Download presentation
Presentation is loading. Please wait.

1
Overactive Bladder Jerry G. Blaivas, MD Clinical Professor of Urology Weil Cornell Medical College New York Presbyterian Hospital Adjunct Professor of Urology SUNY-Downstate Medical Center

2
Prevalence of OAB (USA) OAB (33.3 million) 17% of adults Hampel, Urologe A 2003;42:776; Stewart, World J Urol 2003;20:327; http://www.census.gov/cgi-bin/ipc/idbrank.pl
 OAB (33.3 million) 17% of adults Hampel, Urologe A 2003;42:776; Stewart, World J Urol 2003;20:327;")
3
Prevalence of OAB (USA) Wet versus Dry 37% Wet (12 million) 63% Dry (21 million) OAB Hampel, Urologe A 2003;42:776; Stewart, World J Urol, 2003;20:327; http://www.census.gov/cgi-bin/ipc/idbrank.pl
 Wet versus Dry 37% Wet (12 million) 63% Dry (21 million) OAB Hampel, Urologe A 2003;42:776; Stewart, World J Urol, 2003;20:327;")
4
Prevalence of OAB by Age Stewart, World J Urol, 2003;20:327

5
Prevalence of OAB Compared to Other Chronic Conditions http://www.cdc.gov/nchs/fastats/default.htmhttp://www.cdc.gov/nchs/fastats/default.htm; http://www.diabetes.org/diabetes-basics/diabetes; Hu T, et al. Urology. 2004;63(3):461-465. http://www.diabetes.org/diabetes-basics/diabetes
:")
6
Falls and Fractures Brown et al. JAGS. 2000;48(7): 721-725. Increased Risk (%) 26% 34% Falls Fractures 40 30 20 10 0
 26% 34% Falls Fractures")
7
7 7 Impact of Urinary Incontinence on Quality of Life Quality of Life Physical Limitations or cessation of physical activities Sexual Avoidance of sexual contact and intimacy Occupational Absence from work Decreased productivity Social Reduction in social interaction Alteration of travel plans Increased risk of institutionalization of frail older persons Domestic Requirements for specialized underwear, bedding Special precautions with clothing Psychological Guilt/depression Loss of self-respect and dignity Fear of: Being a burden Lack of bladder control Urine odor Apathy/denial

8
Overactive Bladder: “urgency, with or without urge incontinence usually with frequency and nocturia…if there is no proven infection or other pathology” ICS, 2002

9
Urgency ICS, 2002 “...a sudden compelling desire urge to pass urine, which is difficult to defer.”

10
Urgency is not an all-or-none phenomena; it can be graded Urgency should be redefined: –“...a sudden compelling desire urge to pass urine, which is difficult to defer.” There are at least two types of urgency OAB: A New Paradigm

11
OAB is a symptom complex, not a syndrome OAB has a differential diagnosis OAB can be classified by urodynamics A New OAB Paradigm

12
Types of Urgency Type 1 - An intensification of the normal urge to void (69%) Type 2 - A sudden urge that is a different sensation (31%) Some patients report a constant feeling of the need to void – not really urgency May have different etiologies May respond differently to treatment Blaivas et al, Two Types of Urgency. Neurourol Urodyn. 2009;28(3):188
:188.")
13
Incontinence associated with urgency Urge Incontinence

14
A subtle sensation, gradual in onset, felt in the suprapubic area as fullness or in the penis, vagina or urethra as a tingling If patient waits too long > urgency Normal Urge to Void

15
Type 0 - no urge Type 1 - mild urge (can delay for > 1H) Type 2 - moderate urge (can delay for 10 – 60 minutes) Type 3 - severe urge (can delay for < 10 minutes) Type 4 - precipitous urge (must void immediately) Urgency Perception Grade Blaivas et al, Urgency Perception Score, J Urol, 2007
 Type 2 - moderate urge (can delay for 10 – 60 minutes) Type 3 - severe urge (can delay for < 10 minutes) Type 4 - precipitous urge (must void immediately) Urgency Perception Grade Blaivas et al, Urgency Perception Score, J Urol, 2007")
16
Type 4 - “...a sudden compelling desire to pass urine, which is difficult to defer.” and / or Type 3 - A short warning time between the first and a severe urge and / or Type 2 - Waiting too long Urgency

17
Healthy Volunteers Grade of UrgePer cent 019% 146% 226% 310% 4 0% 65% DeWachter & Wyndaele, Neurourol & Urodynam, 2004

18
Urge gradeNormal*LUTS**OAB*** 08 (10)2 (3)2 (2) 131 (37)22 (36)7 (9) 234 (41)28 (45)36 (45) 36 (7)5 (8)19 (24) 44 (5)5 (8)16 (20) Total836280 *vs** p=0.24 *vs***p<0.001 **vs***p<0.001 Blaivas, J Urol, 2007 44% 47%
2 (3)2 (2) 131 (37)22 (36)7 (9) 234 (41)28 (45)36 (45) 36 (7)5 (8)19 (24) 44 (5)5 (8)16 (20) Total *vs** p=0.24 *vs***p<0.001 **vs***p<0.001 Blaivas, J Urol, % 47%")
19
A ll of these sensations need to be put into context by relating them to bladder volume If a patient experiences all of the UPS sensations of the course of 2 hours & the bladder volume is only 90 ml, that is OAB If she experiences all of the UPS sensations of the course of 2 hours and the bladder volume is 300 ml, the bladder is probably normal The bladder diary is the best method for evaluating sensations related to volume

20
Why did you urinate? (0) Convenience (no urge or desire) (1) Mild urge (can delay urination for an hour) (2) Moderate urge (can delay > 10 but <60 min) (3) Severe urge (can delay for < 10 min) (4) Desperate urge (must go immediately) Incontinence grade. Grade 1 - some drops Grade 2 - moderate loss (wet underpants) Grade 3 - extensive loss (wet outer clothes) OAB Bladder Diary Instructions
 Convenience (no urge or desire) (1) Mild urge (can delay urination for an hour) (2) Moderate urge (can delay > 10 but <60 min) (3) Severe urge (can delay for < 10 min) (4) Desperate urge (must go immediately) Incontinence grade. Grade 1 - some drops Grade 2 - moderate loss (wet underpants) Grade 3 - extensive loss (wet outer clothes) OAB Bladder Diary Instructions.")
21
TimeUPSVolume (ml)Incontinence Grade 6 AM41201 7:303900 8:004901 9:103900 12:3021200 5:501900 8:002600 10:002300 12:0041001 3:0041002 8:402600 6:0041201 OAB Diary
Incontinence Grade 6 AM : : : : : : : : : : : OAB Diary")
22
volume

23
TimeUPSVolume (ml)Incontinence Grade 6 AM46600 7:302 900 8:0021200 8:4023600 9:1022400 12:3021800 2:450900 5:5036000 8:0033600 10:0022400 3:0023600 6:0035400 OAB Diary
Incontinence Grade 6 AM : : : : : : : : : : : OAB Diary")
24
volume

25
TimeUPSVolume (ml)Incontinence Grade 6 AM42000 8:3031800 11:0032401 1:0032301 3:2022000 6:0021800 10:0021800 12:45 01800 1:3022400 3:00 22200 5:0022001 6:0012000 OAB Diary
Incontinence Grade 6 AM : : : : : : : : : : : OAB Diary")
26
volume

27
Guan et al, Euro Urol, 2011

28
volume

29
Overactive Bladder: Symptom Complex or Syndrome? “urgency, with or without urge incontinence usually with frequency and nocturia…if there is no proven infection or other pathology” ICS, 2002

30
Clinical Presentation of OAB Lower urinary tract symptoms (LUTS) – the physician elicits OAB symptoms “I have OAB” – the patient self diagnoses The physician probes a reluctant patient who admits she has OAB symptoms
 – the physician elicits OAB symptoms I have OAB – the patient self diagnoses The physician probes a reluctant patient who admits she has OAB symptoms")
31
Differential Diagnosis (non-neurogenic) Urinary tract infection Urethral obstruction: – Pelvic organ prolapse – Post-op – Urethral diverticulum – Stricture – Primary bladder neck
 Urinary tract infection Urethral obstruction: – Pelvic organ prolapse – Post-op – Urethral diverticulum – Stricture – Primary bladder neck")
32
Differential Diagnosis (non-neurogenic) Mixed stress & urge incontinence Foreign body Bladder cancer Bladder stones
 Mixed stress & urge incontinence Foreign body Bladder cancer Bladder stones")
33
Differential Diagnosis (neurogenic) Synergy –Stroke –Parkinson’s –MS (supraspinal) –Spina bifida Dyssynergy –SCI –MS (spinal) –Spina bifida –Other spinal conditions
 Synergy –Stroke –Parkinson’s –MS (supraspinal) –Spina bifida Dyssynergy –SCI –MS (spinal) –Spina bifida –Other spinal conditions")
34
Diagnosis# % Stress incontinence5333% Idiopathic3723% Pelvic organ prolapse3924% Bladder outlet obstruction1610% Miscellaneous149% Neurogenic127% Total171106% Differential Diagnosis in Women

35
Miscellaneous#% Prior pelvic surgery96% Bladder cancer21% Urethral diverticulum21% Vesicovaginal fistula11% Differential Diagnosis in Women

36
Urodynamic Classification During filling: –Type 1 - 4 based on control mechanisms –+ / - low bladder compliance During voiding: –normal Q / p –urethral obstruction –impaired detrusor contractility Flisser, J. Urol 169: 529-534, 2003

37
Urodynamic Classification Type I: symptoms of overactive bladder, no IDC at urodynamics Type II: IDC present; patient is aware and can abort the IDC Type III: IDC patient aware, cannot abort but can temporarily maintain continence by contracting the sphincter Type IV: IDC, no awareness or control Flisser, J. Urol 169: 529-534, 2003

38
OAB Classification Type I: symptoms of overactive bladder, no IDC at urodynamics

39
HMR Voluntary detrusor contraction FSF = 66 ml, FSF = 66 ml 1st urge = 80 ml severe urge = 105 ml Capacity = 346 ml

41
OAB Classification Type I: symptoms of overactive bladder, no IDC at urodynamics Type II: IDC present; patient is aware and can abort the IDC

42
Asked to hold: contracts sphincter Aborts detrusor contraction Involuntary detrusor contraction Prevents incontinence HO

43
OAB Classification Type I: symptoms of overactive bladder, no IDC at urodynamics Type II: IDC present; patient is aware and can abort the IDC Type III: IDC patient aware, cannot abort but can temporarily maintain continence by contracting the sphincter

44
BA Involuntary Contraction Trying to hold incontinent Can’t hold any longer

45
OAB Classification Type I: symptoms of overactive bladder, no IDC at urodynamics Type II: IDC present; patient is aware and can abort the IDC Type III: IDC patient aware, cannot abort but can temporarily maintain continence by contracting the sphincter Type IV: IDC, no awareness or control

46
Voi Rbn IDC Incontinent

47
Type 4 OAB Without Obstruction

48
RS IDC (pdet@Qmax = 12 cm H 2 0) Qmax = 18 ml/S
 Qmax = 18 ml/S")
49
Type 2 OAB Impaired Detrusor Contractility (DHIC)
")
50
AL Involuntary detrusor contractions Sphincter relaxation Incontinent

52
Type 3 OAB Obstruction due to urethral Diverticulum in a woman

53
BG JTJT IDC (detmax = 48 cm H 2 0) Qmax = 1 ml/S Urethral obstruction
 Qmax = 1 ml/S Urethral obstruction")
54
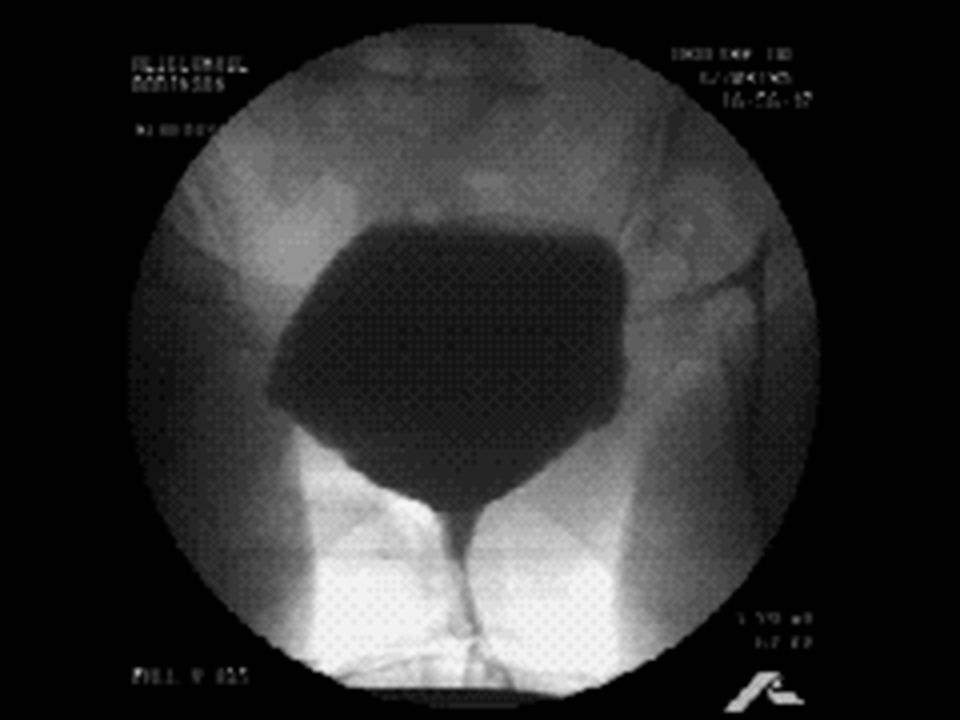
Type 2 OAB Grade 4 prolapse Normal voiding mechanics

55
IC Involuntary detrusor contraction cough

56
IC thigh cystocele bladder catheter

57
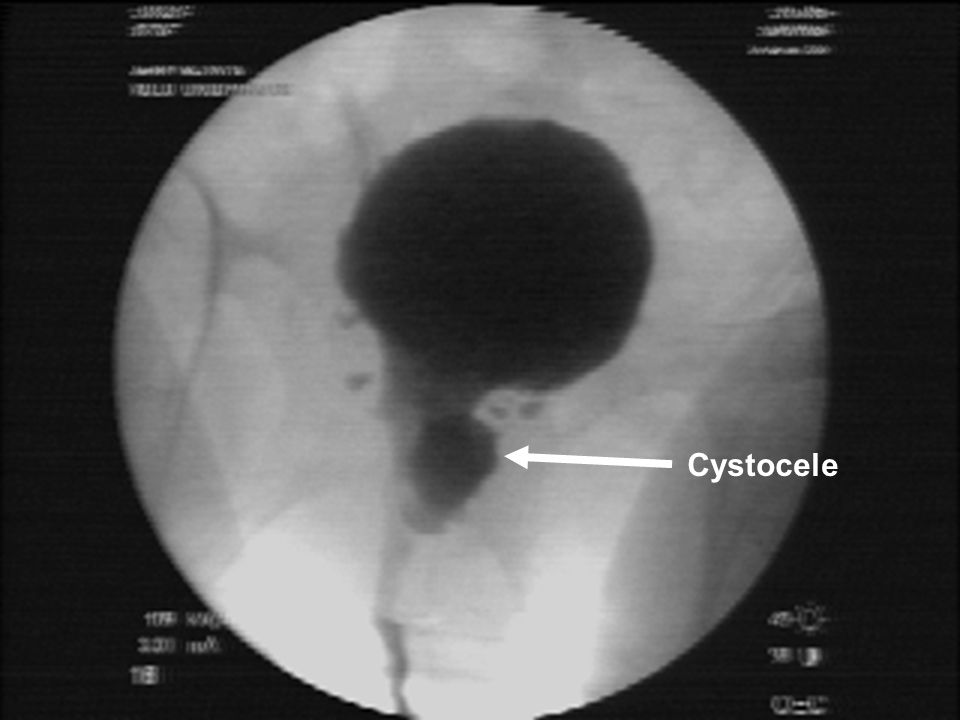
IC cystocele

58
IC Cystocele

59
IC Cystocele

60
IC Cystocele

61
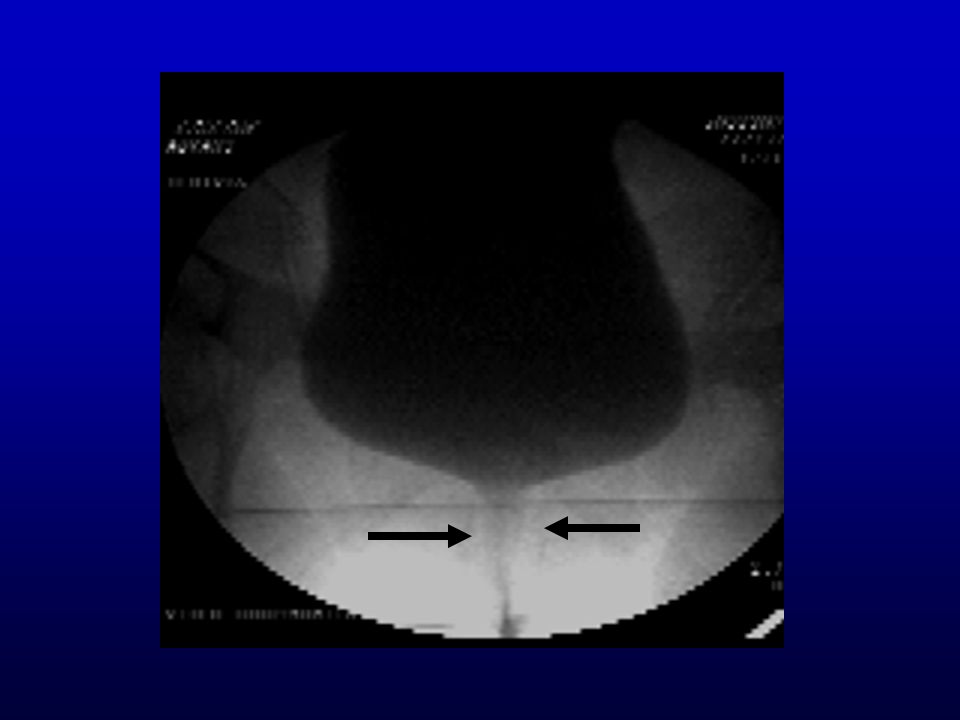
Urethra Urine in vagina Cystocele

63
IC Cystocele

64
IC Cystocele

65
Type 4 OAB Grade 4 prolapse Occult sphincteric incontinence

66
gdl coughs

67
gdl Involuntary detrusor contraction Incontinent

68
gdl VLPP Sphincteric incontinence

69
gdl Voluntary detrusor contraction Normal voiding

70
Type 3 OAB Grade 3 prolapse Grade 1 urethral obstruction

71
FK Involuntary detrusor contraction Incontinent

72
FK Voluntary Low flow

73
Urethral catheter Urethral meatus Bladder capacity cystocele

74
Urethral catheter Urethral meatus Onset of voiding cystocele

75
Qmax urethra

76
Type 4 OAB Impaired Detrusor Contractility

77
AL IDC (pdet@Qmax = 17 cm H 2 0) Qmax = 9 ml/S
 Qmax = 9 ml/S")
78
Type 3 OAB Low Bladder Compliance

79
DS Steep rise in pressure IDC V-U reflux

80
Type 4 OAB Neurogenic Detrusor Overactivity Detrusor sphincter dyssynergia (DESD)
")
81
PS Involuntary detrusor contraction Involuntary sphincter contraction Obstruction due to sphincter contraction

82
Type 1 OAB Painful bladder syndrome Acontractile detrusor

83
Command to void HMR FSF = 66 ml, FSF = 25 ml 1st urge = 50 ml severe urge = 80 ml Capacity = 105 ml

84
Type 4 OAB Without Obstruction Bladder cancer

85
Involuntary detrusor contraction Incontinent Filling defects

86
So, how does cystoscopy help?

87
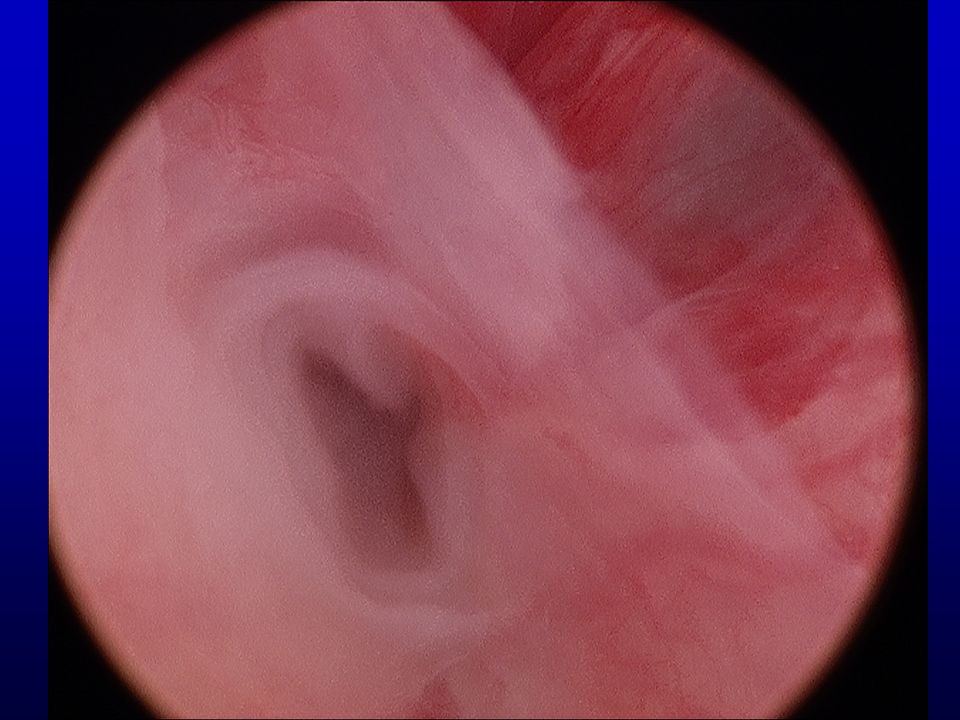
Bladder Neck Contracture

89
Fibroadenomatous Urethral Polyp

90
`

91
Urethral Erosion of Synthetic Sling

92
Bladder neck Eroded mesh

93
Bladder Erosion of Synthetic

94
Strands of eroded mesh

95
Urethral Diverticulum

96
distal mid proximalbladder neck ostia

97
Urethral Stricture

99
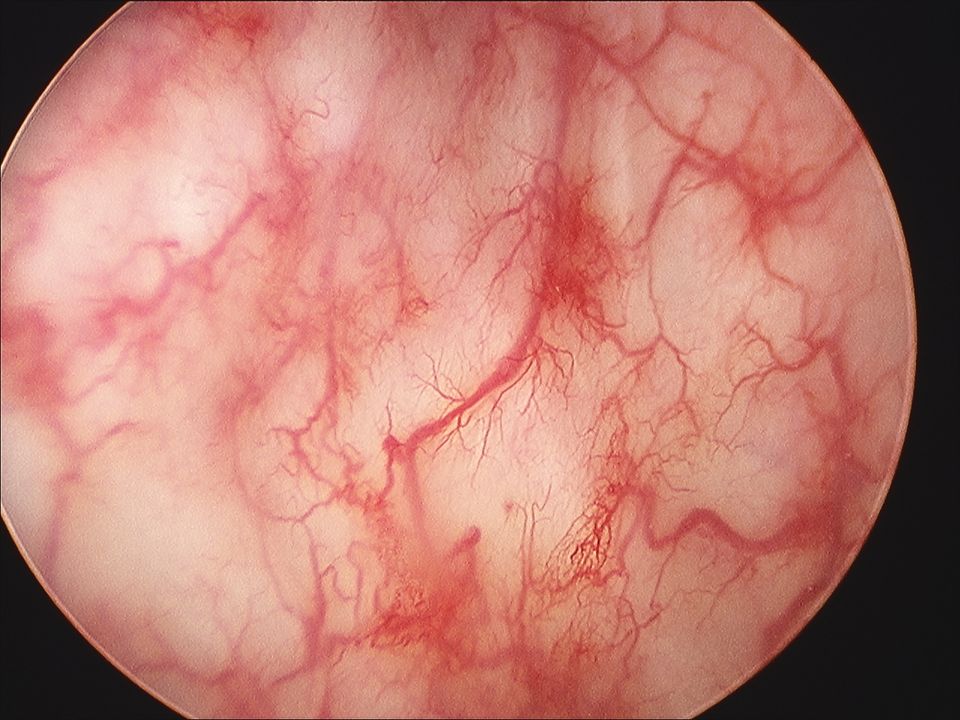
Radiation Cystitis

101
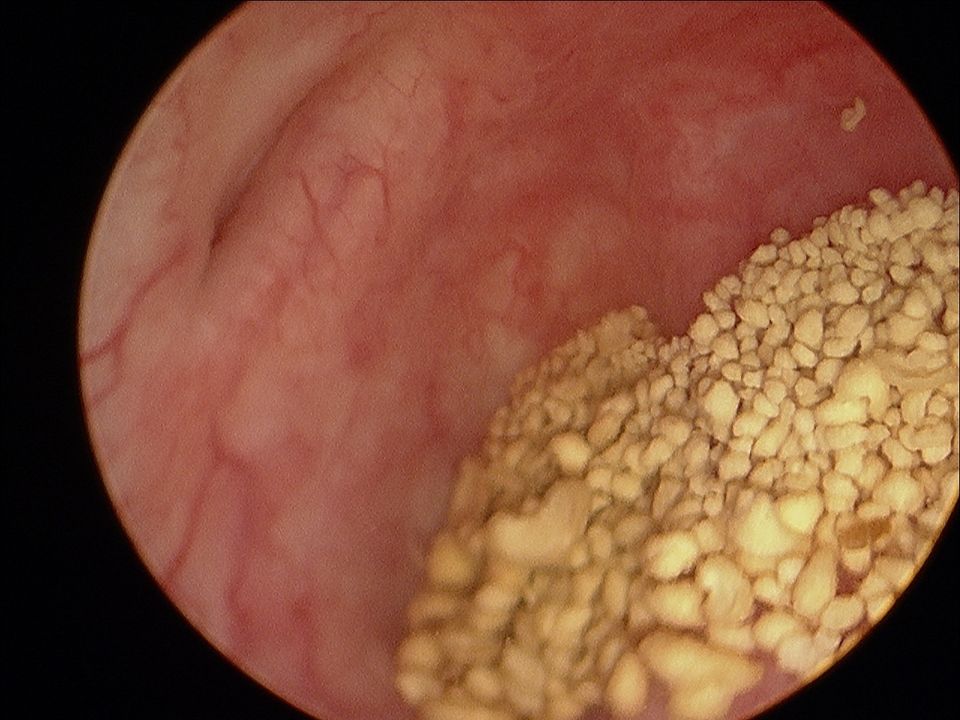
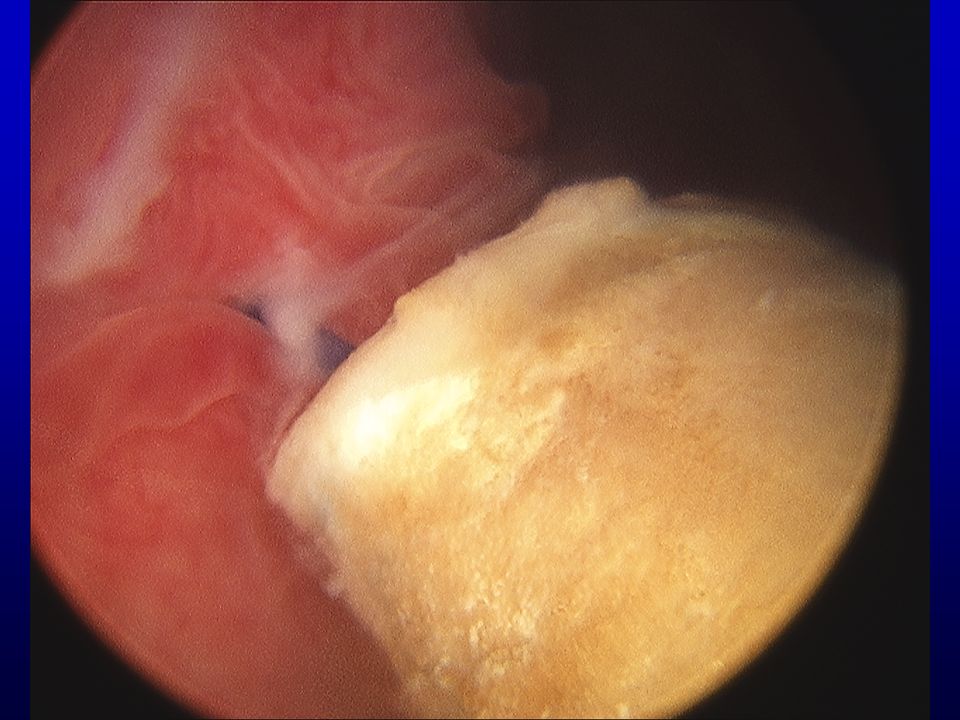
Bladder Stones

104
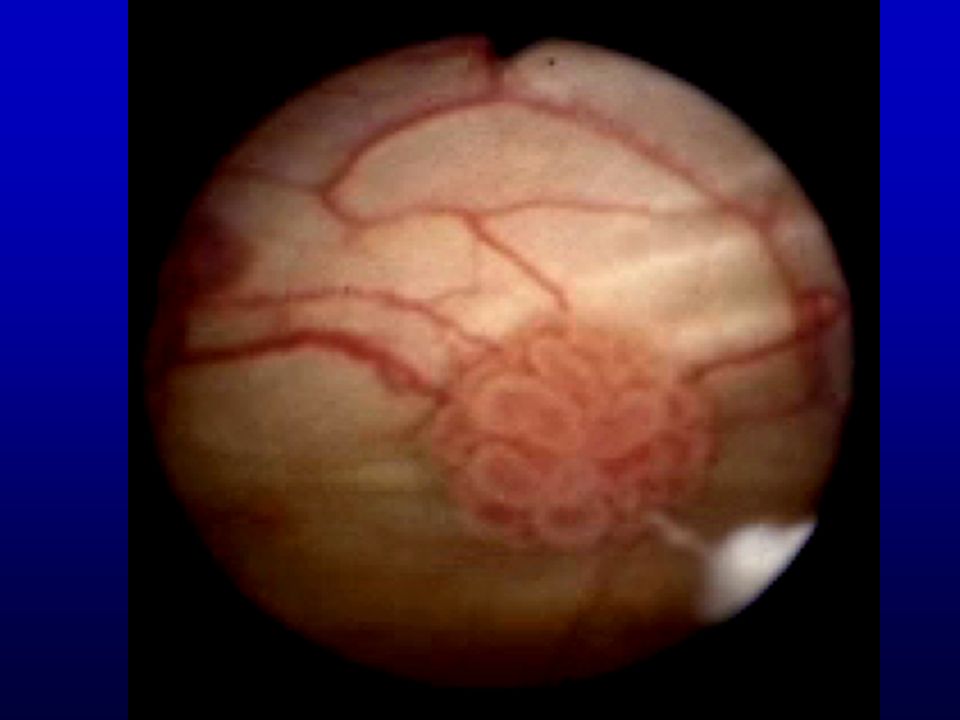
Low Grade Bladder Cancer

106
Carcinoma in Situ

107
CIS

108
Diagnostic Evaluation History & questionnaire Physical exam Urinalysis & culture Bladder diary

109
Initial Treatment Treatment of remediable conditions Behavioral therapy Pharmacotherapy Electrical stimulation

110
Remediable Conditions Uro-gynecologic Pelvic organ prolapse Stress incontinence Urethral diverticulum Bladder & ureteral stones Bladder cancer Medical UTI Polyuria Diabetes Congestive heart failure Medications

111
Indications for Further Workup Hematuria Recurrent UTI Diagnosis unclear Voiding symptoms Elevated PVR Neurologic disease Pelvic organ prolapse Prior pelvic surgery Bladder pain No Rx response after 2 – 3 months

112
112112112 112 Further Workup Urodynamics Cystoscopy

113
Treatment of Refractory OAB Botox injections Neuromodulation Enterocystoplasty Urinary diversion

114
The Many Faces of OAB

115
Is it really necessary to make these distinctions? That’s for you to decide, but remember, If the only tool you have is a hammer, everything looks like a nail!

Similar presentations
















>")



