage is not complete, irrevesible muscle damage may be avoided, but the patient will experience severe angina at rest. This syndrome is known as unstable angina (UA)
.")
7
Myocardial Infarction

8
Diagnosis of ACS Patients who have symptoms of acute myocardial ischemia may or may not have an ST elevation (ECG) Most patients who have ST-segment elevation will ultimately develop a Q-wave acute myocardial infarction (1) Patients who have ischemic discomfort without an ST- segment elevation are having either unstable angina (2) or non-ST-segment elevation myocardial infarction that usually leads to a non-Q-wave myocardial infarction (3)
 Most patients who have ST-segment elevation will ultimately develop a Q-wave acute myocardial infarction (1) Patients who have ischemic discomfort without an ST- segment elevation are having either unstable angina (2) or non-ST-segment elevation myocardial infarction that usually leads to a non-Q-wave myocardial infarction (3)")
9
ECG ST elevation Q wave ST segment

10
ACS

11
Numbers (from The U.S.) 5 Million patients present annually to the Emergency Department (ED) complaining of chest pain (approx. 5 % of all annual ED visits) Acute Myocardial Infarction (AMI) and ACS are missed at a rate of 2% -5% Mortality in mistakenly discharged patients is twice that of admitted patients with similar risk 20% of malpractice dollars in emergency medicine are related to missed acute MI The conservative practice of hospital admission for the most patients with suspected ACS spends billions of dollars unnecessarily, because two-thirds of these patients turn out not to have ACS
 Acute Myocardial Infarction (AMI) and ACS are missed at a rate of 2% -5% Mortality in mistakenly discharged patients is twice that of admitted patients with similar risk 20% of malpractice dollars in emergency medicine are related to missed acute MI The conservative practice of hospital admission for the most patients with suspected ACS spends billions of dollars unnecessarily, because two-thirds of these patients turn out not to have ACS.")
12
Risk Factors for Coronary Artery Disease Male > 35 Female > 45, postmenopausal Hypercholesterolemia Hypertension Family History Diabetes Smoking Truncal Obesity Sedentary Lifestyle Response to stress aggressive, ambitious, compulsive persons have almost twice the risk for coronory disease as person who do not express these characteristics

13
Diagnosis of AMI Previously, the diagnosis of AMI estabilished by the WHO required at least two of the following criteria; History of chest pain Evolving changes on the ECG Elevation of serial cardiac markers In 2000, Joint European Society of Cardiology/American College of Cardiology (ESC/ACC) codified the role of biomarkers The quidelines recognized the reality that neither the clinical presentation (atypical symtoms) nor the ECG (the initial ECG may be negative/non-diagnostic in > 40%) had adequate sensitivity and spesifity Not: an ECG still remains the most specific diagnostic tool in evaluating the ED patient with chest pain
 codified the role of biomarkers The quidelines recognized the reality that neither the clinical presentation (atypical symtoms) nor the ECG (the initial ECG may be negative/non-diagnostic in > 40%) had adequate sensitivity and spesifity Not: an ECG still remains the most specific diagnostic tool in evaluating the ED patient with chest pain")
14
Diagnosis of AMI Guidelines: Either one of the following criteria satisfies the diagnosis for an acute, evolving or recent MI Typical rise and gradual fall (troponin) or more rapid rise and fall (CK-MB) of biochemical markers with at least one of the following; Ischemic symptoms Development of pathological Q waves on the ECG ECG changes indicative of ischemia (ST segment elevation or depression) Coronary artery intervention (e.g. Coronary angioplasty) Pathological findings of an AMI
 Pathological findings of an AMI.")
15
An Ideal Marker for Myocardial Injury Would Be Found in high concentrations in myocardium Released rapidly after the onset of pain Not be found in other tissues even in trace amounts Have a convenient diagnostic time window Reflect as much as possible the evaluation of myocardial damage The perfect cardiac marker test, with a 100% early sensitivity and 100% specificity does not exist different cardiac markers are used in varying combinations

16
Serum Cardiac Markers of the Past Aspartate Aminotransferase Activity (AST) Total CK Activity (CK) Lactate Dehydrogenase Activity (LD) LD1/LD2 Ratio
 Total CK Activity (CK) Lactate Dehydrogenase Activity (LD) LD1/LD2 Ratio")
17
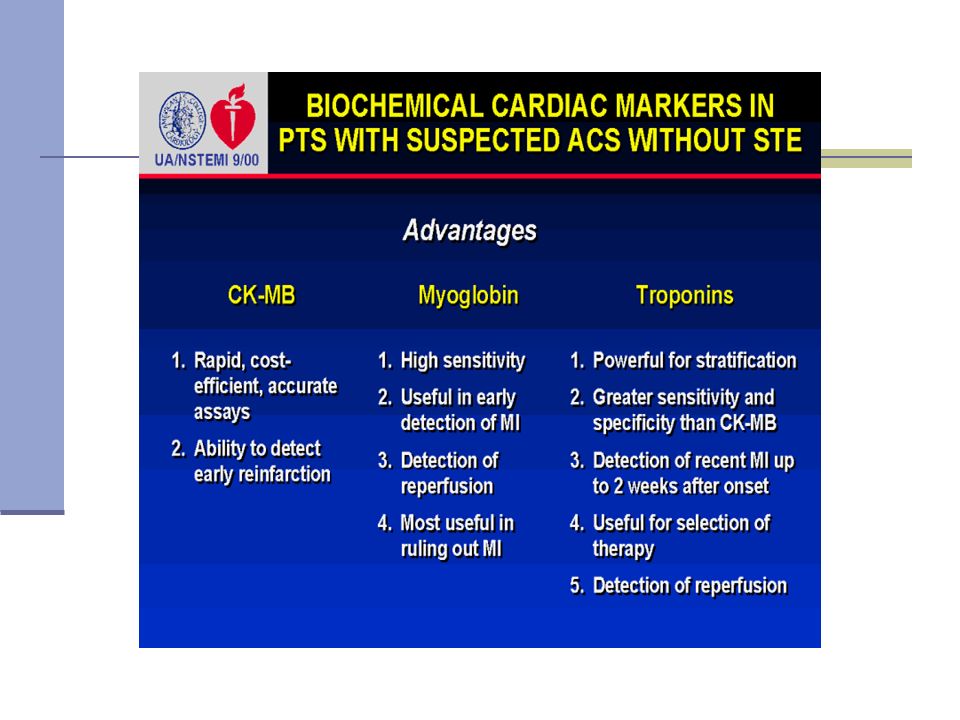
Current Cardiac Markers CK-MB Myoglobin Troponin I and T

18
Creatin Kinase Role in muscular contraction Creatine + ATP ADP + Phosphocreatine the most commonly utilized cardiac enzyme test Dimer composed of 2 monomers: M (43,000 Da) B (44,500 Da) three different iso-enzymes of CK exist CK BB CK MB CK MM
 B (44,500 Da) three different iso-enzymes of CK exist CK BB CK MB CK MM")
19
CK-MB Skeletal muscle CK-MM (99%) CK-MB (1%) Cardiac muscle 80% CK-MM 20% CK-MB Even if total plasma CK is eleveted (trauma, severe exercises), presence of more than about 5% of total as CK-MB suggests cardiac muscle damage CK-BB is found primarily in the brain and contributes very little to the serum TCK level Most of the serum CK is derived from skeletal muscle and the serum level reflects the total body muscle mass
 CK-MB (1%) Cardiac muscle 80% CK-MM 20% CK-MB Even if total plasma CK is eleveted (trauma, severe exercises), presence of more than about 5% of total as CK-MB suggests cardiac muscle damage CK-BB is found primarily in the brain and contributes very little to the serum TCK level Most of the serum CK is derived from skeletal muscle and the serum level reflects the total body muscle mass")
20
CK-MB After AMI Increase 4-6 Hours Peak 10-24 Hours Return to Normal 48-72 Hours During recent years, CK-MB activity assays have been increasingly replaced by CK-MB mass assays that measure the protein concentration of CK-MB rather than its catalyitic activity (a more rapid and more sensitive test)
")
21
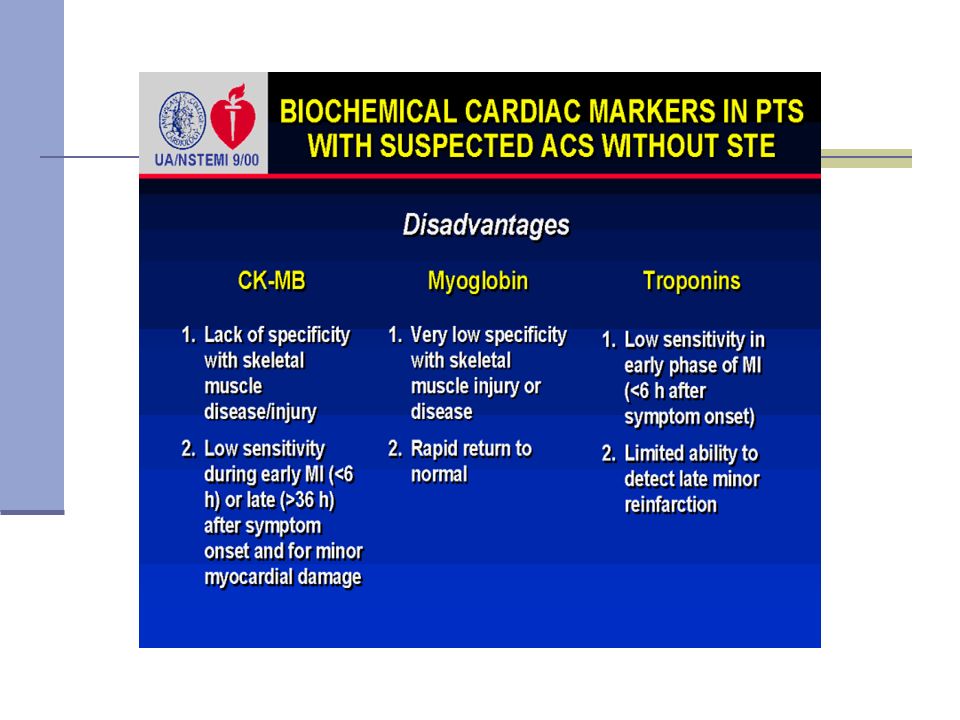
Diagnostic performance of CK-MB in AMI Sensitivity Specificity Admission 31 94 2 Hr 68 92 4 Hr 80 91 6 Hr 96 94 an elevated serum CK-MB is usually highly specific for an AMI, although rare false-positives exist (mainly from skeletal muscle release and renal failure)
")
22
Limitations of CKMB in AMI Elevated CKMB levels can be observed in: Skeletal Muscle Involvement Duchenne Muscular Dystrophy Polymyositis Alcohol Myopathy Thermal or Electrical Burn Patients Carcinomas Colon, Lung, Prostate, Endometrial

23
CK isoforms C-terminal lysine CK-MB2 (tissue) CK-MB1 (circulating) normal serum CK-MB2/CK-MB1 ratio (about 1.0) is increased in patients with an AMI (1.5 within six hours) Advantages: Early detection of AMI (1-2 hours) Methodology Limitations Labor Intensive Requires careful interpretation of CK patterns Results not available in a timely fashion Plasma carboxypeptidase
 CK-MB1 (circulating) normal serum CK-MB2/CK-MB1 ratio (about 1.0) is increased in patients with an AMI (1.5 within six hours) Advantages: Early detection of AMI (1-2 hours) Methodology Limitations Labor Intensive Requires careful interpretation of CK patterns Results not available in a timely fashion Plasma carboxypeptidase")
24
Myoglobin Definition: Oxygen-binding protein MW=17,800 kd Cytoplasmic Heart and Skeletal Muscle Tissue

25
Myoglobin The most sensitive early marker of myocardial injury (arguably) Increase 2-4 Hours Peak 5-9 Hours Return to Normal 12-24 Hours very low specificity with many false positive test results exhaustive exercise, trauma, rhabdomyolysis, surgery, shock, renal failure
 Increase 2-4 Hours Peak 5-9 Hours Return to Normal Hours very low specificity with many false positive test results exhaustive exercise, trauma, rhabdomyolysis, surgery, shock, renal failure")
26
Myoglobin Myoglobin CKMB Increase Hrs 2-4 4-6 Peak Hrs 5-9 10-24 Return to Normal 12-24 48-72

27
Myoglobin Advantages: Early Indicator of AMI Methodology – Automated Results Available in <60 Minutes Disadvantages: Not Cardiac Specific

28
Troponins Regulatory proteins in cardiac muscle that modulate the interaction between actin and myosin Troponin C (18 kd) Troponin I (26.5 kd) Troponin T (39 kd)
 Troponin I (26.5 kd) Troponin T (39 kd)")
29
Troponins

30
Tissue specificity of Troponin Subunits Troponin C is the same in all muscle tissue Troponins I and T have cardiac-specific forms cTnI and cTnT Circulating concentrations of cTnI and cTnT are very low cTnI and cTnT remain elevated for several days Troponins would seem to have better specificity than CK-MB the long-term sensitivity of LD-1

31
Troponins After AMI Troponin I TroponinT CKMB Increase Hrs 4-6 3-6 4-6 Peak Hrs 14-24 10-24 10-24 Return to Normal (Days) 5-7 6-10 2-3
")
32
Diagnostic Performance of Troponin I and Troponin T for AMI Sensitivity % Specificity % Troponin I Troponin T Troponin I Troponin T Admission 6 15 100 97 1 hr 25 38 100 96 2 hr 70 74 100 93 6 hr 96 97 99 93 12-24 hr 96 99 99 93

34
Kinetics of cardiac markers

38
Use of Biochemical Markers for Detecting Myocardial Necrosis ESC/ACC Recommendations Tn – at least 1 value > cutoff in first 24 hrs CK-MB – 2 successive samples > cutoff or 1 sample 2x cutoff CK, AST, LDH – not recommended Testing Protocol On admission, 6 – 9 hrs, and 12 – 24 hrs JACC, 2000; 36:959-69

39
ACS

40
Other markers for ACS Carbonic anhydrase III Gylcogen phosphorylase isoenzyme BB Heart fatty acid binding protein Myosin Ischemia modified albumin

41
Markers of Coronary Risk Hs-CRP Homocystein Fibrinogen D-dimer

42
Hs-CRP (High sensitive C-reactive protein) CRP is a member of the class of acute phase reactants Its levels rise dramatically during inflammatory processes occurring in the body Recent research suggests that patients with elevated basal levels of CRP are at an increased risk of diabetes, hypertension and cardiovascular disease
 CRP is a member of the class of acute phase reactants Its levels rise dramatically during inflammatory processes occurring in the body Recent research suggests that patients with elevated basal levels of CRP are at an increased risk of diabetes, hypertension and cardiovascular disease")
43
Homocystein Homocysteine is a homologue of the naturally-occurring amino acid cysteine A high level of homocysteine is a powerful risk factor for cardiovascular disease by promoting plaque formation Deficiencies of the vitamins folic acid (B9), pyridoxine (B6), or cyanocobalamin (B12) can lead to high homocysteine levels
, pyridoxine (B6), or cyanocobalamin (B12) can lead to high homocysteine levels")
44
Fibrinogen Fibrinogen is a soluble glycoprotein produced in the liver and involved in platelet agregation and coagulation It is also an acute phase protein produced in response to inflammation A relationship has been estabilished between elevated levels of fibrinogen and risk of CVD and may serve as a marker of long-term prognosis

45
D-dimer D-dimer is the end product of the ongoing process of thrombus formation and dissolution that occurs at the site of active plaques Because this process precedes myocardial cell damage and release of protein contents, it can be used for early detection Elevations of D-dimer have been shown to be useful in predicting risk for future cardiac events D-dimer lacks specifity for cardiac damage as it is increased in other conditions that cause thrombosis

46
Markers of Congestive Heart Failure B-type Natriuretic peptid (BNP) The Human Heart functions as a Pump functions as an Endocrine Organ Cardiomyocytes secrete a family of related peptide hormones, called natriuretic peptides (B-Type) Secreted by the ventricles of the heart in response to excessive stretching of heart muscle cells
 The Human Heart functions as a Pump functions as an Endocrine Organ Cardiomyocytes secrete a family of related peptide hormones, called natriuretic peptides (B-Type) Secreted by the ventricles of the heart in response to excessive stretching of heart muscle cells")
47
BNP

48
Cleavage of the 108-amino acid precursor of BNP (proBNP) produces two molecules: BNP, the active C-terminal, 77 to 108-amino acid molecule N-terminal proBNP (NT-proBNP), the inactive 1 to 76-amino acid molecule Studies indicate that NT-proBNP testing has the same clinical utility as BNP
 produces two molecules: BNP, the active C-terminal, 77 to 108-amino acid molecule N-terminal proBNP (NT-proBNP), the inactive 1 to 76-amino acid molecule Studies indicate that NT-proBNP testing has the same clinical utility as BNP")
49
BNP / NT-proBNP

50
BNP Strong negative predictive value (>98%) allows BNP and proBNP to rule out CHF Help triage possible CHF patients by determining whether symptoms such as dyspnea, edema, and fatigue are due to heart or lung disease Can detect asymptomatic left ventricular dysfunction in post-MI patients Help optimize treatment in individuals with heart failure Aid in the prognosis of existing CHF patients - BNP and proBNP levels increase proportionally with severity of disease
 allows BNP and proBNP to rule out CHF Help triage possible CHF patients by determining whether symptoms such as dyspnea, edema, and fatigue are due to heart or lung disease Can detect asymptomatic left ventricular dysfunction in post-MI patients Help optimize treatment in individuals with heart failure Aid in the prognosis of existing CHF patients - BNP and proBNP levels increase proportionally with severity of disease")
Similar presentations




 J. Teixeira, (2) P. Wotquenne, (2) V. D’Orio, (3) D. Gruson, (1)>")


 are enzymes that differ in amino acid sequence but catalyze the same.>")








>")




 Definition of ACS Signs and symptoms of ACS Gender and age related difference in ACS Pathophysiology.>")