Download presentation
Presentation is loading. Please wait.

1
Day 2

2
http://www.youtube.com/watch?v=k9e3dTOJi0o

3
Use of *Wild Card Assists in searching for creative/difficult name spellings. Reduces potential for duplication of people. Type in the first few letters of the name followed by an asterisk (*) Search Ste* to return Steven, Stephan, Stephen Search Gob* to return Goble, Gobel, Gobell Multiple wild cards may be used in the same search Search M*Doug* to return McDougal, MacDougal, MacDougall
 Search Ste* to return Steven, Stephan, Stephen Search Gob* to return Goble, Gobel, Gobell Multiple wild cards may be used in the same search Search M*Doug* to return McDougal, MacDougal, MacDougall.")
4
AKA (Also Known As) Basic person search will not provide return results if name is listed as AKA. Checking allows for complete search of names including AKA. Date Restricted Removing allows a complete review of case/provider information. Viewable when date restricted box is checked: Provider licenses - 36 months Provider notes – 36 months Legal and Planning (ISSP) - 24 months Case notes - 90 days
 - 24 months Case notes - 90 days.")
5
Person vs. Case Person Search provides information related to the person. This search locates cases or providers related to a person. Case search provides information related to the case. Use this search to: View all information contained in a specific case. View/filter case notes. Create case note or meeting without an assignment to the case. Do not use case search to review all information related to a specific person.

6
Identifying correct relationships and roles on the intake will help: Ensure vital information is quickly available in the intake. During investigation or family assessment response and ensure information printed from the system is as accurate as possible. All CPS intakes must have a subject and victim identified in the participants tab. Relationship vs. Role Relationship describes the connection between the participant and the reference person Role describes an activity or responsibility of the participant related to the intake

7
Relationship Values Establish your reference person first. Reference Person is: The person identified as the intake name. Primarily is the head of household. Each subsequent relationship value will be determined by the participant’s connection to the reference person. “Other” is an acceptable value

8
A participant must have one role and may have up to five. Alleged Perpetrator (LE Only) Identifies a person who has committed a crime. Used for a child on child action with the potential of a criminal act. Allows FamLink to populate the Law Enforcement Report accurately. Household Member A member of the family residing in the home. A grandmother living with the family. Identified Child Used on CPS-Risk Only and Non-CPS Intakes. Child in which the current concern is about or services are being requested for. More than one child may have the role of Identified Child (when applicable)
 Identifies a person who has committed a crime. Used for a child on child action with the potential of a criminal act. Allows FamLink to populate the Law Enforcement Report accurately. Household Member A member of the family residing in the home. A grandmother living with the family. Identified Child Used on CPS-Risk Only and Non-CPS Intakes. Child in which the current concern is about or services are being requested for. More than one child may have the role of Identified Child (when applicable).")
9
Intake Name Will be the reference person. Non-Household Member An active member of the family not residing in the home. A grandmother living in her own residence but active in the household activities. Parent/Parental Role Consider the Intake you are completing. Intake Name will consistently have the role of Parent/Parental role. Referrer, Witness or Collateral Role values that will not relate the participant to the case.

11
Good interviewing skills are critical to information gathering: Take notes as soon as the referrer/caller begins speaking Show respect Be empathetic Listen carefully to the referrer’s/caller’s concerns Acknowledge feelings

12
Good interviewing skills: Be professional, non judgmental Ask open-ended questions Make affirmations-genuine statements of appreciation Utilize reflective listening Summarize

13
I think, at a child’s birth, if a mother could ask a fairy godmother to endow it with the most useful gift, that gift should be curiosity. Eleanor Roosevelt

14
Referrers/Callers to CA intake may be in crisis or have escalated emotions. De-escalation techniques: Assess the situation promptly Ask clarifying questions to better understand Maintain a calm demeanor and voice Use problem solving with the referrer/caller— ask “What will help now?” Be empathetic Reassure referrer/caller

15
Avoid an argumentative tone. Engage the referrer/caller by asking open-ended questions. Give the referrer/caller time to think. Ignore challenges; redirect challenging questions. Allow venting, but maintain focus of call. Avoid power struggles. Be clear; use simple language. Use reflective technique -- "Am I hearing you?" Summarize concerns reported. Tell referrer/caller what you can do.

16
Caller’s name and phone number. Relationship to the family or child For CA/N referrals explain: CA does not reveal the referrer’s name during the investigation, HOWEVER, Family may guess, referrer often confirms CA may disclose if court involvement, criminal investigation or by court order Good Faith and immunity (RCW 26.44.060) False reporting, if appropriate (RCW 26.44.061) If call made on behalf of medical professional, document name of professional
 False reporting, if appropriate (RCW ) If call made on behalf of medical professional, document name of professional.")
17
Screen in when there is:: A serious threat of substantial harm to a child. Conduct involving a criminal offense that has occurred, or is about to occur, in which the child is the victim. A founded CA/N report on a household member within the past three years. The allegations include bruises on a child less than a year old. Intake uses their best judgment to determine if there is a threat of substantial harm to the child. If the four factors above do not exist, the intake is screened out.

18
What made the referrer/caller call today? Start gathering demographic information: Household composition Caregiver, Primary caregiver Child or children Current addresses, any information referrer/caller knows to locate the child and family Race, ethnicity, cultural considerations Native American Heritage Primary Language Document what the referrer/caller doesn’t know Ask follow up questions, ask referrer/caller to clarify and define terms used.

19
What is the nature and extent of the maltreatment? What surrounding circumstances accompany the maltreatment? How does the child or children function on a daily basis? What are the overall parenting/child practices used by the caregiver? How does the parent/caregiver manage his/her own life on a daily basis? How does the parent (s)/caregiver discipline the child?
/caregiver discipline the child .")
23
Make sure referrer/caller has your full name before the call is terminated. Summarize the referrer/caller’s concerns. Ask if there is any information that was missed or additional concerns. Let the referrer/caller know: The information is appreciated. Whether the information will likely be screened in or not. The potential outcomes, documentation requirements and that the report will be sent to law enforcement if appropriate. To call back with any additional concerns.

24
Search history in FamLink Summarize history under “additional risk factors”. Note if there is an open case on the family or victim. Note fact patterns, frequency, detail as needed to illustrate information: Any recent case assignment, investigations and closing summaries All prior intakes History of the maltreatment Prior cases assignment Prior dependency Prior placement, legal history Prior engagement in services Findings history including unfounded

25
Intake staff should contact collateral information sources & record each contact when: It is necessary to clarify or verify an allegation of child abuse or neglect, or Information is not available from the referrer to determine the intake screening decision or appropriate response (e.g., alternate intervention or investigation). Information indicates the child or any relative may be Native American, Alaska Native or Canadian First Nations and a WA State Tribe is indicated.

26
Collateral contacts are made as soon as possible prior to making screening decisions unless: An emergent response is required, It compromises the impending investigation, Puts the referrer at risk of harm, or Sufficient information was gathered by the original referrer to determine a screening decision.

27
Child Abuse Consultation Network for Washington State Child Protection Medical Consultants: Interpret written reports, radiological findings, and other materials submitted by CA social workers, law enforcement officers, prosecuting attorneys, and other physicians requesting consultation regarding evidence of abuse or neglect. Provide telephone consultation to CA social workers on cases of suspected child abuse or neglect. Upon request of CA, coordinate and facilitate child protection training events with local health experts at locations throughout the state.

28
Use clear, simple and common language. Spell out or define acronyms. Keep sentences and paragraphs short. Use term referrer or caller in body of document to identify the reporter Limit use of pronouns. Spell out acronyms before subsequent use. Quote caller when necessary, e.g. “Swear words”. Be behavior specific and concrete.

29
Clarify with caller what words mean to them. For example, the house was filthy. What does filthy mean to you? Can you describe what you saw? Written word should reflect the story the caller is telling in a logical way that can be understood by others. How do you ensure that the information in the Intake accurately reflects what the caller is saying? Summarize, for the caller, what they have told you. Ask if you have captured their concerns.

31
Does the intake contain a clear summary of the nature of the concern for the child? Safety threats? Child’s vulnerability? Are the risk factors for the children clearly and specifically documented, including information known in the record? Are the risk factors for the caregivers clearly and specifically documented, including information known in the record? Does the intake clearly indicate if there is an open case? Does the intake clearly state the household composition? Does the intake have a summary of prior history including prior intakes, outcome of investigations, out of home placements, dependency actions, etc.? Or clearly state there is no prior history? Does the intake state what the referrer/caller does not know?

33
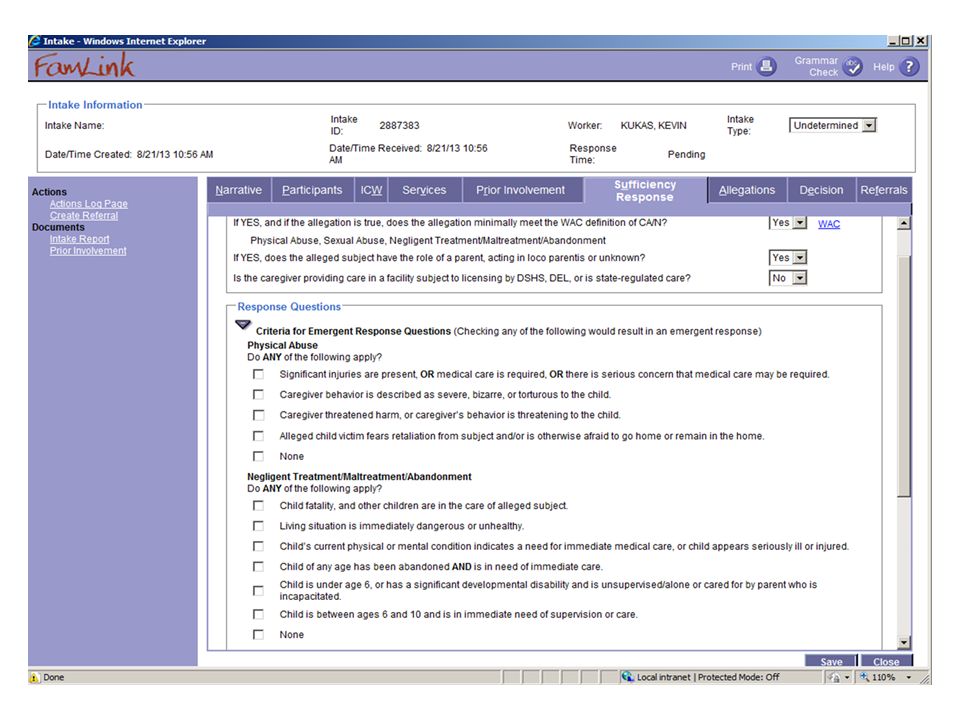
◦ Is the victim under 18 years of age? ◦ The allegation, if true, minimally meets the WAC/RCW definition of CA/N? ◦ Is the alleged subject a parent/guardian of the alleged victim, acting in loco parentis or unknown? ◦ Or is the alleged subject providing care in a facility subject to licensing by DSHS, DEL or state- regulated care?

35
If the allegation were true, does the allegation minimally meet the WAC definition of CA/N? Physical abuse is characterized by physical injury of an intentional, non-accidental nature. Not all physical injuries are visible. Sexual abuse Neglect is characterized by failure to provide the supervision and care necessary for a child’s safety, development or health. Neglect may result in impending danger to a child or can have cumulative effect on the child’s safety, development and health. This includes medical neglect. Failure by the parent to obtain professional help for a child with mental health issues or life- threatening medical conditions would be considered neglect.

36
Emotional neglect or abuse is not specifically defined in RCW or CA policy. However, emotional neglect or abuse may be occurring along with other forms of CA/N. Emotional neglect or abuse will generally be included as a form of negligent treatment or maltreatment. Abandonment of a child by the parent is characterized by the lack of parental intention to return to the parenting role.

39
Physical Abuse ◦ Significant injuries are present, or medical care is required, or there is serious concern that medical care may be required ◦ Caregiver behavior is described as severe, bizarre or tortuous to the child ◦ Caregiver threatened harm, or caregiver’s behavior is threatening to the child ◦ Alleged child victim fears retaliation from perpetrator and/or is otherwise afraid to go home or remain in the home.

40
Negligent Treatment ◦ Child Fatality and other children are in the care of alleged subject ◦ Living situation is immediately dangerous or unhealthy. ◦ Child’s current physical or mental condition indicates a need for immediate medical care or child appears seriously ill or injured. ◦ Child is under 6, or has a significant developmental disability and is unsupervised/alone or cared for by parent who is incapacitated. ◦ Child is between ages 6 and 10 and is in immediate need of supervision or care.

41
Sexual abuse/exploitation ◦ Is the non-perpetrating caregiver aware of the alleged abuse and is demonstrating a response that is appropriate and protective of the child? ◦ Allegation involves a licensed home or facility, and children remain in their care. ◦ Alleged perpetrator will have access to alleged child victim within the next 72 hours, or access within the next 72 hours is unknown. ◦ Alleged physical injury to the child victim occurred due to alleged sexual abuse/exploitation. ◦ Allegations are against the out-of-home, unlicensed caregiver, and children remain in their care.

43
Physical Abuse ◦ Alleged victim is in out of home care AND allegations are against the out of home, unlicensed caregiver ◦ Allegation involves a licensed home or facility ◦ Alleged victim is the victim or alleged subject is the subject in three or more investigations or assessments in the past year. ◦ Allegation includes reports of bruises on non- mobile children. ◦ Report made by a physician, or a medical professional on a physician’s behalf, regarding a child under age five (5)
.")
44
Negligent Treatment ◦ Alleged victim is in out-of-home care AND allegations are against the out-of-home, unlicensed caregiver. ◦ Allegation involves a licensed home or facility. ◦ Alleged victim is the victim of alleged subject is the subject in three or more investigations or assessments in the past year.

45
If sufficiency screening criteria are not met, the Additional Screening Criteria/Risk Only box is expanded.

47
Intake workers have the ability to override the screening decision. Intake supervisors make the final screening decision.

49
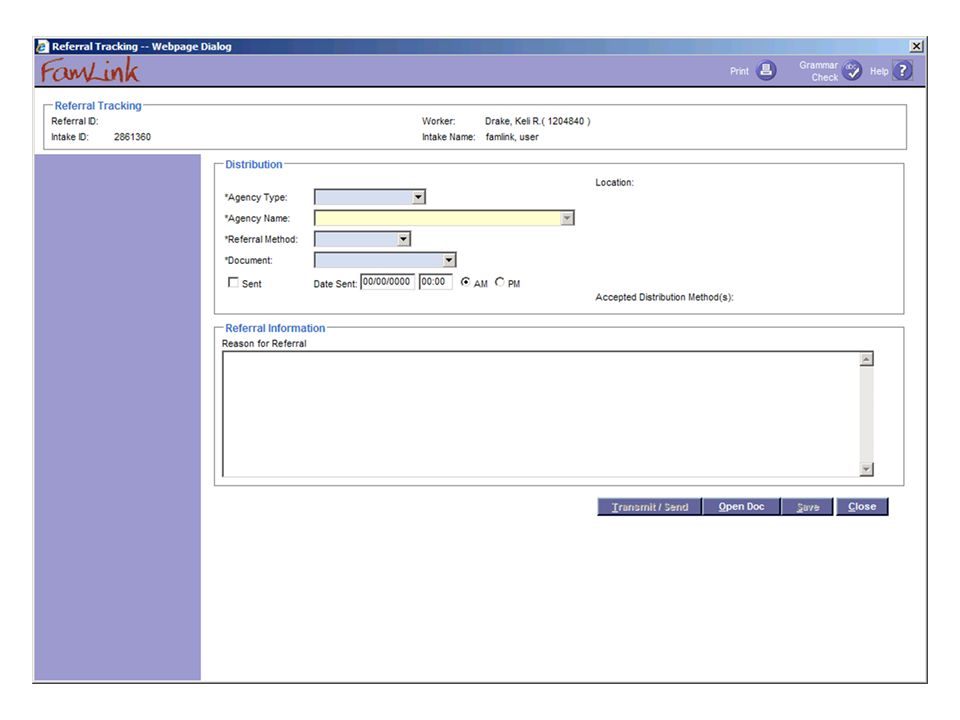
There is a law enforcement referral tab in the intake. ◦ Can be launched at any time, including by CPS. ◦ Provides a way to document when, to whom and how the intake was sent to law enforcement. ◦ Can be sent to multiple law enforcement agencies

52
INTAKE TYPETIMELINE FOR INTAKE COMPLETION AGENCY RESPONSE TIMELINE CPS INTAKES CPS or DLR/CPS Emergent Within 4 hours of receipt24 hours CPS Investigation, CPS FAR or DLR/CPS Non-Emergent Within 4 business hours of receipt 72 hours CPS or DLR/CPS Risk OnlyWithin 4 hours of receipt24 hours or 72 hours

53
INTAKE TYPETIMELINE FOR INTAKE COMPLETION AGENCY RESPONSE TIMELINE NON CPS INTAKES FRSWITHIN 4 HOURS OF RECEIPT 24 HOURS CFWS AND FVSWITHIN 2 BUSINESS DAYS OF RECEIPT 24 HOURS OR 72 HOURS RULE INFRACTIONWITHIN 2 BUSINESS DAYS OF RECEIPT 72 HOURS TRIBAL PLACEMENT/PAYMENT ONLY WITHIN 2 BUSINESS DAYS OF RECEIPT N/A PRIVATE ADOPTION- ADOPTION SUPPORT WITHIN 2 BUSINESS DAYS OF RECEIPT N/A ADOPTION/ICPC/ICAMAN/A

54
Child Pornography. Research indicates child pornography offenders (meaning a charge and conviction) who have also committed a contact sexual offense are “most likely to re-offend, either generally or sexually”. There have been no research findings on whether child pornography possession is a valid indicator of pedophilia in the general population. Allegations of child pornography possession in the home should be screened at a minimum, as risk only, when there are no other CA/N allegations. Exceptions to screen-in include scenarios in which law enforcement has investigated, there is a protective parent, the perpetrator has been arrested and the children interviewed. Possession of child pornography is a crime and requires law enforcement referral.
 who have also committed a contact sexual offense are most likely to re-offend, either generally or sexually . There have been no research findings on whether child pornography possession is a valid indicator of pedophilia in the general population. Allegations of child pornography possession in the home should be screened at a minimum, as risk only, when there are no other CA/N allegations. Exceptions to screen-in include scenarios in which law enforcement has investigated, there is a protective parent, the perpetrator has been arrested and the children interviewed. Possession of child pornography is a crime and requires law enforcement referral..")
55
Universal Screening Question To assess whether a child is in clear and present danger from DV, intake (and all CA staff working with the family) should first identify the presence of DV. Ask: “Has any adult used or threatened to use physical force against an adult in the home?” If the referrer says “yes”, ask the caller, “Who did what to whom?”

56
Determining Risk of Imminent Harm When the answer to the universal screening question is “yes”, consider risk factors to determine whether the DV causes harm or creates a risk of imminent harm to a child. The following questions can help determine risk of imminent harm when DV is present.

57
Questions to Assist with determining Risk of Imminent Harm when DV is Present Was the child assaulted, injured, or threatened during the domestic violence incident? Was the child in danger of physical harm during the domestic violence incident(s), e.g., was the child being held when the domestic violence perpetrator attacked, or did the child attempt to intervene in the domestic violence? Was the child’s parent or caretaker incapacitated or killed by the DV perpetrator so the parent or caregiver is unable to meet the child’s needs?
, e.g., was the child being held when the domestic violence perpetrator attacked, or did the child attempt to intervene in the domestic violence. Was the child’s parent or caretaker incapacitated or killed by the DV perpetrator so the parent or caregiver is unable to meet the child’s needs .")
58
Intake staff must give the following risk factors exceptional consideration when present: DV perpetrator’s suicidal threats or attempts. DV perpetrator’s threats or attempts to kill or injure the adult victim and/or the child or others. DV perpetrator’s active substance abuse. DV perpetrator displays, threatens to use, or uses a firearm or other lethal weapon. DV perpetrator displays evidence of untreated psychosis or mental health disorder.

59
DV perpetrator is obsessive and controlling towards the partner and/or children, such as constant surveillance of the victim by the perpetrator, repeated harassing, telephone calls to the victim, or as evidenced by a civil protection order or criminal conviction on stalking charges, etc. DV is increasing in either frequency or severity. DV perpetrator denies adults and children access to basic needs. Children are exhibiting observable effects of the DV, causing substantial impairment.

60
Notify in-state tribes and law enforcement when intake is completed Send an email regarding CPS intakes related to non DLR/DEL contracted providers to the regional contracts coordinator. Any crimes against a child must be forwarded to law enforcement Generate a new intake on an open case when a report is received alleging a new incident of abuse or neglect has occurred.

61
Generate a new intake if a second report about an incident of abuse or neglect already documented in an intake is received. The intake worker will “Screen Out” this intake with a reason code of “Allegation documented in previous intake.” Intake worker will provide the previous intake # in the explanation dialogue box in the Decision Tab in FAMLINK. The supervisor confirms all allegations have previously been documented.

62
Create separate intakes for the same incident of CA/N involving more than one family residing in the same household. Avoid cutting and pasting. Make sure each intake reflects the correct reference person, alleged victims, subjects and allegations. Make sure CPS and CPS Risk only intakes are not linked to Adoption Support or ICAMA cases in FAMLINK.

63
http://www.bing.com/videos/search?q=telephone+comedy+filte rui%3aduration-short+filterui%3aduration- short&view=detail&mid=56C57B2FBA000CDD743256C57B2FBA0 00CDD7432&first=81&qft=+filterui%3aduration-short

Similar presentations






















: OCONUS 484-530-5908 www.myarmyonesource.com.>")



>")



 Version 1.0 | 2014.>")
