Download presentation
Presentation is loading. Please wait.

1
1 DG SANITA PRIMARY CARE: Regional strategies to improve efficacy and equity while guaranteeing economic sustainability Pisa, June 13, 2011 STRATEGIES AND NEW MEASUREMENTS IN PRIMARY CARE: THE CREG PROJECT IN LOMBARDY REGION Carlo ZOCCHETTI Direzione Generale Sanità – Regione Lombardia

2
Rome LOMBARDY LOMBARDY 24,000 SqKm 9.8 million inhabs (17% Italy) 17 Billion Euros health expens (17% Italy) A significant proportion of mountaineous terrain Just for starting … DG SANITA
 17 Billion Euros health expens (17% Italy) A significant proportion of mountaineous terrain Just for starting … DG SANITA")
3
Lombardy Region GDP (per cap) 33,648 (Italy 26,278 ) 220 Hospitals (30% profits) 4 beds x 1,000 inhabs 8,150 GPs 2,700 Pharmacies 730 Outpatient ambuls DG SANITA
 33,648 (Italy 26,278 ) 220 Hospitals (30% profits) 4 beds x 1,000 inhabs 8,150 GPs 2,700 Pharmacies 730 Outpatient ambuls DG SANITA")
4
Lombardy Region 2 Mln discharges 10% discharges for non residing people (50% in oncology, cardiosurgery) 3,8% passive mobility 160 Mln outpatient services 60 Mln drug prescriptions DG SANITA
 3,8% passive mobility 160 Mln outpatient services 60 Mln drug prescriptions DG SANITA")
5
15 LOCAL HEALTH AUTHORITIES (ASL) DG SANITA 100 Districts
 DG SANITA 100 Districts")
6
6 L.R. Health System:L.R. Health System: –Universal coverage; funded by general taxation; separation between Purchasers (ASL) and Services Providers (Hospitals, Ambulatories, GPs, …) –Purchasers funded by weighted capitation; Services Providers funded (mainly) on delivery of services (DRGs, List of outpatient activities, tariffs) General rules: Lombardy Region HS DG SANITA
 and Services Providers (Hospitals, Ambulatories, GPs, …) –Purchasers funded by weighted capitation; Services Providers funded (mainly) on delivery of services (DRGs, List of outpatient activities, tariffs) General rules: Lombardy Region HS DG SANITA.")
7
7 L.R. Health System:L.R. Health System: –Centered on hospitals, and acute care: inadequate to manage chronicity Requires different ideas, culture, competence, tools, instrumentsRequires different ideas, culture, competence, tools, instruments CReG: Accent on Chronicity, not primary careCReG: Accent on Chronicity, not primary care –People is getting older: Big proportion of citizens with chronic diseases or conditionsBig proportion of citizens with chronic diseases or conditions –Some figures about chronicity in Lombardy Region CReG: the problem DG SANITA

8
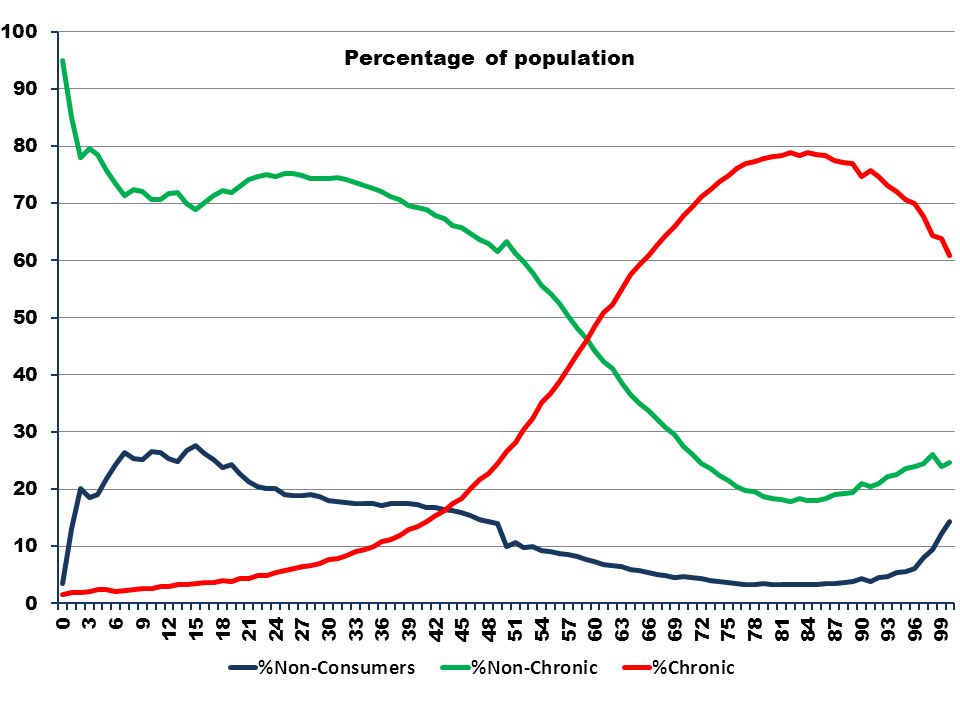
Non_ConsAcuteChronicDeath 70% of expends

11
OnlyNot Only DiseaseNumber%Euro/PCNumber%Euro/PC Transplants 618 0,0 5.543 6.857 0,2 21.846 Kidney Insuff 2.245 0,1 7.815 41.701 1,0 12.956 HIV-AIDS 15.227 1,0 7.455 27.425 0,6 9.486 Cancer 104.720 6,6 3.518 297.704 6,9 5.195 Diabetes 87.371 5,5 895 426.424 9,9 2.921 Cardiovascular 835.231 52,8 1.166 1.754.271 40,9 2.450 Pulmonary Dis 116.701 7,4 1.169 242.828 5,7 2.981 Gastro&Liver 143.076 9,0 1.269 494.394 11,5 4.014 Neurological 93.662 5,9 2.449 225.720 5,3 4.133 Autoimmune Dis 18.314 1,2 1.146 77.658 1,8 2.306 Endocr_Methabol 164.445 10,4 904 693.816 16,2 2.710

12
12 The chronic patient uses many services which do not resolve his problemsThe chronic patient uses many services which do not resolve his problems –Live longer with chronicity –Delay negative consequencies –Needs control, monitoring, and organizational acitivities: no specialization The chronic patient requires treatment planes, guidelines, for specific diseasesThe chronic patient requires treatment planes, guidelines, for specific diseases –Agreed –Finalized to obtain continuity of care –Some problems CReG: the motivations DG SANITA

13
Anti- diabeticsStatins Anti- hypertensiv TreatedMalFemMalFemMalFem Sporadic19,722,524,324,719,822,5 Adherent38,638,226,420,842,034,7 Not adherent61,461,873,679,258,065,3 Persistent57,658,651,546,557,150,6 Not persistent42,441,448,553,542,949,4

14
14 The chronic patient needs to be maintained on careThe chronic patient needs to be maintained on care –Not guaranteed by hospitals acute approach –Coordination between hospitals and primary care Is primary care prepared to face chronicity?Is primary care prepared to face chronicity? –It lacks some necessary attributes: Contractual conditionsContractual conditions Clinical, management and administrative expertiseClinical, management and administrative expertise CReG: the motivations DG SANITA

15
15 We need a new institutional subject:We need a new institutional subject: –A manager of a group of many cases In the context of L.R. health system general characteristics:In the context of L.R. health system general characteristics: –Freedom of choice of provider –Purchaser-provider split –Accreditation –Parity between public and private companies The approach emerged after some experiences, mainly with GPsThe approach emerged after some experiences, mainly with GPs CReG: the approach DG SANITA

16
16 CReG: Chronic Related GroupCReG: Chronic Related Group –Innovative way of taking care of chronic cases –A group of predefined resources (tariff) assigned to an institutional subject to guarantee the delivery of an established treatment plan to chronic patients it has in charge –Services excluded: Hospital dischargesHospital discharges GPs feesGPs fees CReG: the approach DG SANITA
 assigned to an institutional subject to guarantee the delivery of an established treatment plan to chronic patients it has in charge –Services excluded: Hospital dischargesHospital discharges GPs feesGPs fees CReG: the approach DG SANITA")
17
17 CReG requires three technological pillars:CReG requires three technological pillars: –Ability to classify people with regard to chronicity (type of diseases, staging, …) –An established treatment plan, guidelines –A reimbursement scheme (CReG tariff and some administrative stuffs) CReG requires an organizational platformCReG requires an organizational platform CReG: the approach DG SANITA
 –An established treatment plan, guidelines –A reimbursement scheme (CReG tariff and some administrative stuffs) CReG requires an organizational platformCReG requires an organizational platform CReG: the approach DG SANITA")
18
18 1. CReG: how to classify people1. CReG: how to classify people –A specific information system Hospital discharges, outpatient ambulatory services, drug consumeHospital discharges, outpatient ambulatory services, drug consume On an individual basis (PIN)On an individual basis (PIN) Paid with a pps scheme (tariffs)Paid with a pps scheme (tariffs) Services purchased outside the regionServices purchased outside the region Large coverage (98% of expenditures)Large coverage (98% of expenditures) No GPs activitiesNo GPs activities No pure private activitiesNo pure private activities –A classification scheme Also with disease exemptionsAlso with disease exemptions CReG: the pillars DG SANITA
On an individual basis (PIN) Paid with a pps scheme (tariffs)Paid with a pps scheme (tariffs) Services purchased outside the regionServices purchased outside the region Large coverage (98% of expenditures)Large coverage (98% of expenditures) No GPs activitiesNo GPs activities No pure private activitiesNo pure private activities –A classification scheme Also with disease exemptionsAlso with disease exemptions CReG: the pillars DG SANITA.")
19
CITIZEN DRUGS Consumes Hospital DISCHARGES OUTPATIENTS Activities MORTALITY PATHOLOGY Exams CANCER Registries SUPPORT and Others PSYCHIATRY SUPPLY

20
20 1. CReG: how to classify people1. CReG: how to classify people –A specific information system Hospital discharges, outpatient ambulatory services, drug consumeHospital discharges, outpatient ambulatory services, drug consume On an individual basis (PIN)On an individual basis (PIN) Paid with a pps scheme (tariffs)Paid with a pps scheme (tariffs) Services purchased outside the regionServices purchased outside the region Large coverage (98% of expenditures)Large coverage (98% of expenditures) No GPs activitiesNo GPs activities No pure private activitiesNo pure private activities –A classification scheme Also with disease exemptionsAlso with disease exemptions CReG: the pillars DG SANITA
On an individual basis (PIN) Paid with a pps scheme (tariffs)Paid with a pps scheme (tariffs) Services purchased outside the regionServices purchased outside the region Large coverage (98% of expenditures)Large coverage (98% of expenditures) No GPs activitiesNo GPs activities No pure private activitiesNo pure private activities –A classification scheme Also with disease exemptionsAlso with disease exemptions CReG: the pillars DG SANITA.")
21
CancerCancer or code 048* (or code 0043) code 048* (or code 0043) if 1exemption1exemption 2discharges2discharges 3drugs3drugs 4out-patient4out-patient codeICD9-CMbetween140* and 208* Or V10* codeICD9-CMbetween140* and 208* Or V10* ATC L01 or Chemiother. Chemiother.Radiother. (code 92.24*) Radiother. or 1 1 2 2 3 3 4 4 if
 Radiother. or if.")
23
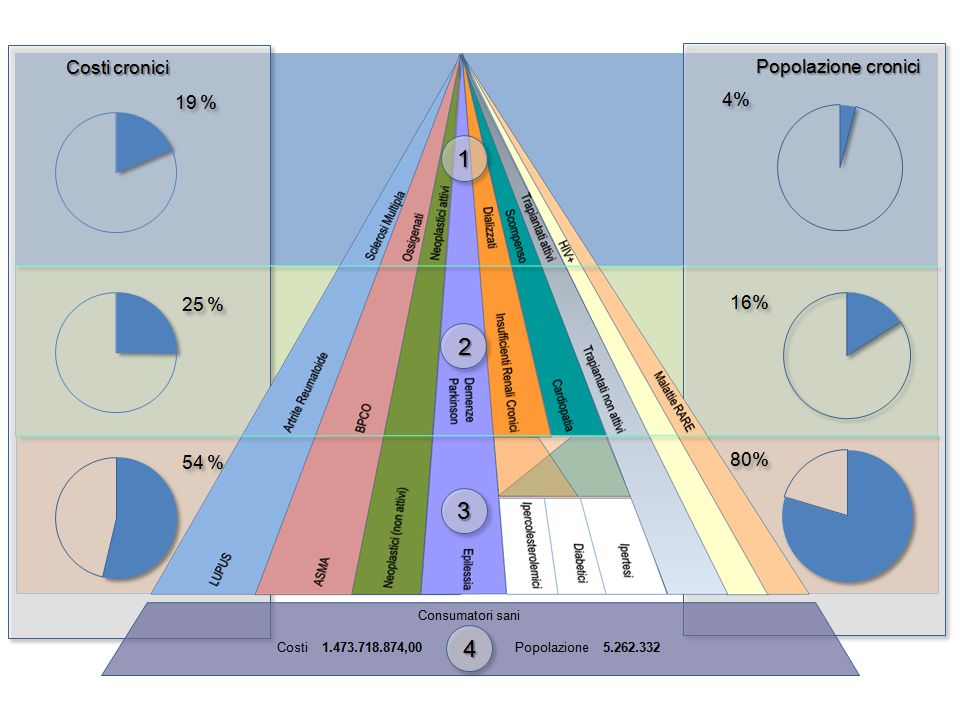
23 1. CReG: how to classify people1. CReG: how to classify people –The classification scheme produced a huge number of classes –Ranking of the diseases (according to expenditures), and selection of the first two –A manageable number of CReGs (some hundreds) 2. CReG: treatment plans2. CReG: treatment plans –They identify needs for specific diseases –Experts collected and discussed treatment plans and guidelines CReG: the pillars DG SANITA
, and selection of the first two –A manageable number of CReGs (some hundreds) 2. CReG: treatment plans2. CReG: treatment plans –They identify needs for specific diseases –Experts collected and discussed treatment plans and guidelines CReG: the pillars DG SANITA.")
24
24 3. CReG: a reimbursement scheme3. CReG: a reimbursement scheme –To reimburse a global treatment plan (like DRG), not individual activities (like drugs, visits, examinations, …) –Two methodological questions: How to set a tariffHow to set a tariff How to manage reimbursement from the administrative point of viewHow to manage reimbursement from the administrative point of view –How to consider complexity (more than two diseases in the same patient) For each CReG: number of diseasesFor each CReG: number of diseases Linearity in expenditures according to complexityLinearity in expenditures according to complexity CReG: the pillars DG SANITA
, not individual activities (like drugs, visits, examinations, …) –Two methodological questions: How to set a tariffHow to set a tariff How to manage reimbursement from the administrative point of viewHow to manage reimbursement from the administrative point of view –How to consider complexity (more than two diseases in the same patient) For each CReG: number of diseasesFor each CReG: number of diseases Linearity in expenditures according to complexityLinearity in expenditures according to complexity CReG: the pillars DG SANITA.")
25
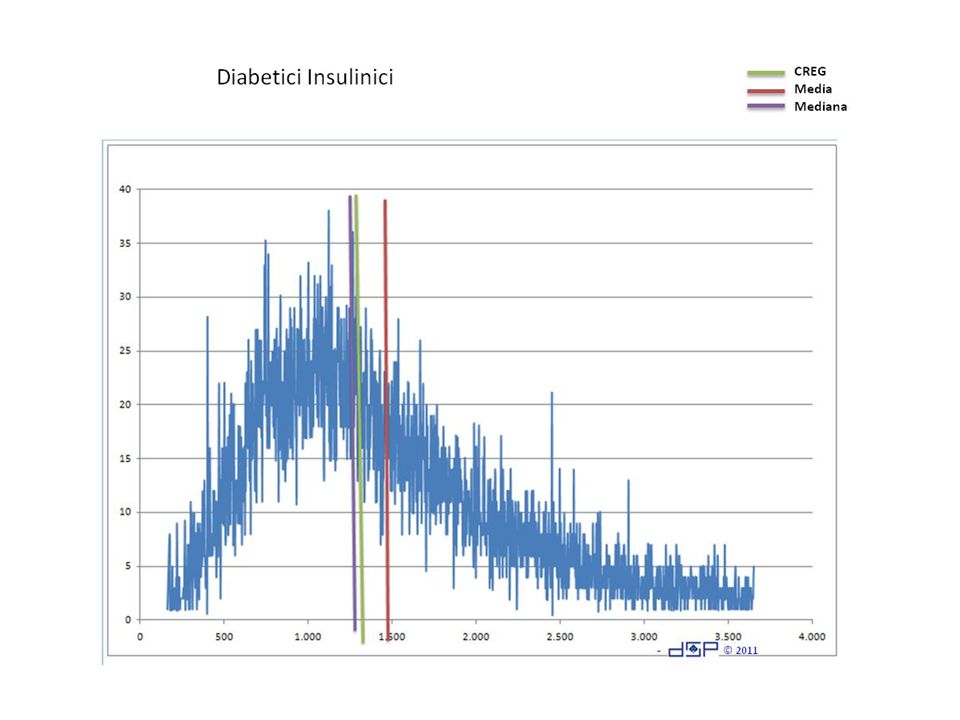
Examples of linearity of expenditures According to complexity

28
CREG Media Mediana Ipertesi

30
30 3. CReG: a reimbursement scheme3. CReG: a reimbursement scheme –150 different CReGs –A basic tariff for each CReG –An incremental tariff for each additional disease –Examples CReG: the pillars DG SANITA

31
CReGBasic Tariff Incremen tal Tariff Chronic kidney insuff. with dialisis, hypertension34.7021.356 Chronic kidney insuff. without dialisis, hypertension 1.6661.049 Chronic kidney insuff. without dialisis, gastro&liver1.149375 Hypercholesterol, hypertension1.014530 Hypercolesterol, asthma1.391534 Insulinic diabetes, transplant (inactiv)5.252389 Diabetes, Parkinson2.504289 COPD, cardio-vasculopatic2.262579 Asthma, diabetes1.588235 Cardio-vasculopatic, systemic Lupus heritematosus 1.477650 Hypertension, rheumatoid arthritis1.003566
 Diabetes, Parkinson COPD, cardio-vasculopatic Asthma, diabetes Cardio-vasculopatic, systemic Lupus heritematosus Hypertension, rheumatoid arthritis")
32
32 4. CReG: the organizational platform4. CReG: the organizational platform –A new institutional subject A group of GPsA group of GPs Association of patients, or professionalsAssociation of patients, or professionals Any type of provider (hospitals, ambulatories, …) private or publicAny type of provider (hospitals, ambulatories, …) private or public Must be accredited (establish criteria and rules)Must be accredited (establish criteria and rules) Must sign a contract with ASLMust sign a contract with ASL –Patients will receive a defined set of activities (treatment plan) CReG: the organizational platform DG SANITA
 private or publicAny type of provider (hospitals, ambulatories, …) private or public Must be accredited (establish criteria and rules)Must be accredited (establish criteria and rules) Must sign a contract with ASLMust sign a contract with ASL –Patients will receive a defined set of activities (treatment plan) CReG: the organizational platform DG SANITA.")
33
33 4. CReG: the organizational platform4. CReG: the organizational platform –Accreditation: Organizational and managerial attributesOrganizational and managerial attributes Professional skills (clinical expertise)Professional skills (clinical expertise) Information systemInformation system … … …… … … –Contract: Duties for the institutional subjectDuties for the institutional subject –Patients interested, expected needs, treatment plans, managerial activities, information exchanged Duties for the ASLDuties for the ASL –Reimbursement scheme, control activities CReG: the organizational platform DG SANITA
Professional skills (clinical expertise) Information systemInformation system … … …… … … –Contract: Duties for the institutional subjectDuties for the institutional subject –Patients interested, expected needs, treatment plans, managerial activities, information exchanged Duties for the ASLDuties for the ASL –Reimbursement scheme, control activities CReG: the organizational platform DG SANITA.")
34
34 Next months:Next months: –A restricted application of CReG approach –In five areas: Bergamo, Como, Lecco, Melegnano, MilanoBergamo, Como, Lecco, Melegnano, Milano –For some diseases: Diabetes, hypertension, COPD, kidney insufficiency, …Diabetes, hypertension, COPD, kidney insufficiency, … –Objectives: To fine tune the CReG approachTo fine tune the CReG approach Particularly: organizational, managerial, administrative aspectsParticularly: organizational, managerial, administrative aspects … and just for closing … DG SANITA

35
Thank you forattentionandpatience Marc Chagall: The Violinist DG. SANITA Carlo Zocchetti

Similar presentations