Download presentation
Presentation is loading. Please wait.

1
Musculoskeletal block Pathology practical

2
Normal anatomy and histology

4
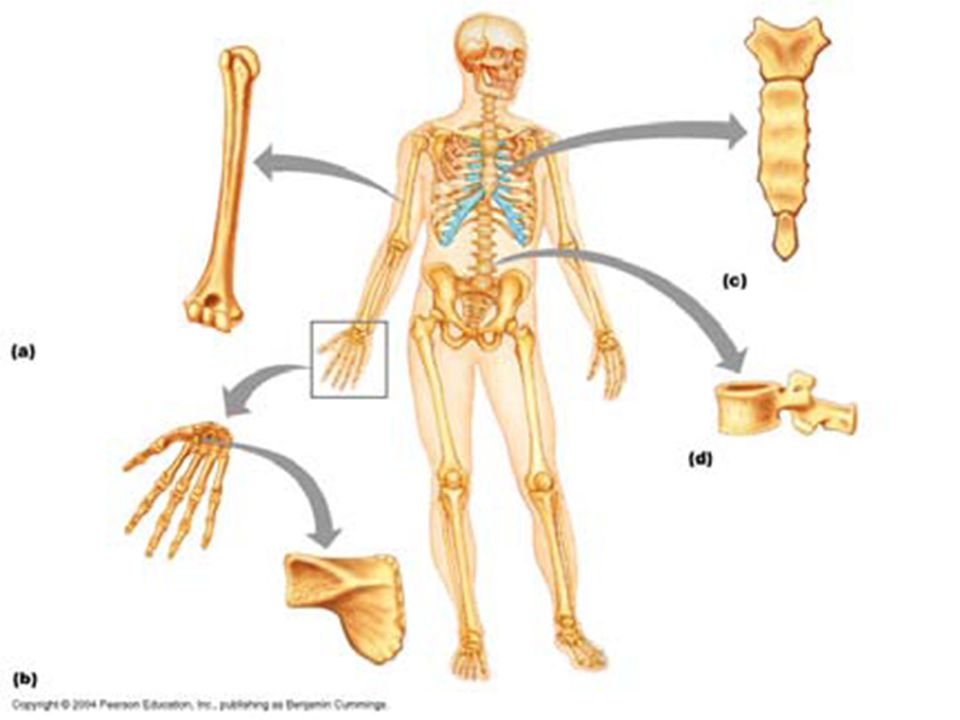
The overall structure of a long bone

7
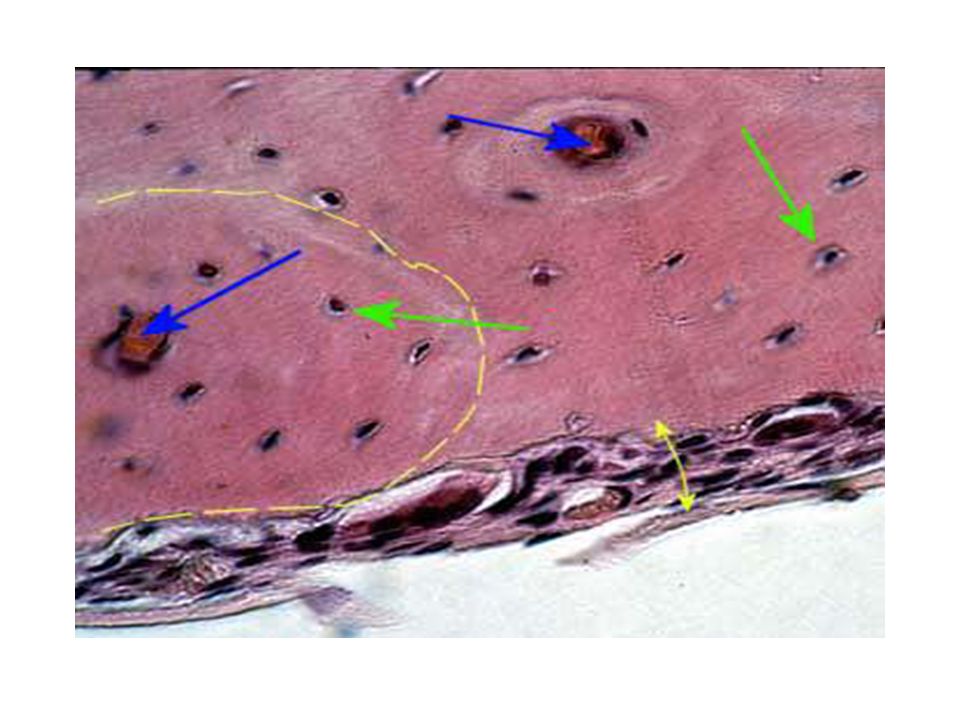
Here is normal cancellous bone as seen under polarized light microscopy, which highlights the lamellar structure. The bony spicules are even, with occasional lacunae containing osteocytes. Cellular marrow is seen between the spicules of bone.

8
Gross pathology and histopathology

9
Case no. 1

10
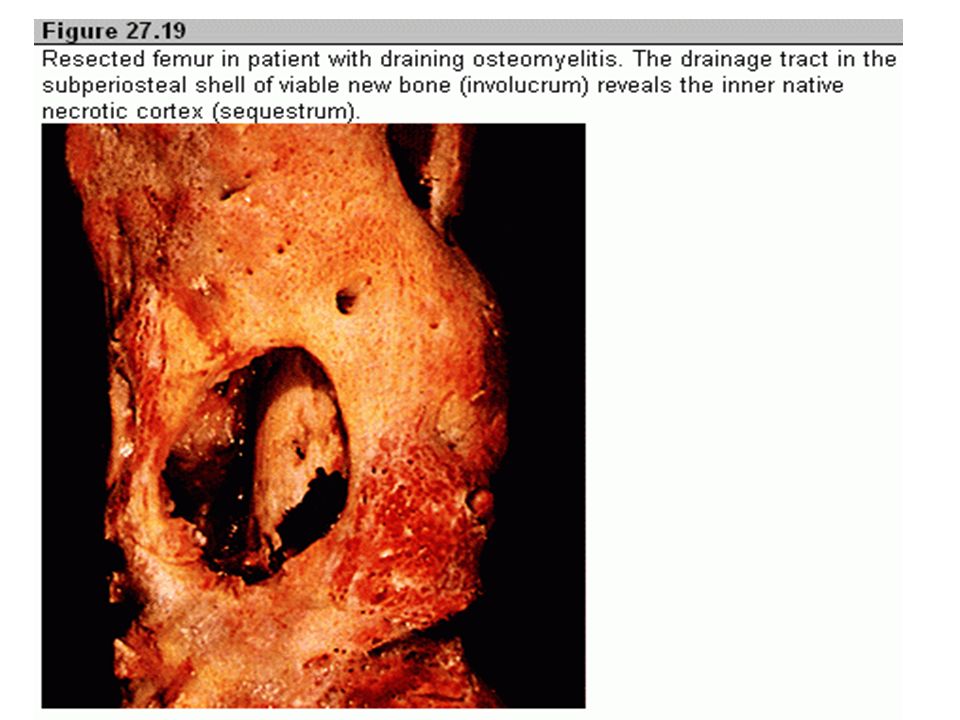
A 22 years old male presented with localized pain above his right knee joint with recurrent fever. Later, he had a discharging sinuses from the skin overlying the right knee What is the most likely diagnosis ?

13
This is chronic osteomyelitis
This is chronic osteomyelitis. Note the fibrosis of the marrow space accompanied by chronic inflammatory cells. There can be bone destruction with remodelling. Osteomyelitis is very difficult to treat.

14
Osteomyelitis

16
Case no. 2

17
A 35 years old debilitated man presented to the orthopedic clinic with back pain, low grade fever, marked elevation of sedimentation rate and recent kyphosis and scoliosis . The patient has a history of coughing up blood, fever, chills, night sweats, weight loss, pallor, and often a tendency to fatigue very easily.

20
Section of bone shows granuloma formation with epithelioid like cells , langhans-type giant cells and rim of lymphocytes . Section of bone shows granuloma formation with epithelioid like cells , langhans-type giant cells and rim of lymphocytes

21
2- Spinal TB - Potts Disease (Tuberculous osteomyelitis)
")
23
Case no. 3

24
A 40 years old woman complains of low grade fever , malaise and stiffness in her joints each morning .

25
Swollen and slightly deformed interphalangeal joints.
Tumor necrosis factor (TNF) plays central role in the pathogenesis of this disease.
 plays central role in the pathogenesis of this disease.")
26
Rheumatoid arthritis affecting the head of femur.
The synovium becomes edematous, thickened and hyperplastic and transforming its smooth contour to one covered by delicate and bulbous fronds .

27
Section shows marked synovial hypertrophy with formation of villi

28
Section of synovial tissue showing
Hyperplastic synovium which is infiltrated by dense chronic inflammatory cells including many lymphocytes and plasma cells.

29
3- Rheumatoid arthritis

31
Case no. 4

32
An obese 56 years old woman presented with bilateral localized pain to her knees, hands and difficulty in walking .

33
Progressive erosion of articular cartilage, eburnated articular surface , subchondral cyst and residual articular cartilage (Osteoarthritis) Progressive erosion of articular cartilage, eburnated articular surface , subchondral cyst and residual articular cartilage Predisposing factors for osteoarthritis are marked obesity , previous injuries to a joint , diabetes and deformed joint .
 Progressive erosion of articular cartilage, eburnated articular surface , subchondral cyst and residual articular cartilage. Predisposing factors for osteoarthritis are marked obesity , previous injuries to a joint , diabetes and deformed joint .")
34
Mushroom-shaped osteophytes (bony outgrowths ) develop at the margins of the articular surface and are capped by fibrocartilage and hyaline cartilage that gradually ossify . (Osteoarthritis) Mushroom-shaped osteophytes (bony outgrowths ) and splitting of articular cartilage . There is absence of inflammation .
 Mushroom-shaped osteophytes (bony outgrowths ) and splitting of articular cartilage . There is absence of inflammation .")
35
4- Osteoarthritis

37
Case no. 5

38
A 16 years old male was found to have a small swelling protruding from upper part of his leg with local pain .

39
This is an osteochondroma of bone
This is an osteochondroma of bone. This lesion appears as a bony projection (exostosis). Most are solitary, incidental lesions that may be excised if they cause local pain. There is a rare condition of multiple osteochondromatosis marked by bone deformity and by a greater propensity for development of chondrosarcoma. This is an osteochondroma of tibial bone. This lesion appears as a bony projection (exostosis). Most are solitary, incidental lesions that may be excised if they cause local pain. There is a rare condition of multiple osteochondromatosis marked by bone deformity and by a greater propensity for development of chondrosarcoma.
. Most are solitary, incidental lesions that may be excised if they cause local pain. There is a rare condition of multiple osteochondromatosis marked by bone deformity and by a greater propensity for development of chondrosarcoma. This is an osteochondroma of tibial bone. This lesion appears as a bony projection (exostosis). Most are solitary, incidental lesions that may be excised if they cause local pain. There is a rare condition of multiple osteochondromatosis marked by bone deformity and by a greater propensity for development of chondrosarcoma.")
40
A bluish-white cartilagenous cap overlies the bony cortex.
These are probably not true neoplasms, but they are a mass lesion that extends outward from the metaphyseal region of a long bone. A bluish-white cartilagenous cap overlies the bony cortex. These are probably not true neoplasms, but they are a mass lesion that extends outward from the metaphyseal region of a long bone.

41
The microscopic appearance of an osteochondroma displays the benign cartilagenous cap at the left upper and the bony cortex at the right lower. This bone growth, though benign, can sometimes cause problems of pain and irritation that leads to removal surgically. It is a benign tumor with very rare incidence of malignant transformation The microscopic appearance of an osteochondroma displays the benign cartilagenous cap at the left upper and the bony cortex at the right lower. This bone growth, though benign, can sometimes cause problems of pain and irritation that leads to removal surgically.

42
Osteochondroma of bone.
This is an osteochondroma of bone. Osteochondroma of bone.

43
5- Osteochondroma (osteochondroma exostosis)
")
45
Case no. 6

46
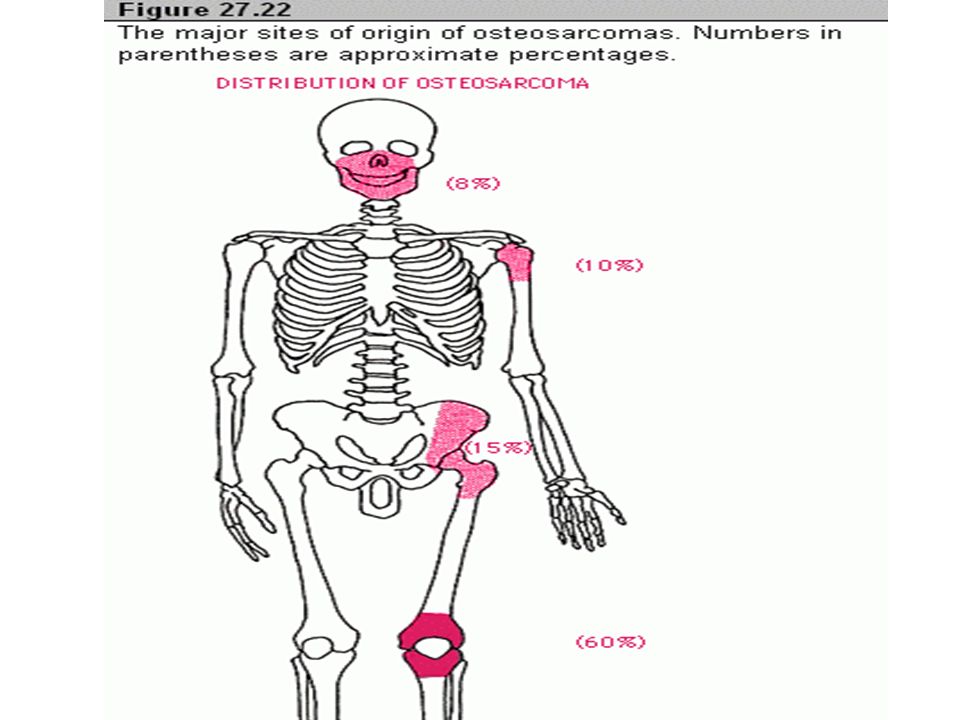
An 18 years old female presented to the rheumatology clinic with 2 months history of pain and swelling in her upper thigh with weight loss .

47
Conventional osteosarcoma

48
Mass lesion involving the upper end of the tibial bone.
The mass show pale, yellowish cut surface with few hemorrhagic areas. Conventional osteosarcoma Mass lesion involving the upper end of the tibia bone. The mass show pale, yellowish cut surface with few hemorrhagic areas.

49
Osteosarcoma Malignant osteoid, Malignant pleomorphic cells showing abnormal mitoses

50
Predisposing factors which may lead to the development of the lesion : Paget’s disease , Radiation, fibrous dysplasia

51
6-Osteosarcoma

54
Case no. 7

55
Case no. 7

56
A 3 years old boy presented to his pediatrician with complaint of his parents from difficulty in walking , poor balance , and frequent falls . Laboratory investigation shows elevated creatine kinase . Muscle biopsy show absence of dystrophin by western blot analysis What is your provisional diagnosis?

57
clinical features seen in picture : Deformed back, foot drop and asymmetrical calf muscles atrophy

58
Etiology: Abnormalities in the dystrophin gene located on the short arm of the X-chromosome.
DMD showing variations in muscle fiber size , increased endomysial connective tissue , and regenerating fibers (blue hue) . Also there is fiber loss and adipose tissue infiltration
 . Also there is fiber loss and adipose tissue infiltration.")
59
Note again the atrophy/hypertrophy scenario

60
Dystrophin, an intracellular protein, forms an interface between the cytoskeletal proteins and a group of transmembrane proteins NORMAL DMD

61
7-Duchenne muscular dystrophy

63
Case no.8

64
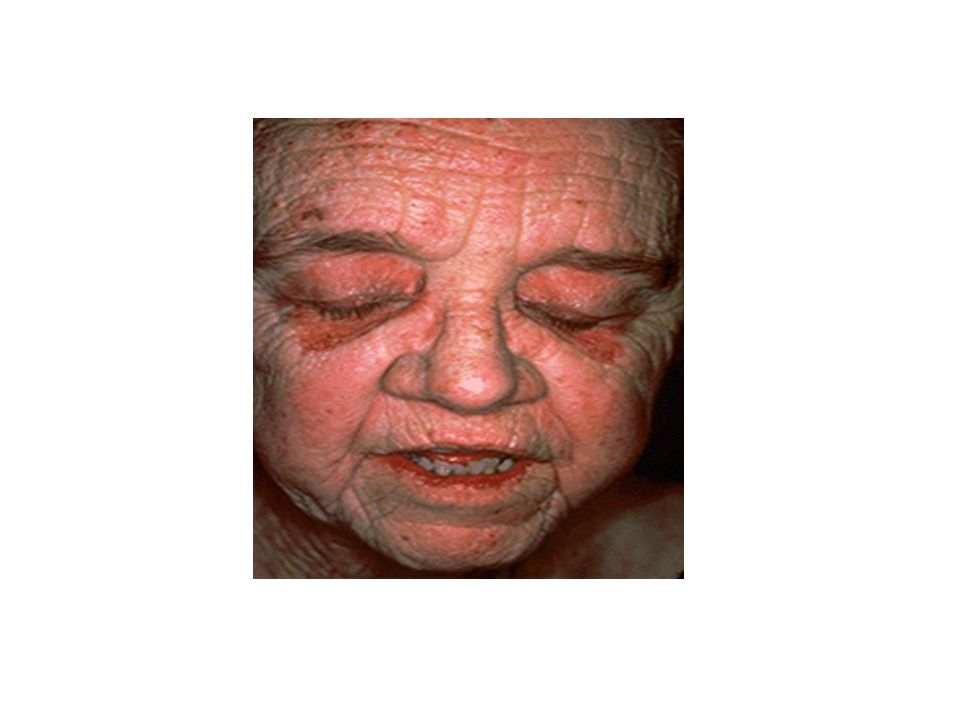
A 52-year-old woman presents with 6-month history of progressive muscle weakness and a skin rash.
Physical examination is remarkable for a diffuse purple/red discoloration of the skin over her cheeks, nose, and eyelids. Examination confirms proximal muscle weakness. Laboratory findings show an increase in creatine kinase (10 times the normal).
.")
66
The histologic appearance of muscle shows perifascicular atrophy of muscle fibers and inflammation .
Patient usually have positive antinuclear antibody (ANA) and increased creatine kinase . The histologic appearance of muscle shows perifascicular atrophy of muscle fibers and inflammation .
 and increased creatine kinase . The histologic appearance of muscle shows perifascicular atrophy of muscle fibers and inflammation .")
67
8-Dermatomyositis

Similar presentations













>")






>")


: It is the commonest cause of chronic inflammatory joint disease. Most typical.>")





