Download presentation
Presentation is loading. Please wait.

1
Dallas 2015 TFQO: Koen Monsieurs 372 EVREV 1: Koen Monsieurs 372 EVREV 2: Ahamed Idris 349 Taskforce: BLS BLS366 Chest Compression Depth (adults)
")
2
Dallas 2015 COI Disclosure (SPECIFIC to this systematic review) EVREV 1 COI 358 Commercial/industry Research grant from the Laerdal Foundation Potential intellectual conflicts Editor Guidelines 2015, ERC EVREV 2 COI 302 Commercial/industry None Potential intellectual conflicts Co-author of one study on depth
 EVREV 1 COI 358 Commercial/industry Research grant from the Laerdal Foundation Potential intellectual conflicts Editor Guidelines 2015, ERC EVREV 2 COI 302 Commercial/industry None Potential intellectual conflicts Co-author of one study on depth")
3
Dallas 2015 2010 Treatment Recommendation It is reasonable to compress the sternum at least 2 inches/5 cm for all adult cardiac arrest victims. There is insufficient evidence to recommend a specific upper limit for chest compression depth.

4
Dallas 2015 C2015 PICO Population: Among adults who are in cardiac arrest in any setting Intervention: does a different chest compression depth during CPR Comparison: compared with a chest compression depth of at least 5 cm (2 inches) Outcomes: change Survival with favorable neurological/functional outcome at discharge, 30 days, 60 days, 180 days AND/OR 1 year Survival only at discharge, 30 days, 60 days, 180 days AND/OR 1 year ROSC
 Outcomes: change Survival with favorable neurological/functional outcome at discharge, 30 days, 60 days, 180 days AND/OR 1 year Survival only at discharge, 30 days, 60 days, 180 days AND/OR 1 year ROSC")
5
Dallas 2015 Inclusion/Exclusion & Articles Found Included: all human, comparative studies (prospective and retrospective). Excluded: unpublished studies and studies only published as abstract paediatric studies, manikin studies, animal studies studies that did not specifically address the PICO question. 2486 Articles initially identified, 10 included in Evidence Profile tables RCTs: 0 Non-RCTs: 9 Non-RCT addressing injury associated with depth: 1

6
Dallas 2015 2015 Proposed Treatment Recommendation Draft Treatment Recommendation: We recommend a chest compression depth range of 4.5 cm to 5.5 cm during manual CPR in adults with cardiac arrest (strong recommendation based on moderate quality evidence).
.")
7
Dallas 2015 Risk of Bias in Non-RCTs

8
Dallas 2015 Evidence Profile Table

9
Dallas 2015 Footnotes to Evidence Table Favorable neurological outcome: Upgraded for dose – response effect. Vadeboncoeur 2014,182 – downgraded for imprecision. 175 (30%) missing data, but imputed into analysis. Did not provide a comparison of characteristics of patients with missing data vs. those with data. Hostler 2011,1512: very serious indirectness. Primary outcome was comparison of feedback vs. no feedback. Depth was an indirect comparison in terms of outcomes. Survival to hospital discharge: Upgraded for dose – response effect. Vadeboncoeur 2014,182; Hostler 2011,1512 – same as above. Stiell 2012,1192; Stiell 2014,1962 – no serious downgrades. ROSC: Upgraded for dose – response effect. Babbs 2008,306 – serious bias for exposure, indirectness, imprecision (T-ROSC is a surrogate for ROSC) Bohn 2011,257 – serious bias for exposure (post hoc analysis), confounding (analysis not adjusted) Edelson 2006,137 - very serious indirectness (outcome was first shock success, not ROSC) Edelson 2008,1063– serious bias (no adjustment), very serious indirectness (analysis included multiple variables and did not isolate the effect of depth) Hostler 2011,1512 – same as above Kramer-Johansen 2006,283 – serious bias (no comparison of excluded (21%) vs. included patients), depth was post-hoc analysis Stiell 2012,1192; Stiell 2014,1962 – no serious downgrades.
 missing data, but imputed into analysis. Did not provide a comparison of characteristics of patients with missing data vs. those with data. Hostler 2011,1512: very serious indirectness. Primary outcome was comparison of feedback vs. no feedback. Depth was an indirect comparison in terms of outcomes. Survival to hospital discharge: Upgraded for dose – response effect. Vadeboncoeur 2014,182; Hostler 2011,1512 – same as above. Stiell 2012,1192; Stiell 2014,1962 – no serious downgrades. ROSC: Upgraded for dose – response effect. Babbs 2008,306 – serious bias for exposure, indirectness, imprecision (T-ROSC is a surrogate for ROSC) Bohn 2011,257 – serious bias for exposure (post hoc analysis), confounding (analysis not adjusted) Edelson 2006,137 - very serious indirectness (outcome was first shock success, not ROSC) Edelson 2008,1063– serious bias (no adjustment), very serious indirectness (analysis included multiple variables and did not isolate the effect of depth) Hostler 2011,1512 – same as above Kramer-Johansen 2006,283 – serious bias (no comparison of excluded (21%) vs. included patients), depth was post-hoc analysis Stiell 2012,1192; Stiell 2014,1962 – no serious downgrades..")
10
Dallas 2015 Proposed Consensus on Science Statements For the critical outcome “survival with good neurological outcome”, we found very low quality evidence from two observational studies [Vadeboncoeur 2014,182] [Hostler 2011,1512] suggesting that a compression depth in adults of more than 5 cm is better than all other compression depths during manual CPR. Evidence was downgraded for serious bias, imprecision, and indirectness. [Vadeboncoeur 2014,182: Neurological outcome, percent of compressions ≥ 51 mm, adjusted odds ratio 1.21 (CI 1.00 – 1.46) N=593, 175 missing data, which was imputed]
![Dallas 2015 Proposed Consensus on Science Statements For the critical outcome survival with good neurological outcome , we found very low quality evidence from two observational studies [Vadeboncoeur 2014,182] [Hostler 2011,1512] suggesting that a compression depth in adults of more than 5 cm is better than all other compression depths during manual CPR.](http://images.slideplayer.com/31/9698148/slides/slide_10.jpg "Evidence was downgraded for serious bias, imprecision, and indirectness. [Vadeboncoeur 2014,182: Neurological outcome, percent of compressions ≥ 51 mm, adjusted odds ratio 1.21 (CI 1.00 – 1.46) N=593, 175 missing data, which was imputed].")
11
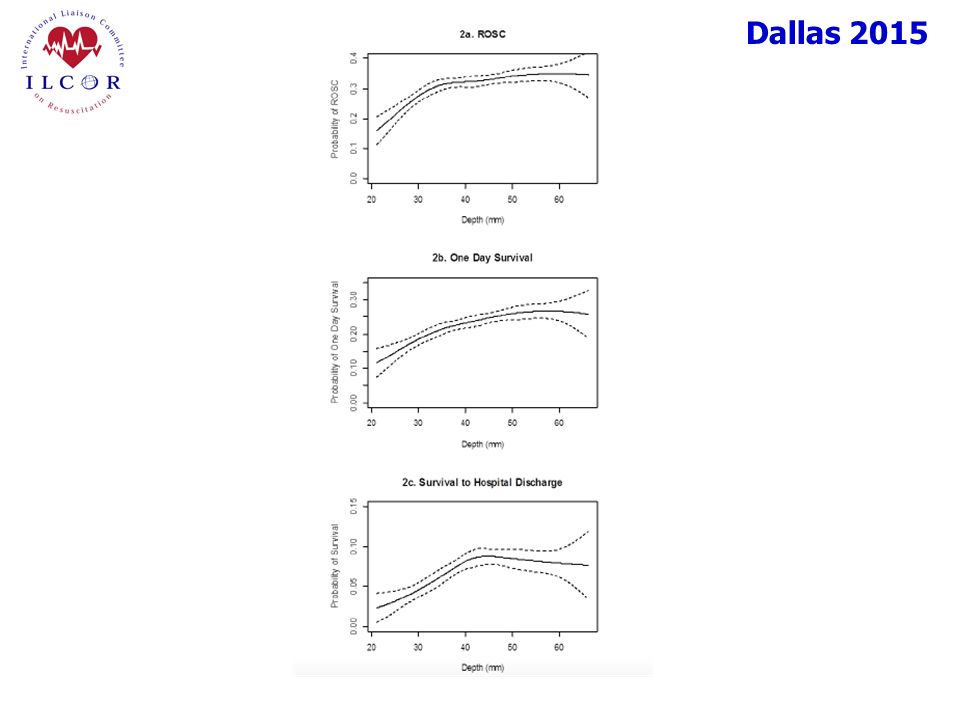
Dallas 2015 Proposed Consensus on Science Statements (Cont.) For the critical outcome “survival to hospital discharge”, we found moderate quality evidence from four observational studies [Vadeboncoeur 2014,182] [Hostler 2011,1512] [Stiell 2012,1192] [Stiell 2014,1962] suggesting that a compression depth range of 4.5 to 5.5 cm in adults is better than all other compression depths during manual CPR. Evidence was upgraded for a dose-response relationship; the two largest studies had no serious bias. [Stiell 2014,1962: Survival, N=9,136, adjusted cubic spline, optimal depth range 40 to 55 mm, peak at 46 mm]
![Dallas 2015 Proposed Consensus on Science Statements (Cont.) For the critical outcome survival to hospital discharge , we found moderate quality evidence from four observational studies [Vadeboncoeur 2014,182] [Hostler 2011,1512] [Stiell 2012,1192] [Stiell 2014,1962] suggesting that a compression depth range of 4.5 to 5.5 cm in adults is better than all other compression depths during manual CPR.](http://images.slideplayer.com/31/9698148/slides/slide_11.jpg "Evidence was upgraded for a dose-response relationship; the two largest studies had no serious bias. [Stiell 2014,1962: Survival, N=9,136, adjusted cubic spline, optimal depth range 40 to 55 mm, peak at 46 mm].")
12
Dallas 2015 Proposed Consensus on Science Statements (cont.) For the critical outcome “ROSC”, we found moderate quality evidence from eight observational studies [Babbs 2008,306] [Bohn 2011,257] [Edelson 2006,137] [Edelson 2008,1063] [Hostler 2011,1512] [Kramer-Johansen 2006,283] [Stiell 2012,1192] [Stiell 2014,1962] suggesting that a compression depth of more than 5 cm (range 4.5 to 5.5 cm) in adults is better than all other compression depths during manual CPR. Evidence was upgraded for a dose - response relationship; the two largest studies had no serious bias. [Stiell 2014,1962: N=9,136, ROSC, depth 38 – 51 mm, adjusted OR 0.86 (CI 0.75 – 0.97), reference ≥51 mm] [Note: this study supports >5 cm for ROSC]
![Dallas 2015 Proposed Consensus on Science Statements (cont.) For the critical outcome ROSC , we found moderate quality evidence from eight observational studies [Babbs 2008,306] [Bohn 2011,257] [Edelson 2006,137] [Edelson 2008,1063] [Hostler 2011,1512] [Kramer-Johansen 2006,283] [Stiell 2012,1192] [Stiell 2014,1962] suggesting that a compression depth of more than 5 cm (range 4.5 to 5.5 cm) in adults is better than all other compression depths during manual CPR.](http://images.slideplayer.com/31/9698148/slides/slide_12.jpg "Evidence was upgraded for a dose - response relationship; the two largest studies had no serious bias. [Stiell 2014,1962: N=9,136, ROSC, depth 38 – 51 mm, adjusted OR 0.86 (CI 0.75 – 0.97), reference ≥51 mm] [Note: this study supports >5 cm for ROSC].")
13
Dallas 2015 For the important outcome “injury”, we found very low quality evidence from one observational study [Hellevuo 2013,760] suggesting that a compression depth of more than 6 cm is associated with an increased rate of injury in adults when compared with compression depths of 5 to 6 cm during manual CPR. Evidence was downgraded for serious risk of bias (confounding), imprecision, and very serious indirectness. N=170 (total 353, 183 excluded for incomplete data). With compression depth >6 cm, 63% had injuries; depth 6 cm were 28%, 27%, and 49% respectively. Proposed Consensus on Science Statements (cont.)
![Dallas 2015 For the important outcome injury , we found very low quality evidence from one observational study [Hellevuo 2013,760] suggesting that a compression depth of more than 6 cm is associated with an increased rate of injury in adults when compared with compression depths of 5 to 6 cm during manual CPR.](http://images.slideplayer.com/31/9698148/slides/slide_13.jpg "Evidence was downgraded for serious risk of bias (confounding), imprecision, and very serious indirectness. N=170 (total 353, 183 excluded for incomplete data). With compression depth >6 cm, 63% had injuries; depth 6 cm were 28%, 27%, and 49% respectively. Proposed Consensus on Science Statements (cont.).")
14
Dallas 2015 Draft Treatment Recommendations Draft Treatment Recommendation: We recommend a chest compression depth range of 4.5 cm to 5.5 cm during manual CPR in adults with cardiac arrest (strong recommendation based on moderate quality evidence). Values and preferences statement In making this recommendation, we placed importance on adequate compression depth. We put an upper limit on compression depth in adults because no additional outcome benefit was demonstrated with compression depths of more than 6 cm and because of the possibility of increased rate of injury. We considered the additional training cost to be minimal. The cost to adjust limits in compression depth feedback devices would be modest.

15
Dallas 2015

Similar presentations








 EVREV 1: Gene Ong (#COI = 118) EVREV 2: Jos Bruinenberg (#COI = 19) Taskforce: Pediatric Taskforce The Long.>")




 Director of Evidence-Based Practice, Quality Management Assistant.>")







