Download presentation
Presentation is loading. Please wait.

1
Stomach & duodenum

7
Barium meal Fluoroscopy + spot films Preparation

8
The Normal Anatomy of Stomach 1- Shape. 2-Size. 3-Site
The Normal Anatomy of Stomach 1- Shape. 2-Size. 3-Site. 4-Anatomical parts. 5-Mucosal pattern.

10
Normal Anatomy of Duodenum Duodenal cap. Duodenal loop

11
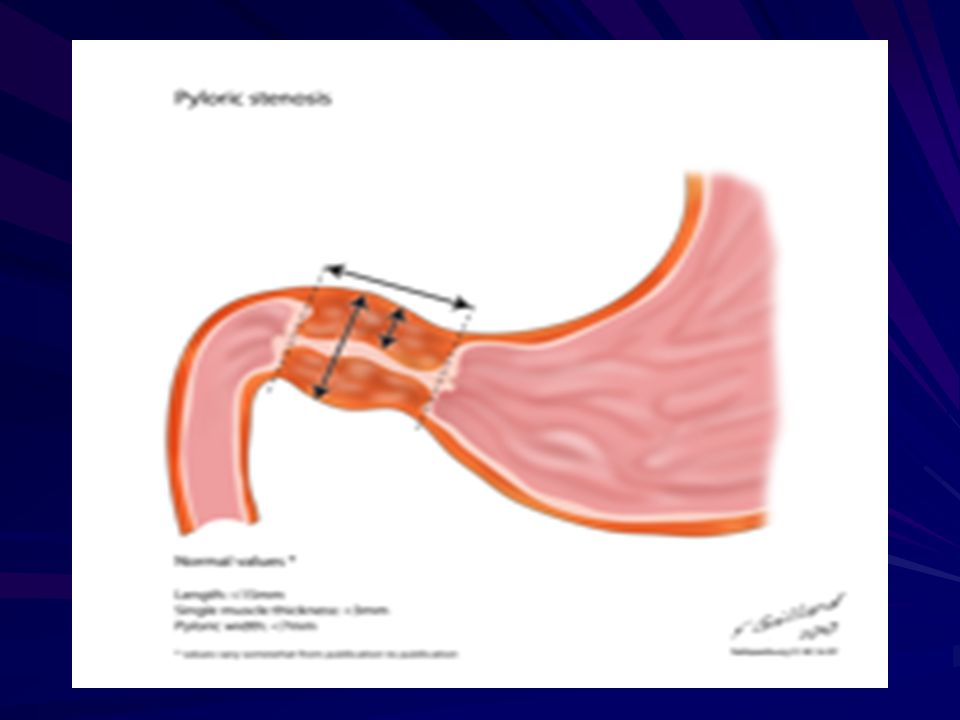
Hypertrophic pyloric stenosis Cause: A. Congenital type B. Adult type

12
Epidemiology Pyloric stenosis is relatively common and has a male predilection (M:F ~ 4:1), and is more commonly seen in Caucasians 4. It typically occurs between the 4-8 weeks of life. There may be a positive family history. Incidence of hypertrophic pyloric stenosis is approximately 2-5 per 1,000 births per year in most white populations, Hypertrophic pyloric stenosis refers to idiopathic thickening of gastric pyloric musculature which then results in progressive gastric outlet obstruction
, and is more commonly seen in Caucasians 4. It typically occurs between the 4-8 weeks of life. There may be a positive family history. Incidence of hypertrophic pyloric stenosis is approximately 2-5 per 1,000 births per year in most white populations, Hypertrophic pyloric stenosis refers to idiopathic thickening of gastric pyloric musculature which then results in progressive gastric outlet obstruction.")
14
In a normal situation, the pyloric muscle thickness (diameter of a single muscular wall on a transverse image) should normally be less than 3 mm (most accurate 3) and the length (longitudinal measurement) should not exceed 15 mm.
 should normally be less than 3 mm (most accurate 3) and the length (longitudinal measurement) should not exceed 15 mm.")
16
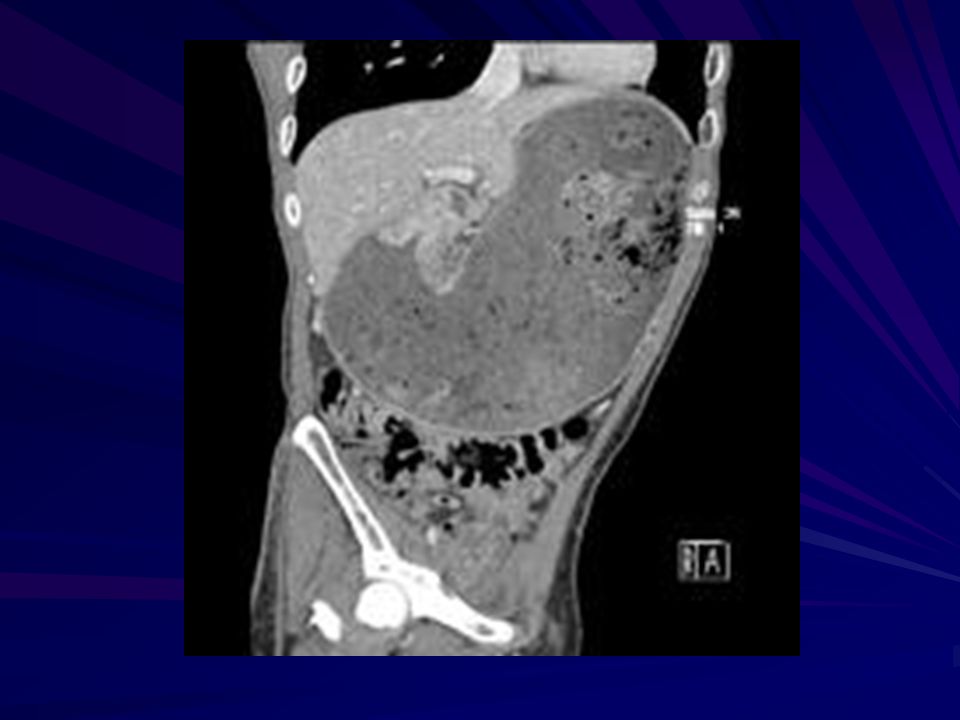
Gastric outlet obstruction (often abbreviated as GOO) is a medical condition where there is an obstruction at the level of the pylorus, which is the outlet of the stomach. Individuals with gastric outlet obstruction will often have recurrent vomiting of food that has accumulated in the stomach, but which cannot pass into the small intestine due to the obstruction. The stomach often dilates to accommodate food intake and secretions. Causes of gastric outlet obstruction include both benign causes (such as peptic ulcer disease affecting the area around the pylorus), as well as malignant causes, such as gastric cancer
, as well as malignant causes, such as gastric cancer.")
17
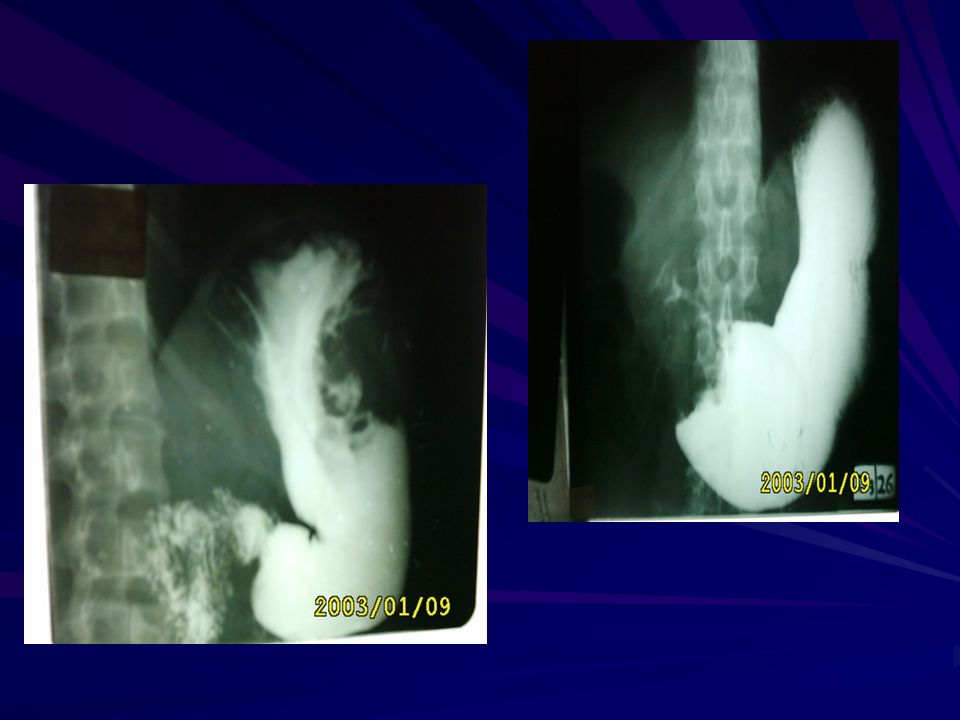
Radiographic Ba meal examination of the Pyloric
stenosis 1. Marked dilatation of the stomach attends the pelvic cavity 2.Failure of passage of contrast into the duodenum. 3.Multiple filing defects are seen within the stomach due to retained food material .

18
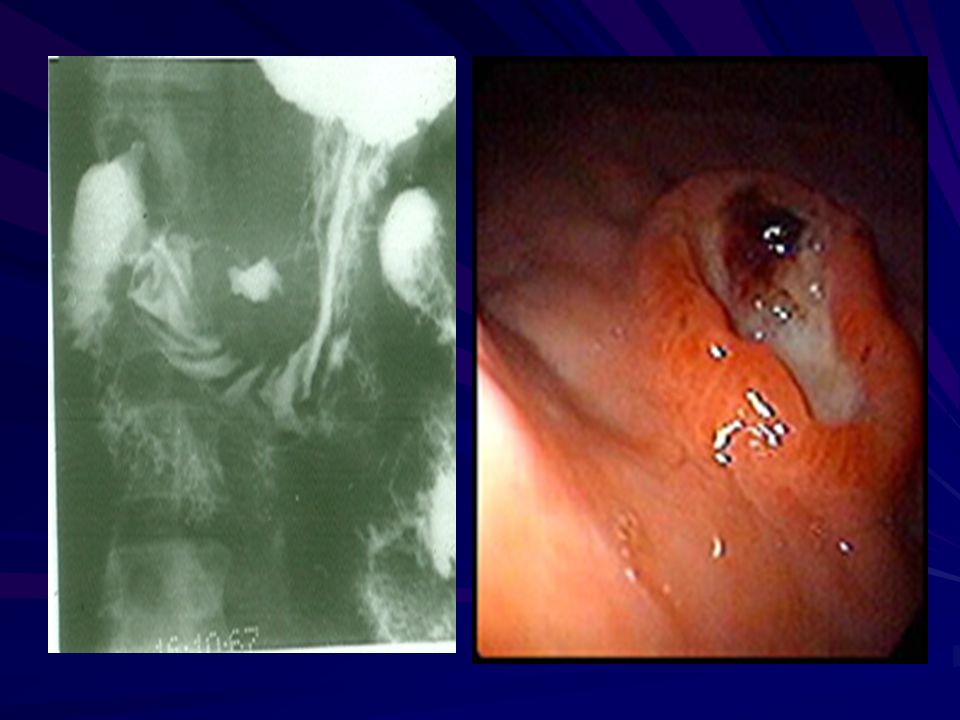
Barium meal image of a case of corrosive-induced gastric outlet obstruction benign narrowing
GASTRIC CA

20
PEPTIC ULCER GU, DU and IU. The Ba
PEPTIC ULCER GU, DU and IU. The Ba. meal findings are : 1-Direct signs : * Ulcer crater ( nitch): Either in enface or in profile * Associated signs: I. Spasm II. Radiated mucosal folds. III. Edema (Hampton's line). 2- Indirect signs : I. Hyper peristaltic waves II. Companion B sign III. Thick mucosal folds & hyper peristaltic stomach (angry mucosa)
: Either in enface or in profile * Associated signs: I. Spasm II. Radiated mucosal folds. III. Edema (Hampton s line). 2- Indirect signs : I. Hyper peristaltic waves. II. Companion B sign. III. Thick mucosal folds & hyper peristaltic stomach (angry mucosa)")
21
Radiographic Signs of a benign gastric ulcer
Ulcer crater-collection of barium on dependent surface which usually projects beyond anticipated wall of stomach in profile (penetration) Hampton’s line-1 mm thin straight line at neck of ulcer in profile view which represents the thin rim of undermined gastric mucosa
 Hampton’s line-1 mm thin straight line at neck of ulcer in profile view which represents the thin rim of undermined gastric mucosa.")
22
lesser curvature gastric ulcer
lesser curvature gastric ulcer. Red arrows point to Hampton's Line, a thin, straight line at neck of ulcer in profile view which represents the thin rim of undermined gastric mucosa. The blue arrows point to the ulcer mound, a smooth, sharply delineated soft-tissue mass surrounding a benign ulcer. Note how the ulcer projects beyond the confines of the expected wall of the stomach.

25
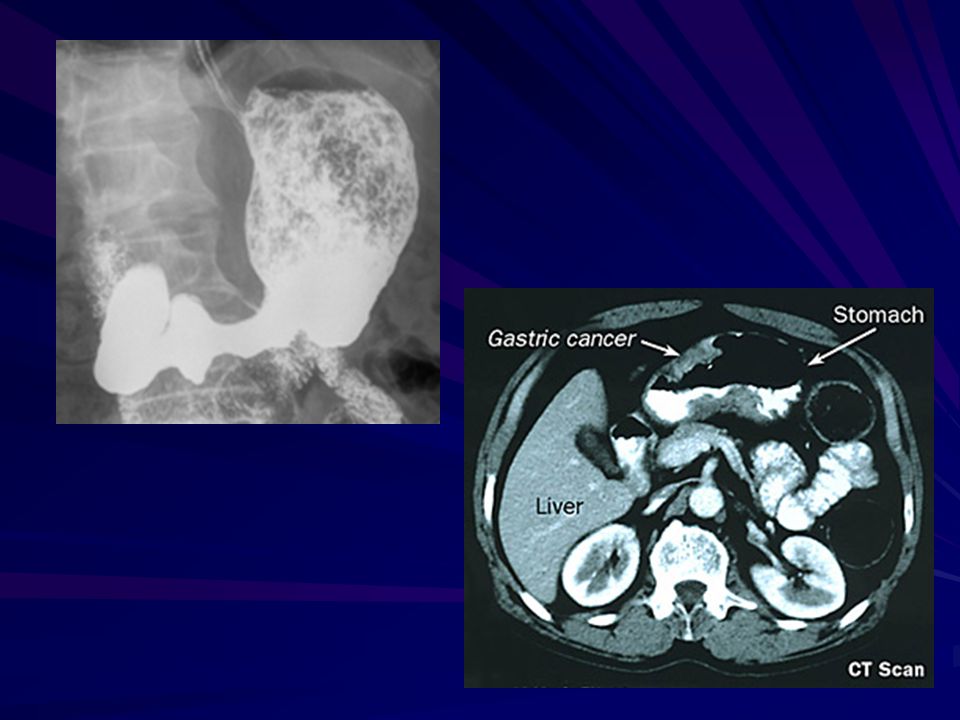
Gastric carcinoma refers to a primary malignancy arising
from the gastric epithelium. 3 presentation Polypoidal Infiltrative * localized * generalized Ulcertaive type barium meal presentation of the CA stomach 1.Carcinoma produce single or multiple irregular filling defect with alteration of near by mucosal Pattern . 2.Localized or generalized narrowing of the stomach rigid in appearance with shoulding sign on either sided aspect of the narrowing .

26
3- Ulcerative Ca Either : I. Polypoidal tumour with ulceration or II
3- Ulcerative Ca Either : I.Polypoidal tumour with ulceration or II. Complicated benign gastric ulcer on Ba. Meal : * Filling defect with central ulcer crater * No mucosal radiation , due to destruction . * The ulcer crater is not projected out side the lumen ( meniscus sign ) * Hour glass deformity ( X ) of stomach
 * Hour glass deformity ( X ) of stomach.")
30
Duodenal ulcers (DUs) affect nearly 10% of the adult population at some time,[1]and these lesions account for two thirds of all peptic ulcers, which are defined as mucosal breaks of 3 mm or greater; gastric ulcer accounts for the rest Most duodenal ulcers are depicted as round or ovoid pools of barium; about 5% may be linear, and most are smaller than 1 cm in diameter. Giant duodenal ulcers, defined as those >2 cm in diameter, have an increased risk of perforation, obstruction, and bleeding. Multiple ulcers occur in about 15% of patients[1] ;Zollinger-Ellison syndrome should be considered in these patients. About 95% of duodenal ulcers occur in the duodenal bulb,[1] and the rest occur in the post bulbar duodenum, bulber U which consists of the proximal 2 cm of the descending duodenum above the ampulla of Vater. As many as half of all duodenal ulcers occur in the anterior wall of the bulb.

32
Complicated Chronic DU 1-Tri foil deformity ( tri foil tree ) 2-Pseudo diverticulum (Akerland diverticulum) 3-Gastric outlet obstruction.( pyloric obstruction ).
 2-Pseudo diverticulum (Akerland diverticulum) 3-Gastric outlet obstruction.( pyloric obstruction ).")
33
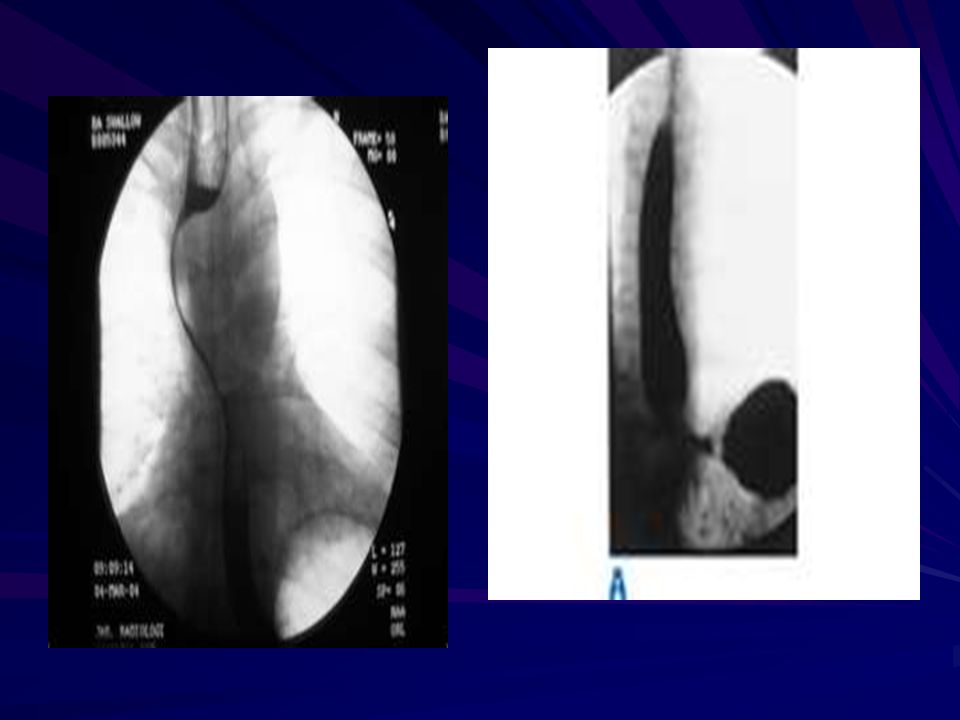
During Ba examination � Bird's Beak deformity of lower oesophagus - Achalsia cardia (Barium Swallow) � Cork screw oesophagus-- Diffuse oesophageal spasm (Barium Swallow) � Commonest radiological appearance of gastric � Trifoliate duodenum - Chronic duodenal ulcer with scarring (Barium Meal) � Hour Glass stomach - Peptic ulcer � Single-bubble appearance - pyloric stenosis � Double-bubble sign--Duodenal atresia, duodenal stenosis, � Triple-bubble sign - Jejunal atresia � Coiled spring appearance -Intussusception
 � Cork screw oesophagus-- Diffuse oesophageal spasm (Barium Swallow) � Commonest radiological appearance of gastric � Trifoliate duodenum - Chronic duodenal ulcer with scarring (Barium Meal) � Hour Glass stomach - Peptic ulcer � Single-bubble appearance - pyloric stenosis � Double-bubble sign--Duodenal atresia, duodenal stenosis, � Triple-bubble sign - Jejunal atresia � Coiled spring appearance -Intussusception.")
34
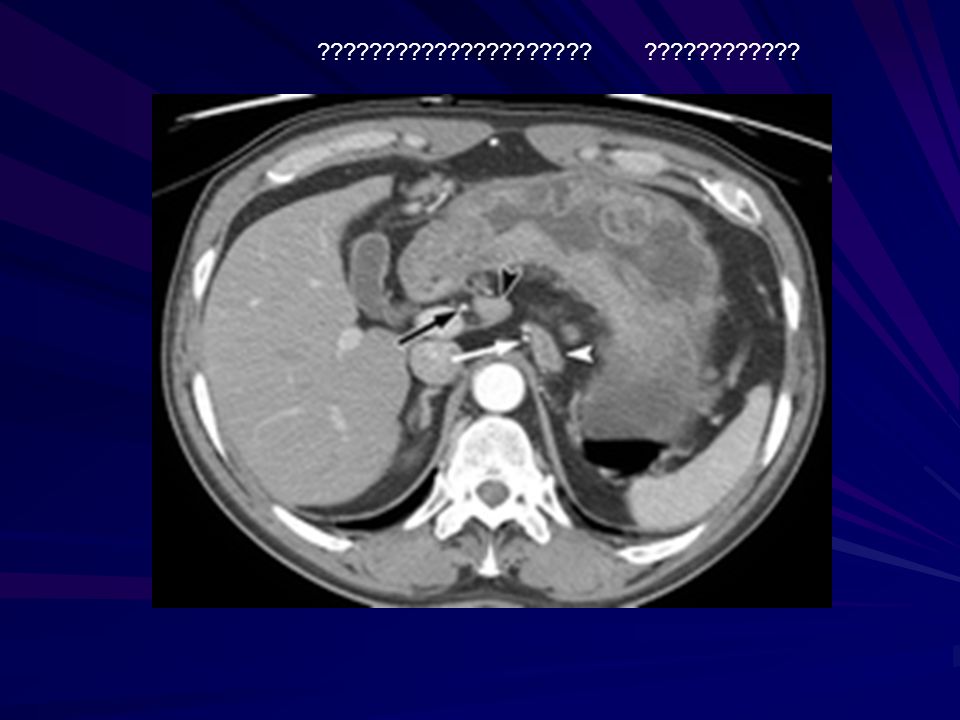
????????????????????? ????????????
Similar presentations











 is usually characteristic of: A.Hypertrophic pyloric stenosis.>")




>")
![Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.](/13/3809458/big_thumb.jpg "Peptic Ulcer Disease Dr Maha Arafah. Objectives Upon completion of this lecture the students will : A] Understand the Pathophysiology of acute and chronic.>")



>")
 Dr. Gehan Mohamed Dr. Abdelaty Shawky.>")




