Download presentation
Presentation is loading. Please wait.

1
HHHoldorf

4
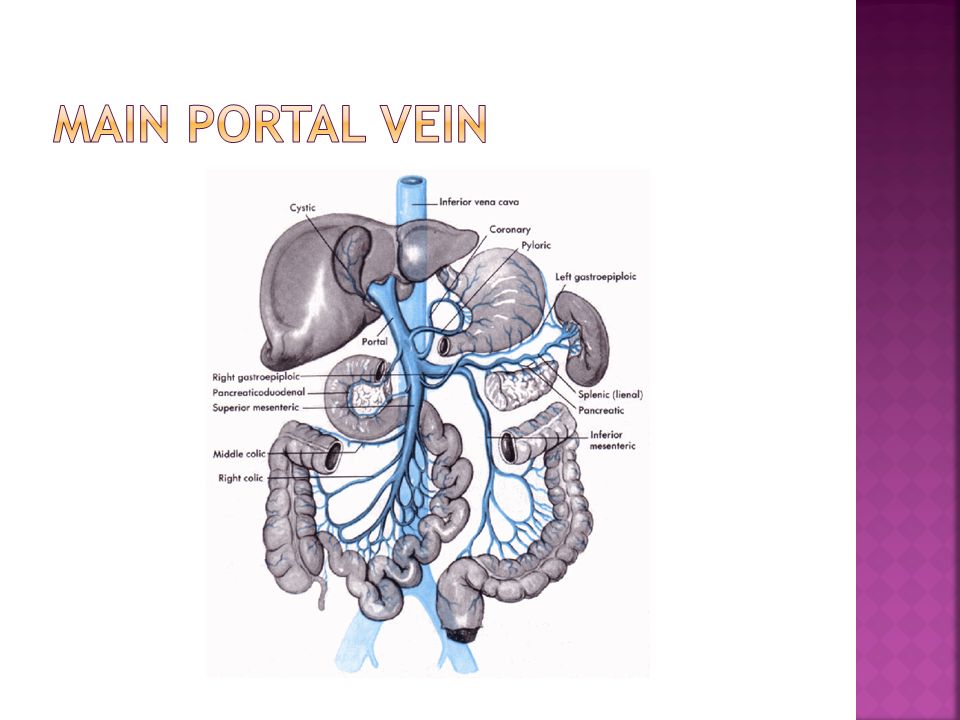
Portal Vein: Collects blood from the digestive tract and empties into the liver and is formed by the junction of the splenic vein and the superior mesenteric vein. A large left branch supplies the left lobe of the liver. The right portal vein has a major branch coming off just superior to the gallbladder. Portal veins have echogenic borders and branch away from the porta hepatic.

6
Portal veins have echogenic borders Portal veins converge at the portal hepatis Portal veins demonstrate hepato-petal blood flow Hepatic Veins do not have echogenic borders Hepatic Veins converge at the IVC Hepatic Veins demonstrate hepto-fugal blood flow.

7
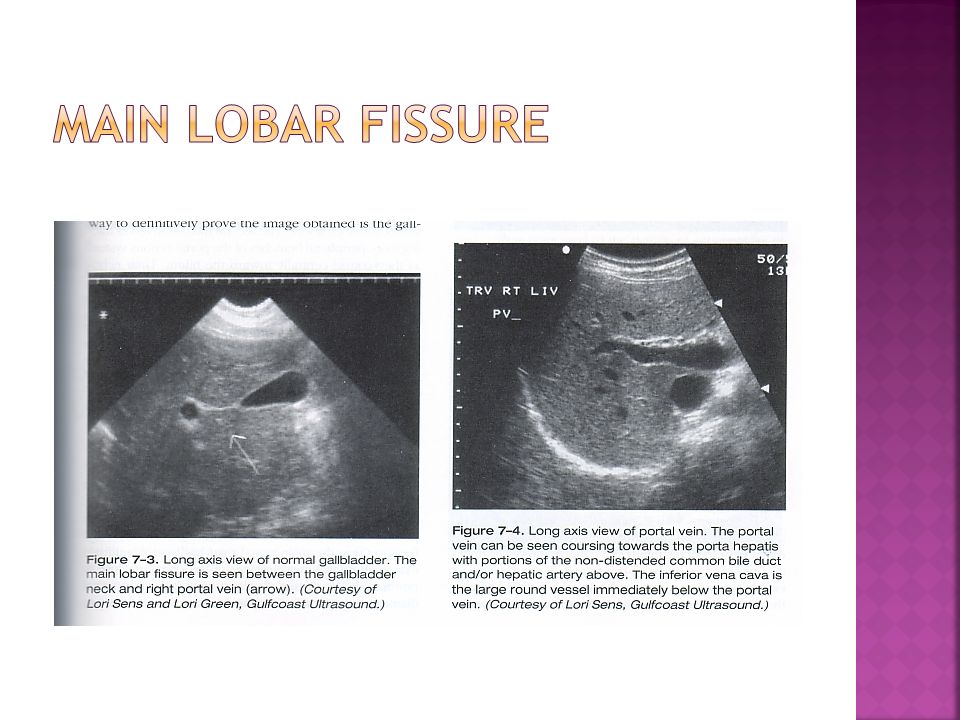
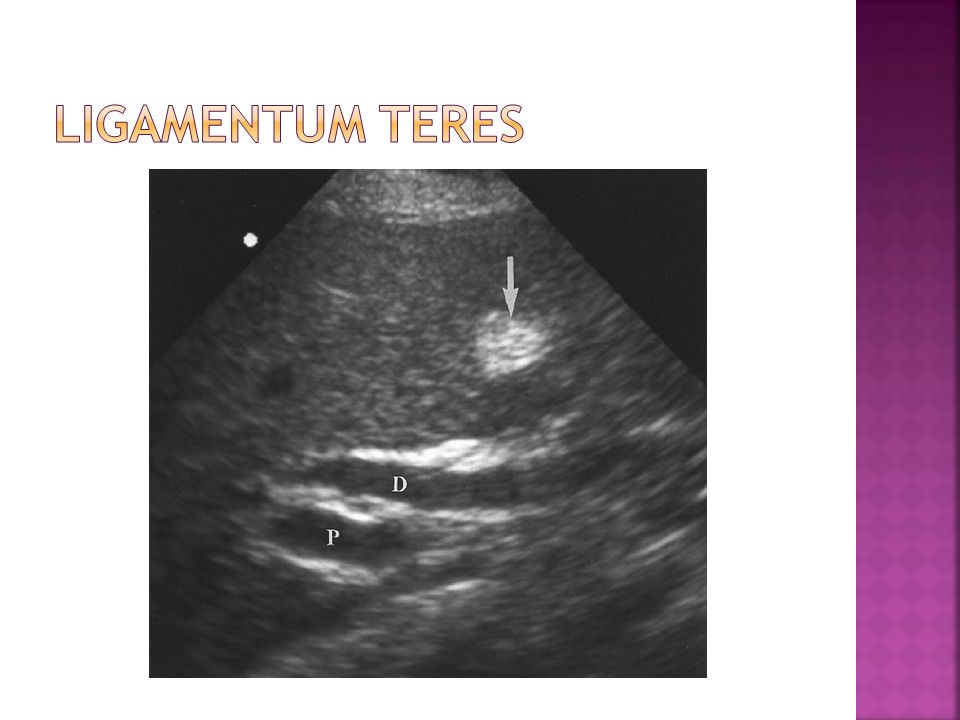
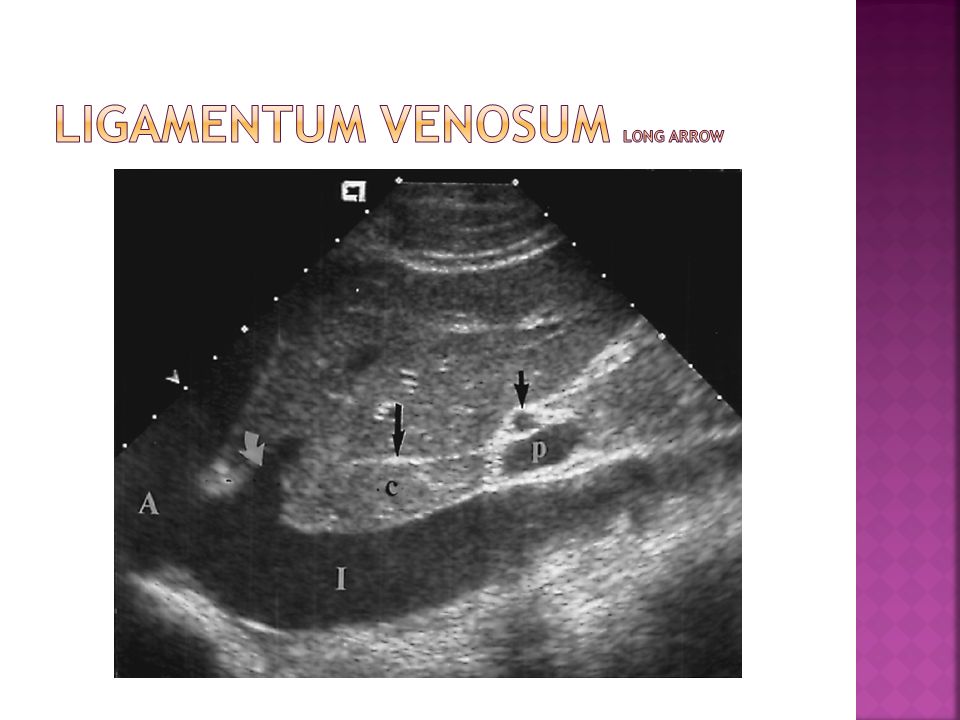
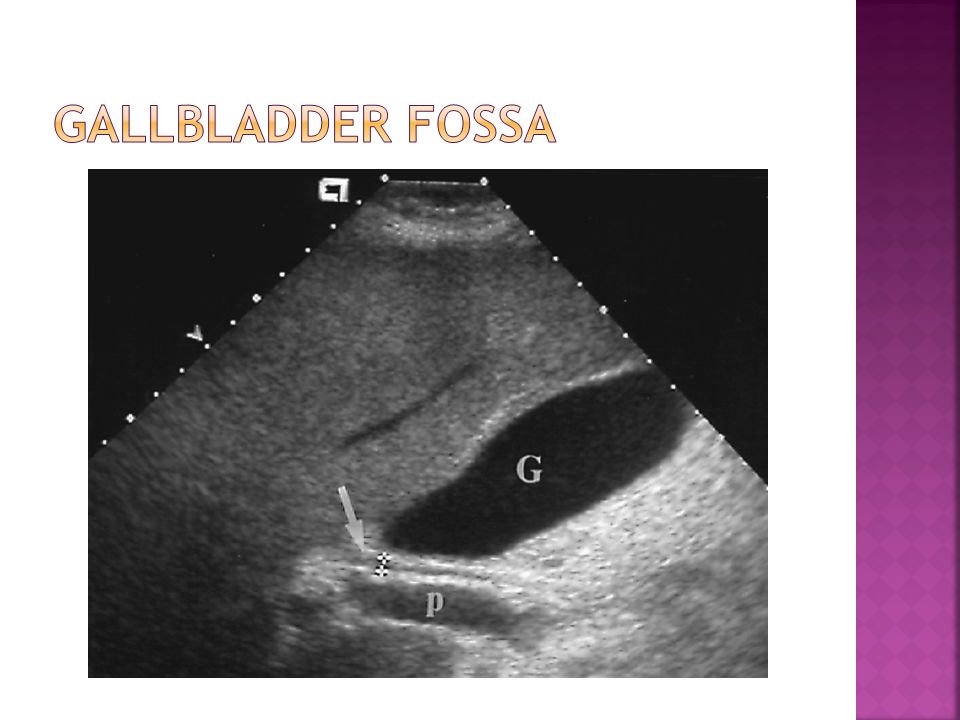
Main lobar fissure: Fissure between the right and left lobes of the liver: seen only between the gallbladder and the right portal vein. Ligamentum Teres: Echogenic structure in the left lobe of the liver (a remnant of the ductus venosum) in which the umbilical vein runs. Ligamentum venosum: Echogenic line anterior to the caudate lobe of the liver.
 in which the umbilical vein runs. Ligamentum venosum: Echogenic line anterior to the caudate lobe of the liver..")
10
The ligamentum teres represents the inferior end of the separation between the medical and laterals segments of the left lobe. A.K.A. The Round Ligament The round ligament represents the remnant of the fetal umbilical vein. For a month or two after birth, the umbilical vein is patent, subsequently degenerating to fibrous tissue, the round ligament.

12
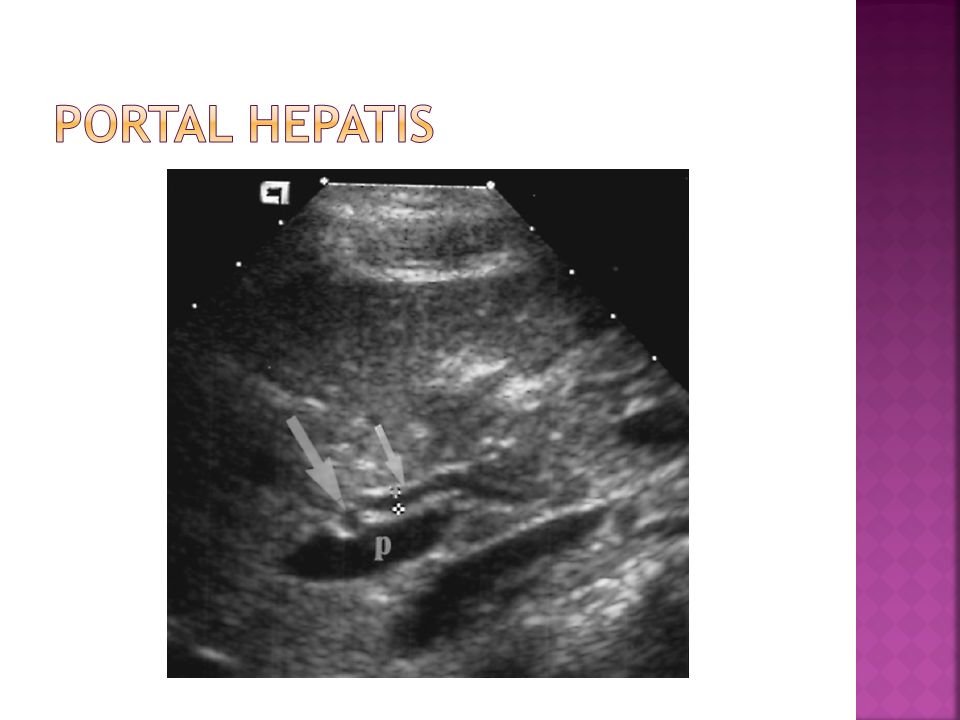
Porta Hepatis: Echogenic region surrounding the portal veins, hepatic artery, and common bile duct where all these structures enter the liver.

14
The hepatic veins represent the divisions between the lobes and segments of the liver. The middle hepatic vein divides the right and left lobes of the liver. The left hepatic vein separates the medical and lateral segments of the left lobe: the right hepatic vein separates the anterior and posterior segments of the right lobe of the liver.

16
The gallbladder represents the inferior end of the separation between right and left lobes of the liver.

18
Technique A real-time scanner with a small foot print and a wide field of view is generally the preferred equipment. This enables easy sub costal and intercostal scanning. As the liver is a large organ, the optimal transducer should provide focusing from near to far field.

19
The patient is generally placed in the supine or left lateral decubitus position. The transducer is placed in a sub costal location. Intercostal scanning may be necessary if the patient is too full of gas or if the liver is small and too high for adequate sub costal scanning. Scans are generally done in longitudinal, transverse, and oblique planes. The best images of the diaphragmatic portion of the liver are usually obtained from a sub costal location with deep, suspended inspirations.

20
Fasting? Check departmental protocols.

21
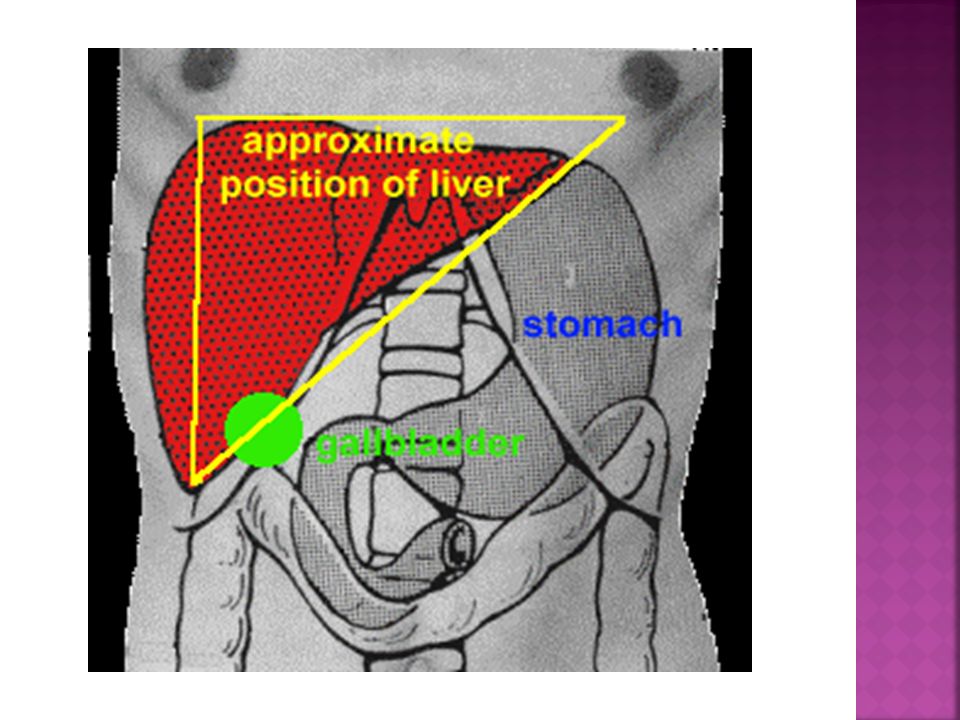
The liver is located in the upper abdomen adjacent to the diaphragm. The bulk of the liver is located in the RUQ and in most patients part of the left love extends into the LUQ. The liver is displaced inferiorly with inspiration. Except for several ligament attachments, there is a large potential space for the accumulation of fluids between the liver and diaphragm known as the right and left subphrenic or sub-diaphragmatic spaces.

22
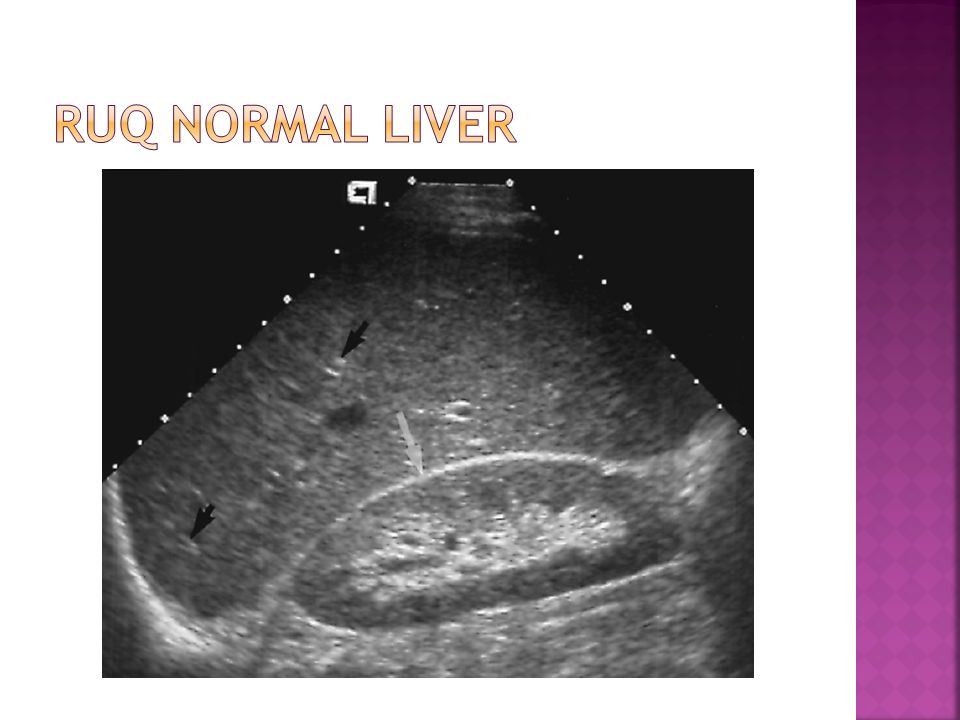
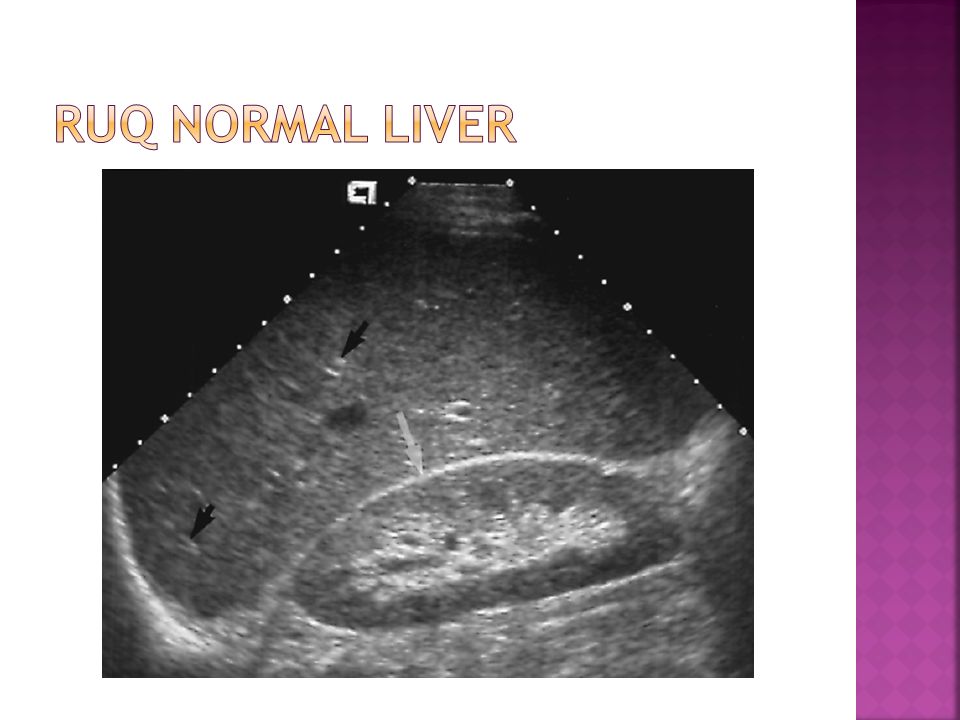
The normal liver should have a homogenous parenchymal echo texture. The normal echo brightness should be equal or slightly greater than the renal cortex and slightly less than the spleen.

23
The size and shape of the normal liver is quite variable making it difficult to assess with real-time scanning whether it is of appropriate size, too small (atrophic), or too large (Hepatomegaly). In the right mid- clavicular line, the cranio-caudal dimension of the normal adult liver should be in the range or 10.5 cm (+/- 1.5 cm) with 13 cm considered a highly reliable cut-off for normal livers. An explanation should be sought if it measures more or less than this.
 with 13 cm considered a highly reliable cut-off for normal livers. An explanation should be sought if it measures more or less than this..")
25
The surface of the liver is smooth and covered by a fibrous capsule known as Glisson’s capsule. Trauma to the liver without laceration to Glisson’s capsule may be seen as a localized subcapsular fluid collection. The liver is impressed by the right kidney, gallbladder, colon and stomach. The actual position of these organs relative to the liver is quite variable. For example: the right kidney may be positioned high and be completely draped anteriorly by liver or it may be low an only be partially covered by liver.

26
The major hepatic and portal veins should be easily seen in the normal liver. The hepatic veins are most prominent closest to the diaphragm. The right, middle, and left Hepatic Veins converge to enter the IVC. The Hepatic Veins have thin, smooth walls which only produce a bright echo when the sound beam is perpendicular to the vessel surface. Portal Veins are largest near the porta hepatis and decrease in size as they subdivide and extend toward the periphery. Each PV courses with a fibrous channel with a hepatic artery and bile duct.

27
KEY POINTS Collectively, three vessels from the PORTAL TRIAD: Hepatic Artery, Biliary Radical, and Portal Vein. A fibrous channel accounts for the thick bright wall seen around the PV. The HVs and PVs are both affected by respiration although the affect is most pronounced in the HVs.

Similar presentations