Download presentation
Presentation is loading. Please wait.

2
Fever Without Localizing Signs in 2013 Coburn Allen, MD Pediatric Infectious Diseases Pediatric Emergency Medicine Dell Children’s Hospital

3
Objectives Discuss the epidemiology of serious bacterial infections in febrile young children. Review recent research that is relevant to this population. Present evidence based recommendations (when available) for the evaluation and treatment of these processes.
 for the evaluation and treatment of these processes..")
4
Definitions Fever = 38°C (100.4°F), 39°C (102.2°F) often used after 2-3 months Hypothermia < 36°Celsius (96.8°F) Hyperpyrexia > 105.5 or 106° F SBI = Serious Bacterial Infections Neonate = 0-28 days Young Infant = 0-60 (or up to 90) days FWLS = 0-36m old child with fever < 7d and no recognized source after H/P, “non-toxic” Fever of Unknown Origin (prolonged, all ages)
, 39°C (102.2°F) often used after 2-3 months Hypothermia < 36°Celsius (96.8°F) Hyperpyrexia > or 106° F SBI = Serious Bacterial Infections Neonate = 0-28 days Young Infant = 0-60 (or up to 90) days FWLS = 0-36m old child with fever < 7d and no recognized source after H/P, non-toxic Fever of Unknown Origin (prolonged, all ages)")
5
Toxic Criteria “Toxic” appearance (A.K.A. septic) Lethargy Poor perfusion Marked hypo/hyperventilation Cyanosis “Toxic” patients = full evaluation 20% of “toxic” 0-90 day old children have and SBI
 Lethargy Poor perfusion Marked hypo/hyperventilation Cyanosis Toxic patients = full evaluation 20% of toxic 0-90 day old children have and SBI.")
6
SBI Epidemiology in FWLS UTI (most common) High risk populations (6-8+%) Girls 0-24m Boys 0-6m, uncirc’d to 12m VUR, anatomic issues, recurrent UTIs E. coli >> other GNRs, enterococcus Occult bacteremia (OB)+/- meningitis 0-2 months: GBS, E. Coli, Listeria 2-36 months Pneumococcus #1, decreased 85% if PCV
+/- meningitis 0-2 months: GBS, E. Coli, Listeria 2-36 months Pneumococcus #1, decreased 85% if PCV.")
7
SBI Epidemiology H. flu era (before1990) Pneumococcus #1 H. flu type B Meningococcus Post H. flu era (1990s) Pneumococcus #1 Salmonella Meningococcus Pneumococcal vaccine(s) era (2000s)
 Pneumococcus #1 Salmonella Meningococcus Pneumococcal vaccine(s) era (2000s).")
8
Post-HiB SBI Epidemiology Occult bacteremia Lee and Harper, 1998; 3-36m, T > 102.2 F 1.6% occult bacteremia 92% pneumococcus, 5% Salmonella Alpern et al, 1999; 2-24m, T > 102.2 F 1.9% occult bacteremia 83% pneumococcus, 5% Salmonella, 5% GABHS 0.03% meningitis/death UTI Boys (< 1 year) 2-3%, 8% if uncircumcised Girls (0-2 years) 6-8%, 20-30% white infants
 2-3%, 8% if uncircumcised Girls (0-2 years) 6-8%, 20-30% white infants")
9
Pneumococcal Conjugate Vaccine (PCV), “Prevnar” FDA, February 2000 7 serotypes (4, 6b, 9v, 14, 18c, 19f & 23f) Black, et al., PIDJ 2000 Double blind, Prevnar or meningococcus C 37,868, randomized 1:1, 4 year follow-up 40 cases invasive pneumococcus (fully vaccinated) 39 of 40 in meningococcal group 97.4% efficacy for vaccine serotypes, 89.1% all serotypes 7% less OM, 20% less PETs, 20% less pneumonia Alpern, et al., 2001 FWLS, occult bacteremia 97% pneumoccus serotypes covered (83% expected) Suggests the serotypes selected for vaccine focused on OB
, Prevnar FDA, February 2000 7 serotypes (4, 6b, 9v, 14, 18c, 19f & 23f) Black, et al., PIDJ 2000 Double blind, Prevnar or meningococcus C 37,868, randomized 1:1, 4 year follow-up 40 cases invasive pneumococcus (fully vaccinated) 39 of 40 in meningococcal group 97.4% efficacy for vaccine serotypes, 89.1% all serotypes 7% less OM, 20% less PETs, 20% less pneumonia Alpern, et al., 2001 FWLS, occult bacteremia 97% pneumoccus serotypes covered (83% expected) Suggests the serotypes selected for vaccine focused on OB")
10
Post-PCV Era FWLS Epidemiology Stoll et al., Arch Pediatr Adolesc Med, 2004 Retrospective, 12/2001-3/2003, NY Pedi EC 329 2-36m FWLS (T>39C) 3 (0.9%) occult bacteremia (all pneumococcus) One child twice, no Prevnar Other child had serotype not in vaccine 4 (1.2%) contaminants Only 28% at 7m and 66% at 12m “UTD” CBC poor screening test
 3 (0.9%) occult bacteremia (all pneumococcus) One child twice, no Prevnar Other child had serotype not in vaccine 4 (1.2%) contaminants Only 28% at 7m and 66% at 12m UTD CBC poor screening test")
11
Post-PCV Era Occult Pneumococcal BCx + Carstairs et al., Ann Emerg Med, June 2007 San Diego 2000-2002, T > 100.4, BCx done Compared any Prevnar to none

12
Post-PCV Era Occult Pneumococcal BCx + Unvaccinated 13 of 550 (2.4%) pneumococcal + All over 28d Half had pneumonia and bacteremia Vaccinated (any) NO pneumococcal cases 15 contaminants (1.8%) 2 had E. coli + BCx with UTIs Carstairs et al., Ann Emerg Med, June 2007

13
Other Post-Prevnar Data MMWR, 2/08 77% reduction in “invasive Pneumococcal disease” Herd immunity for unvaccinated Arch Dis Child, 6/2008 Compared occult bacteremia rates (Duke) Post Prevnar era FWLS BCx + 14 contaminants, 1 pathogen (no S. pneumo) 95% reduction in OB rates pre/post Prevnar 50% of FWLS pts. received abx Eur J Emerg Med, 8/2009 Spain, Retrospective, 3-36 m with FWLS OB 0.23% if 2 Prevnar, 0.82% if < 2 doses
 95% reduction in OB rates pre/post Prevnar 50% of FWLS pts. received abx Eur J Emerg Med, 8/2009 Spain, Retrospective, 3-36 m with FWLS OB 0.23% if 2 Prevnar, 0.82% if < 2 doses.")
14
TCH Experience: Pneumococcal Bacteremia

15
TCH Experience: Pneumococcal Meningitis

16
Typical SBI Pathogens in Young Infants Prospective Cohort: 1-90 d/o with fever (38°C) presenting to EC 1999-2002 N =1298 febrile infants 105 (8%) SBI UTI in 77 (73%) = 6% of cohort 63 of 77 were E. coli 6 of 77 had + BCx (all E. coli) 1 of 77 had + CSF (Serratia marcesens) Bacteremia in 28 (26%) = 2% of cohort Meningitis in 9 (8%) = 0. 7% of cohort 53% of pathogens resistant to ampicillin Byington CL, Pediatrics 2003
 1 of 77 had + CSF (Serratia marcesens) Bacteremia in 28 (26%) = 2% of cohort Meningitis in 9 (8%) = 0. 7% of cohort 53% of pathogens resistant to ampicillin Byington CL, Pediatrics")
17
Resistance Concerns 1-90d Byington CL, Pediatrics 2003

18
What is Causing Occult Bacteremia Now? Herz et al., PIDJ 4/06

19
EBM Approach to FWLS Understand/assign risk (high vs. low) Look for a source Tests, if needed Treat, if needed Good anticipatory guidance and follow-up
 Look for a source Tests, if needed Treat, if needed Good anticipatory guidance and follow-up.")
20
Low Risk SBI Criteria in Young infants with FWLS Clinical Criteria 1. Previously healthy, term infant 2. Non-toxic 3. No focal bacterial infection (except OM) Laboratory Criteria 1. WBC 5-15K, <1.5K bands, or b/n ratio <0.2 2. Gram stain un-spun urine negative (preferred), or neg LE and nitrite, or <5 WBC/hpf 3. If diarrhea, <5 WBC/hpf in stool 4. If CSF done, <8 WBC/mm 3 and NOS
 Laboratory Criteria 1. WBC 5-15K, <1.5K bands, or b/n ratio < Gram stain un-spun urine negative (preferred), or neg LE and nitrite, or <5 WBC/hpf 3. If diarrhea, <5 WBC/hpf in stool 4. If CSF done, <8 WBC/mm 3 and NOS.")
21
“Low Risk Young Infants” Review of literature: Baraff, 2000 Total = 3,161, 1420 “low risk” Total SBI rate 0.9% in low risk 0.4% UTI 0.4% Occult Bacteremia 0.2% Bacterial Enteritis NO Bacterial Meningitis in any of the low risk 0-90 day olds from any of the studies

22
What is a viral source?

23
Viral Sources: Young Infants RSV + Vanderbilt, retrospective cohort (Titus and Wright) 0-8 weeks, fever (38C), full eval in EC 174 RSV+ 2 with SBI (UTIs) Corpus Christi, retro cohort (Purcell and Fergie) 0-90 d/o with RSV+ bronchiolitis No bacteremia/meningitis 1.1% UTI Influenza Krief WI, et. al., Pediatrics, July 2009 0-60d, fever (100.4), rapid flu + vs – Flu +, 2.5% with SBI, (2.4% UTI) Flu -, 13.3% with SBI, (10.8% UTI, 2.2% bacteremia, 0.9% mening) Recommend urine in Flu +
, rapid flu + vs – Flu +, 2.5% with SBI, (2.4% UTI) Flu -, 13.3% with SBI, (10.8% UTI, 2.2% bacteremia, 0.9% mening) Recommend urine in Flu +.")
24
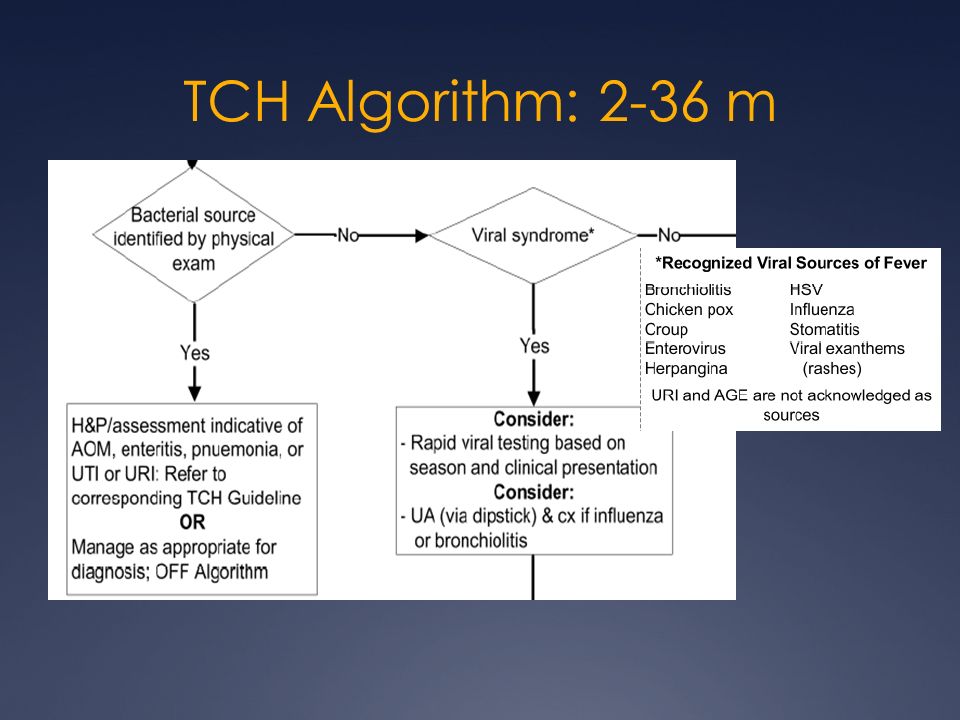
Viral Sources: Older Kids Greenes and Harper, PIDJ 1999 3-36m, T > 102.2 F, blood culture done Viral syndrome, 2 of 876 (0.2%) bacteremia Bronchiolitis, 1 of 411 (0.2%) Croup, 0 of 249 Stomatitis, 0 of 123 Varicella, 1 of 93 (1.1%) 1.4% BCx = contaminants Kuppermann, Arch Ped Adol Med 1997 156 < 2y/o w/ bronchiolitis; 0 Bcx +, 2% UTI
 bacteremia Bronchiolitis, 1 of 411 (0.2%) Croup, 0 of 249 Stomatitis, 0 of 123 Varicella, 1 of 93 (1.1%) 1.4% BCx = contaminants Kuppermann, Arch Ped Adol Med 1997 156 < 2y/o w/ bronchiolitis; 0 Bcx +, 2% UTI")
25
Is Diarrhea a Source? Prospective, Texas Children’s 3-24 m/o, FWLS, w/ or w/o diarrhea Cath Ucx if at risk for UTI Boys 0-6m (circ), 0-12 (uncirc) Girls 3m-24m Results (N = 231) No diarrhea: 12.4% had UTI Diarrhea: 8.5 % had UTI Cardone G, Allen CH, Caviness C, AAP 2009 NCE, Washington, D.C.
, 0-12 (uncirc) Girls 3m-24m Results (N = 231) No diarrhea: 12.4% had UTI Diarrhea: 8.5 % had UTI Cardone G, Allen CH, Caviness C, AAP 2009 NCE, Washington, D.C..")
26
Newer OB Screening Tools Absolute neutrophil count (Kuppermann, An Emerg Med 1998) Occult bacteremia, 3-36m > 10,000 = 8.1% vs. < 10,000 = 0.8% Sensitivity 76%, specificity 78% C-reactive protein (Pulliam, Peds 2001) SBI, 1-36m CRP > 7, sens 79%, spec 91% Procalcitonin (Lopez, PIDJ 2003) SBI vs. viral, 1-36m PCT > 0.6, sens 70%, spec 94%
 SBI, 1-36m CRP > 7, sens 79%, spec 91% Procalcitonin (Lopez, PIDJ 2003) SBI vs. viral, 1-36m PCT > 0.6, sens 70%, spec 94%.")
27
SBI Markers Study Manzano, et. al., Arch. Dis. Child, Jan 2011 Prospective cohort, Quebec, 11/06-11/07 (90%+ UTD) 1-36m, FWLS (38C), had CBC, BCx, UA/Cx, PCT, CRP Compared labs vs. PE to detect SBI Results 328 (of 457) met inclusion criteria, 29% < 6m 16% (N= 54) with SBI 89% UTIs (2 of 48 bacteremic, 2 of 48 had nl UA) 7% (N = 4) “Pneumonia” 2% (N = 1) Meningitis (meningococcal B) 2% (N = 1) Occult bacteremia (S. pneumo 33)
 1-36m, FWLS (38C), had CBC, BCx, UA/Cx, PCT, CRP Compared labs vs. PE to detect SBI Results 328 (of 457) met inclusion criteria, 29% < 6m 16% (N= 54) with SBI 89% UTIs (2 of 48 bacteremic, 2 of 48 had nl UA) 7% (N = 4) Pneumonia 2% (N = 1) Meningitis (meningococcal B) 2% (N = 1) Occult bacteremia (S. pneumo 33).")
28
SBI Markers ROCs No significant difference for AUC for all 4 blood tests All were better than exam alone (VAS)
")
29
SBI Markers…

30
SBI Markers if UA normal (do they help?) Only had 8 SBIs with normal UA 2 UTIs (would have caught with Ucx) 4 “Pneumonias” (could have been viral) 1 Meningitis (no details provided) 1 Occult bacteremia
 Only had 8 SBIs with normal UA 2 UTIs (would have caught with Ucx) 4 Pneumonias (could have been viral) 1 Meningitis (no details provided) 1 Occult bacteremia")
31
Does having a PCT change clinical decisions? Manzano (same) et. al., Am. J. Emer. Med 2010 Same study population Half knew PCT value, half didn’t know No difference in abx prescribing No difference in decision to hospitalize Value of the test “uncertain”

32
Occult Pneumonia Bachur et al., An Emerg Med 1999 WBC > 20,000, T > 102.2 Normal PE = 26% occult pneumonia Abnormal respiratory exam = 40% pneumonia Bacteremia No difference; pneumonia vs. no pneumonia 6.5% overall, all pneumococcus TCH post-PCV7 experience WBC > 25k better predictor of + CXR Lemke D, Allen CH, SPR 2010

33
UTI Screening “Enhanced urinalysis” (Hoberman, Peds 1993) Unspun urine Pyuria; > 10 WBC/hpf hemocytometer OR Bactiuria (any) on Gram stain Sensitivity 95.8%, specificity 92.6% If neither, NPV 99.8% Spun urine Gram stain 93% sensitive Dip for LE or nitrite 88% sensitive Sensitivities drop in young infants, 70-80%
 Unspun urine Pyuria; > 10 WBC/hpf hemocytometer OR Bactiuria (any) on Gram stain Sensitivity 95.8%, specificity 92.6% If neither, NPV 99.8% Spun urine Gram stain 93% sensitive Dip for LE or nitrite 88% sensitive Sensitivities drop in young infants, 70-80%")
34
Management of FWLS 0-28d Full evaluation CBC, BCx Cath UA, UCx LP, +/- Rapid viral testing Consider LFTs in first 2 weeks Admit IV Abx Amp/Gent (or observe off) if “low risk” UA +, consider 3 rd gen. cephalosporin Gram stain+, adjust therapy IV Acyclovir if HSV suspected

35
HSV Risk Factors Caviness, et. Al., PIDJ 5/2008

36
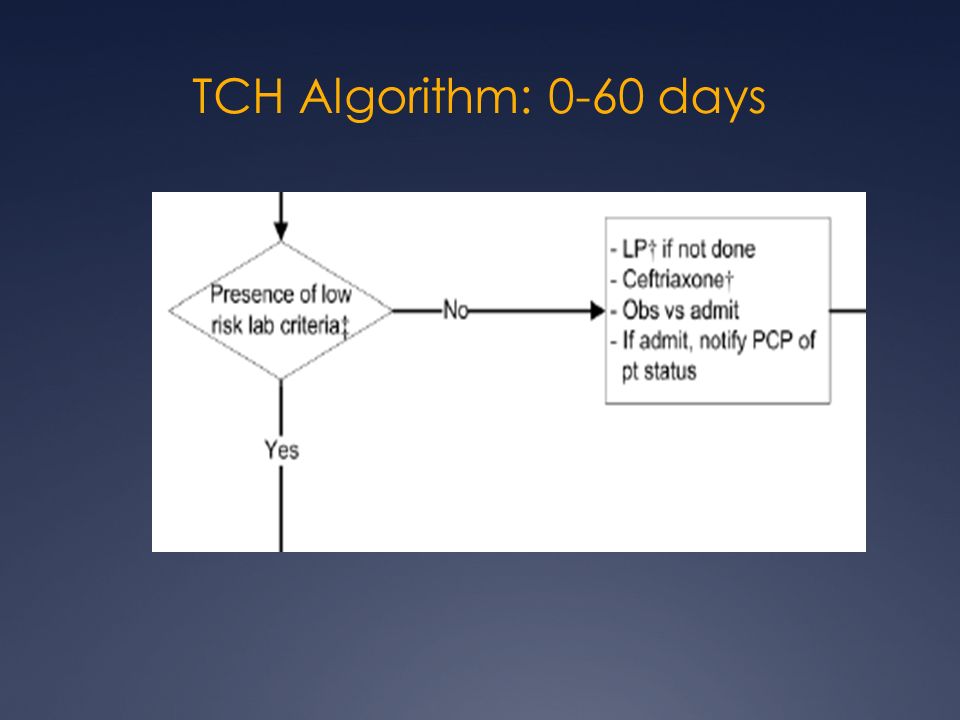
Management FWLS 29-60d Evaluation CBC, BCx Cath Ua, UCx CSF if high risk, concern for meningitis Categorize risk High risk: Admit, LP if not done, IV abx Abx based on screening UA +, consider 3rd gen cephalosporin Abnl WBC, consider ampicillin and cefotaxime LP abnl, based on stain, if Gram stain-, vanc/ctx Low risk: Discharge, no abx without LP Ceftriaxone 50mg/kg if abx F/u 1 day

37
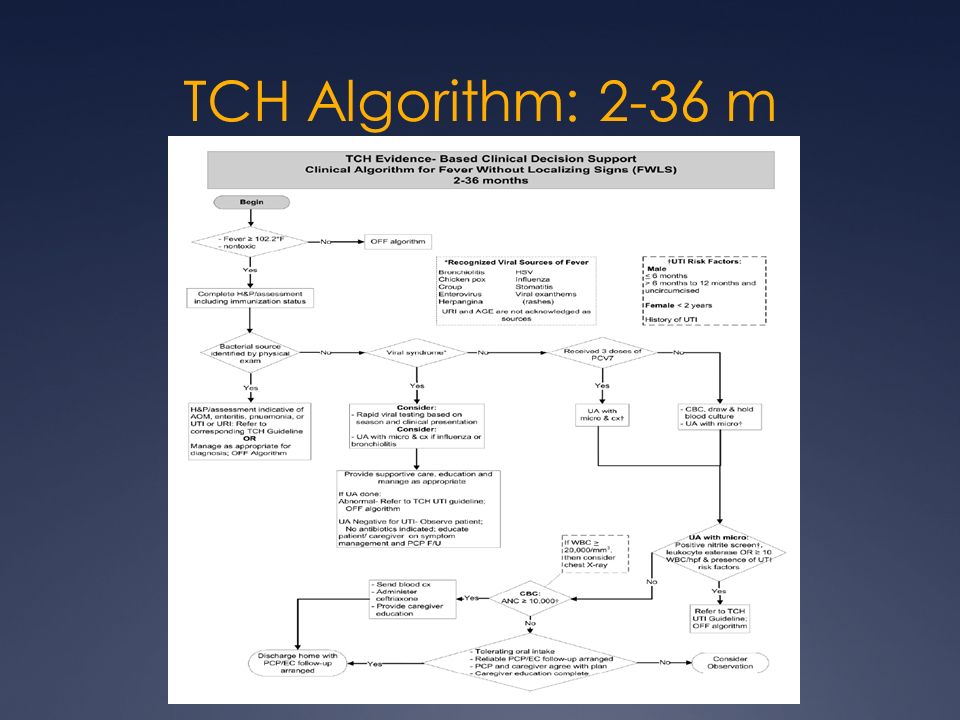
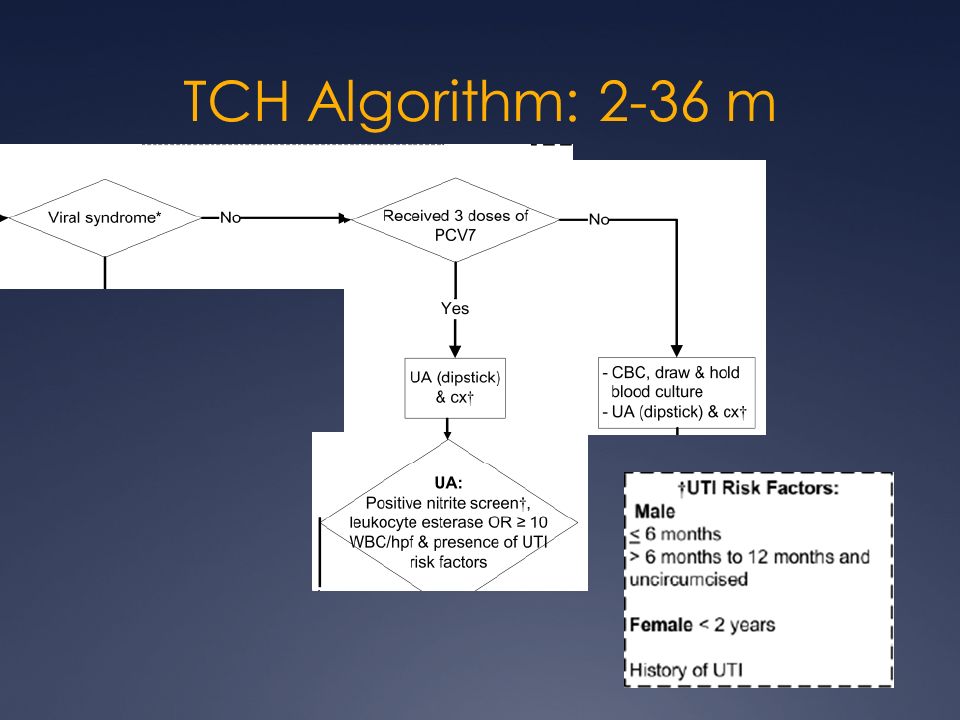
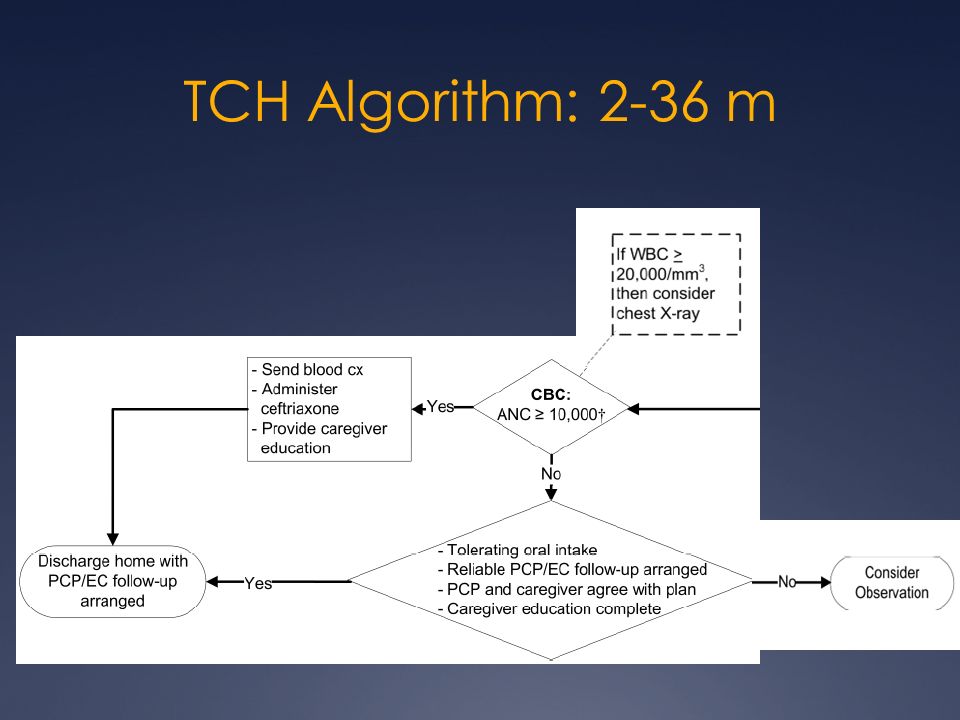
Management FWLS 2m-3y Evaluation CBC (and hold BCx) Less than 6 months (some say 4m) Unimmunized (HiB, PCV) No viral source Cath/CC UA, UCx Boys 0-6m, 6-12 if uncirc’d Girls 0-24m Low threshold if h/o recurrent UTIs, > 2 d fever Rapid viral testing if changes care Flu in high risk populations Send BCx if ANC > 10k, DON’T if not CXR if WBC > 20-25k
 Less than 6 months (some say 4m) Unimmunized (HiB, PCV) No viral source Cath/CC UA, UCx Boys 0-6m, 6-12 if uncirc’d Girls 0-24m Low threshold if h/o recurrent UTIs, > 2 d fever Rapid viral testing if changes care Flu in high risk populations Send BCx if ANC > 10k, DON’T if not CXR if WBC > 20-25k")
38
Management FWLS 2m-3y Disposition Most discharged home, f/u 1-2 days Decisions to treat ANC > 10k; 50mg/kg IM ceftriaxone UA+; 3 rd gen PO cephalosporin Pneumonia; PO beta lactam (i.e. amox) Anticipatory guidance Antipyretics What to expect/worry about Expect fever 3-5+ days for most viral illnesses Return if SOB, dehydration, irritable/lethargy/AMS
 Anticipatory guidance Antipyretics What to expect/worry about Expect fever 3-5+ days for most viral illnesses Return if SOB, dehydration, irritable/lethargy/AMS.")
39
Management FWLS 2m-3y Positive Blood Cultures (Allen CH, UpToDate) All should be reevaluated Contaminant vs. Pathogen Gram stain Time to positivity GPCs pairs/chains or confirmed Pneumococcus Febrile: LP, if neg ceftriaxone home on PO amox 30-40 % still bacteremic 4% meningitis Afebrile/Well: reculture, no LP, PO amox Other Pathogens: BCX, LP (except E. coli and Staph aureus after 3m), admit IV abx
, admit IV abx.")
40
FWLS Epi: National Trends Simon AE, et. Al., Peds Emerg Care, 6/2013 1.6 million visits/yr, for FWLS in 2-24m in 2009 20% of ER visits in 2-24 m are for FWLS Decreased blood work done since 2004 No significant change in UAs Simon AE, et. Al., Peds, 12/11 No tests in 56% of FWLS, 3-36m 20% get CBC 17% got UA (only 40% of girls with 39 C)
.")
41
Happy Hunting!

42
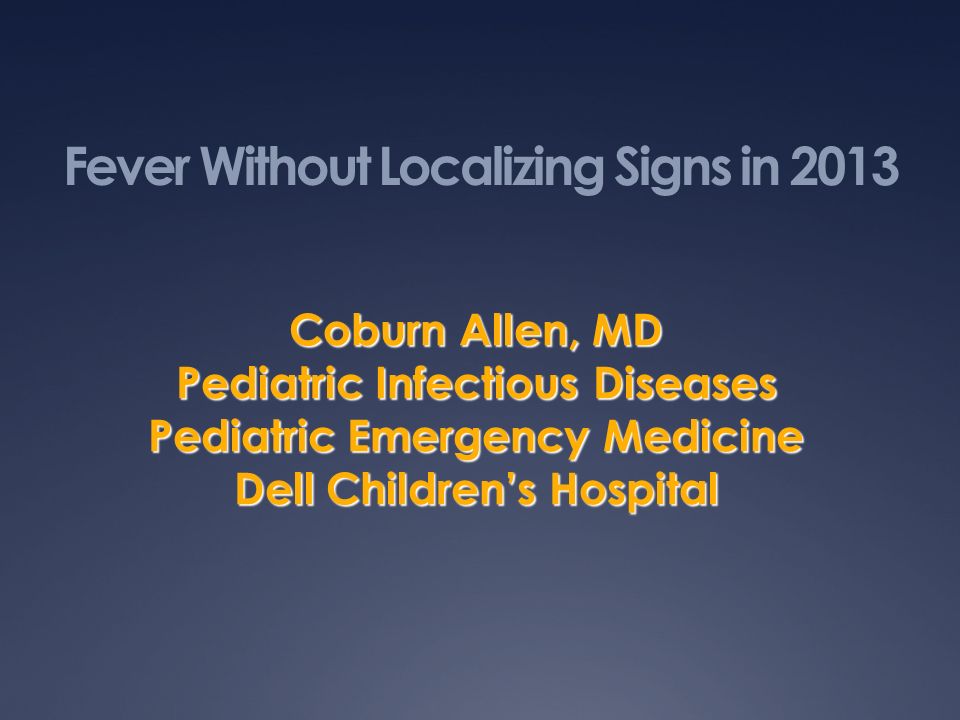
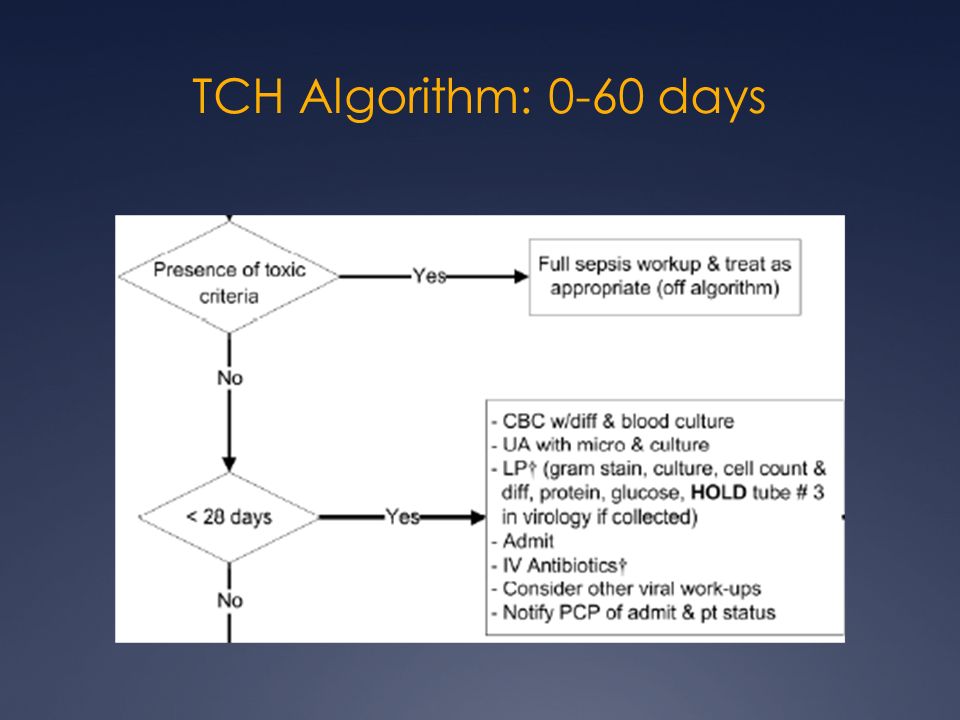
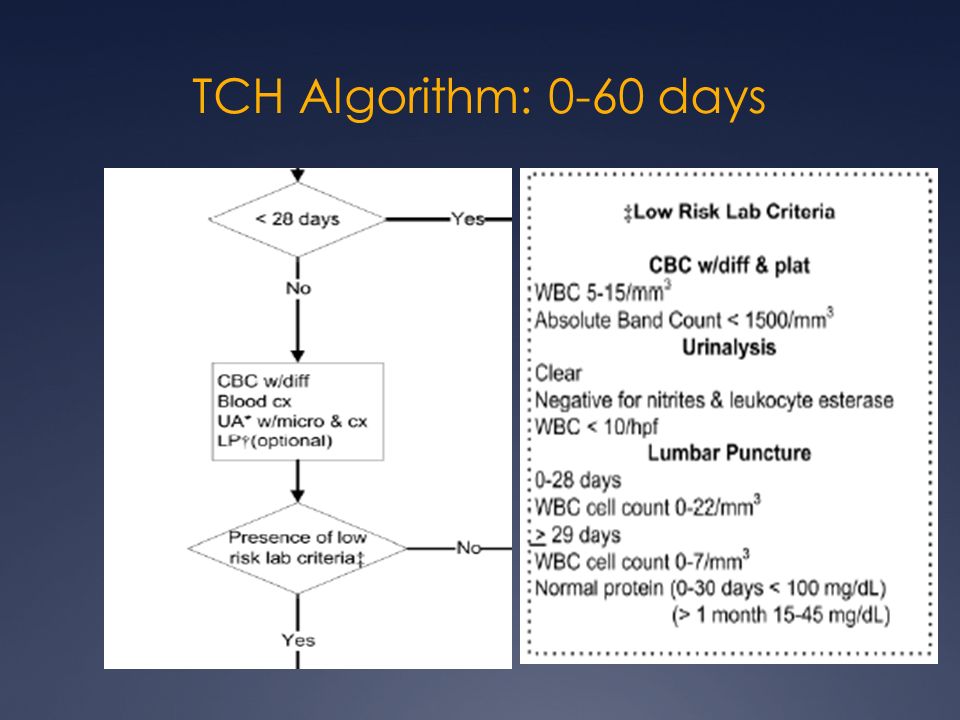
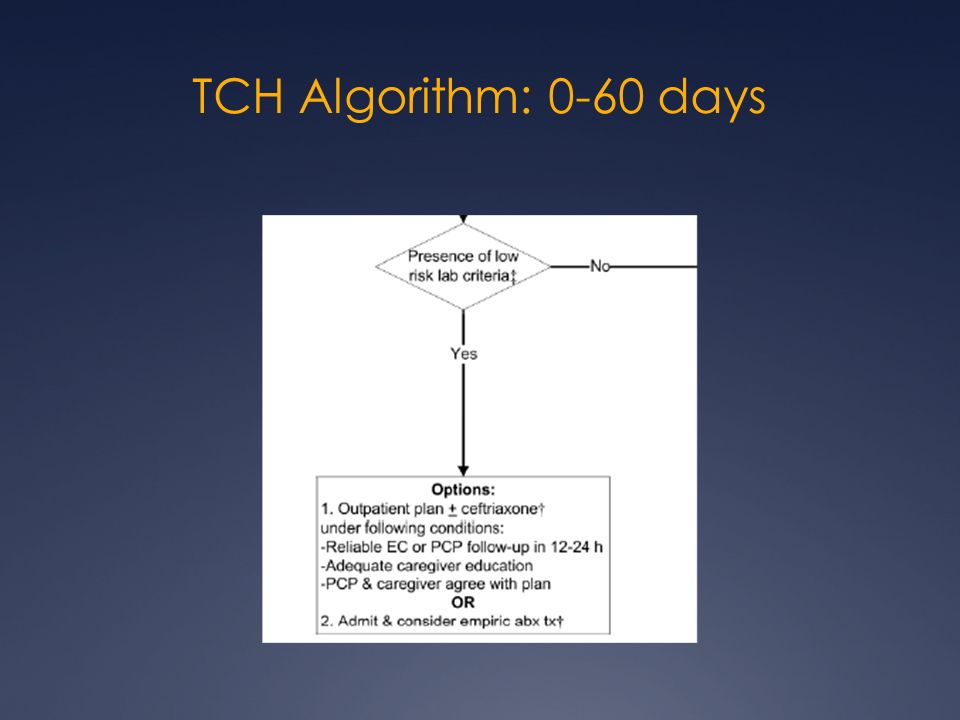
TCH Algorithm: 0-60 days

48
TCH Algorithm: 2-36 m

53
Q/A

Similar presentations







. First described.>")





 –Physical exam findings unreliable –Immunologic.>")





