Download presentation
Presentation is loading. Please wait.

1
Carbapenemases in practice - lessons learnt from spread in our patch, prophylaxis and first/second line treatments Dr Andrew Dodgson Consultant Microbiologist and Infection Control Doctor Health Protection Agency & Central Manchester University Hospitals NHS Foundation Trust

2
Carbapenemases Phenotypically similar enzymes Genotypically diverse Epidemiologically Diverse

3
Classification Class A (serine based) KPC, GES, SME, NMC, IMI Class B (metallo-enzymes) NDM, IMP, VIM, GIM, SIM, SMP, L1, BCII, Ccra Class D (serine) OXA From Queenan and Bush, CMR 2007
 KPC, GES, SME, NMC, IMI Class B (metallo-enzymes) NDM, IMP, VIM, GIM, SIM, SMP, L1, BCII, Ccra Class D (serine) OXA From Queenan and Bush, CMR 2007")
4
Classification Chromosomal – Class A SME, NMC, IMI – Class B BCII, L1, Ccra Plasmid – Class A KPC, GES – Class B NDM, IMP – Class D OXA From Queenan and Bush, CMR 2007

5
“Transmission” of Resistance Clonal spread (particularly ST258 K. pneumo for KPC) Transmission of plasmid Other enterobacteriaceae implicated, e.g. Enterobacter, E.coli
 Transmission of plasmid Other enterobacteriaceae implicated, e.g. Enterobacter, E.coli.")
6
Therapy Need to know local epidemiology i.e. clonal spread – all isolates have the same antibiogram or polyclonal, transmission of plasmid – sensitivities vary depending on the background of the strain carrying the plasmid

7
Local situation? Many different strains Same plasmid Enterobacter E. coli KPC producer from a nearby hospital Courtesy N. Woodford

8
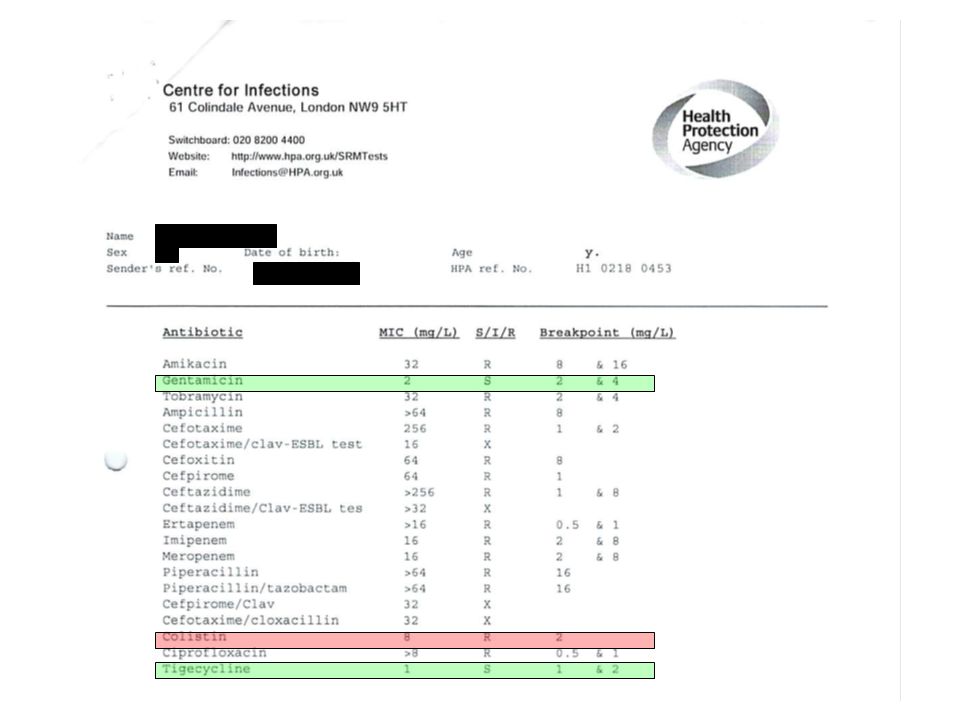
Carbapenems? Some carbapenemase producers will have MIC’s below the breakpoint for resistance Carmeli et al. CMI 2010

9
SIR Erta≤0.51>1 0.5->64 Imi≤24-8>8 0.5->64 Mero≤24-8>8 1-64 Miriagou et al. CMI 2010.

10
Carbapenems? Some carbapenemase producers will have MIC’s below the breakpoint for resistance Carbapenems show some activity in animal models against these strains Strong inoculum effect noted in in-vitro models MIC ≤8 Mortality 29%, MIC>8 75% Carmeli et al. CMI 2010; Daikos et al, AAC 2009

11
Other options Again, depends on susceptibility results. Many strains multi (or almost pan-) resistant
 resistant.")
13
Other options – Quinolones – Aminoglycosides – Tigecycline – Colistin – Trimethoprim – Fosfomycin – Temocillin – Combinations (which ones?)
")
14
What should we do? Review of 298 published cases (244 BSI) Tzouvelekis et al, CMR 2011 TreatmentFailure rate 2 drugs, inc carbapenem (MIC<8)8% 2 drugs, no carbapenem29% Aminoglycoside alone24% Carbapenem alone(MIC<8)25% Tigecycline alone36% Colistin alone47% Inappropriate Rx54%
 Tzouvelekis et al, CMR 2011 TreatmentFailure rate 2 drugs, inc carbapenem (MIC<8)8% 2 drugs, no carbapenem29% Aminoglycoside alone24% Carbapenem alone(MIC<8)25% Tigecycline alone36% Colistin alone47% Inappropriate Rx54%.")
15
Sensitivities Data from 30 Blood cultures Sensitive (%)Intermediate( %)Resistant (%) Colistin 928 Amikacin 771013 Tigecycline 7413 Gentamicin 58339 Temocillin 5743 Ciprofloxacin 5248 Trimethoprim 4852 Meropenem 31087
Intermediate( %)Resistant (%) Colistin 928 Amikacin Tigecycline 7413 Gentamicin Temocillin 5743 Ciprofloxacin 5248 Trimethoprim 4852 Meropenem 31087")
16
What do we do? Plasmid mediated resistance Necessitates individual patient approach Usually based on sensitivities of previous screening or clinical isolates Some broad principles: – 2 agents – B-lactam (if poss) – Aminoglycoside if possible – Colistin never alone
 – Aminoglycoside if possible – Colistin never alone.")
17
Prophylaxis Difficult to generalise due to variable susceptibilities – GI Surgery Tigecycline – Urology Aminoglycoside or Cipro

18
Empiric Rx Paeds neutropenic sepsis: – Pip/Taz and Amikacin 1 st line – Close scrutiny of sens of all BC’s – And sens of CPC screening isolates – No Amik resistance (yet)
")
19
Empiric Rx GNR in blood culture, pt known to be colonised Depends on sens and site of primary infection Toxicity often less of a concern (due to lack of options) Almost always add suitable aminoglycoside Tige/Colistin not used alone
 Almost always add suitable aminoglycoside Tige/Colistin not used alone")
20
Empiric Rx What have we done? – 30 bacteraemic adult pt’s – 18 different regimes used – 11 received monotherapy (cip 4, gent 4, tige, col, mero) – 15 had 2 Abx, 1 had 3 and 1 4. – 16 of 19 with 2 or more abx had an aminoglycoside
 – 15 had 2 Abx, 1 had 3 and 1 4. – 16 of 19 with 2 or more abx had an aminoglycoside.")
21
Summary Carbapenemase producing enterobacteriaceae are heterogenous Know your local epidemiology Take MIC’s into account (esp. Carb’s) Be prepared to think laterally
 Be prepared to think laterally.")
22
Acknowledgements Dr Louise Sweeney Dr Barry Neish All the Micro staff at CMFT Prof Neil Woodford

Similar presentations









>")
 Enzymatic modification (erm )>")







 bacteraemia: impact on survival Single-centre retrospective cohort.>")
randomised trials: N=7,863 pts with sepsis: any BL monoTx vs any combination of BL + AG: N (studies) : same.>")