Download presentation
Presentation is loading. Please wait.

1
Congenital malformations
Be not the first whom the new is tried Nor yet the last whom the old is cast aside. The secret of success is constant to purpose.

2
Common congenital lesions of the oral cavity
Cleft lip, Cleft palate, and Ankyloglosia (Tongue tie) Ankylosis (not true congenital problem)
 Ankylosis (not true congenital problem)")
3
Topics to be covered Cleft lip and palate Embryology Etiologic factors
Classification Problems of cleft Treatment of clefts Dental needs of cleft afflicted patients Prosthetic speech aid appliances

4
Topics Problems of the cleft Dental problems Nasal deformity Feeding
Ear problems Speech difficulties Associated anomalies

5
Topics Treatment of clefts Timing of cleft repair Cheilorrhaphy
Palatorrhaphy Alveolar cleft grafts Correction of maxillomandibular disharmonies Secondary surgical procedures

6
Introduction A cleft is a congenital space or gap in the upper lip, alveolus or palate. Cleft lip also known as “hare lip”. Cleft can be on Lip only Unilateral or bilateral Palate only Complete or incomplete Or both lip and palate

7
Classification Cleft lip alone Cleft palate alone Cleft lip and palate
Unilateral (one side only) Bilateral (both sides) Cleft palate alone Complete Incomplete Cleft lip and palate
 Bilateral (both sides) Cleft palate alone. Complete. Incomplete. Cleft lip and palate.")
9
Classification cont… Useful classification divides palate into;
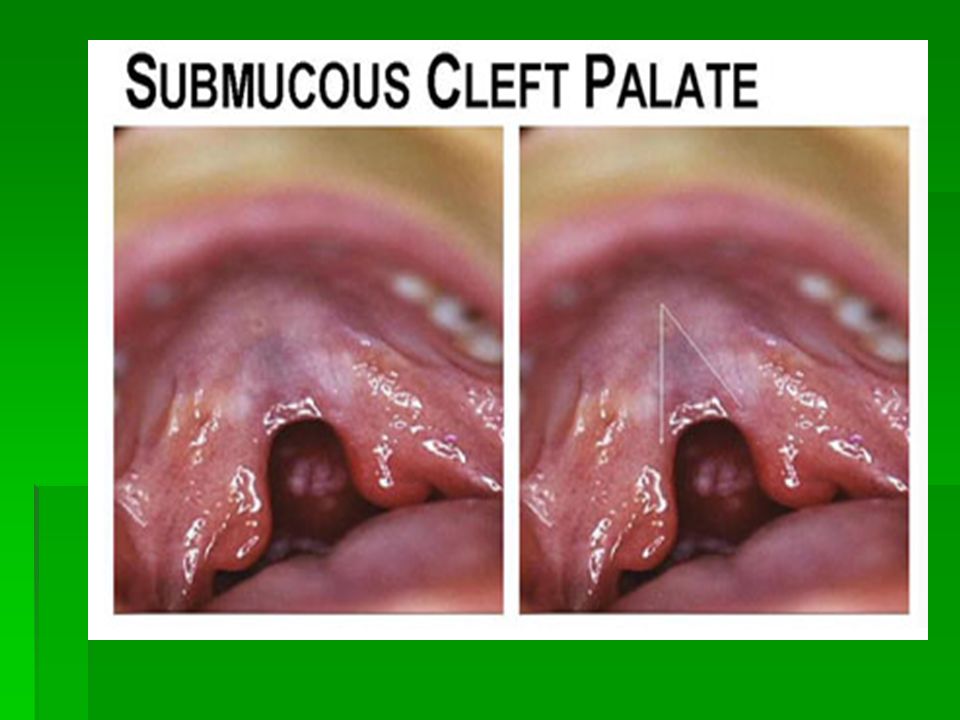
Primary palate Structure anterior to the incisive foramen. Pre-maxilla (lip and alveolus) Secondary palate Those structure posterior to the incisive foramen Hard and soft palate Cleft of the soft palate alone- bifid uvula.
 Secondary palate. Those structure posterior to the incisive foramen. Hard and soft palate. Cleft of the soft palate alone- bifid uvula.")
14
Epidemiology Occurrence of clefts in US is 1 in every 600 to 1000 live births. Clefts exhibit racial predilections Occur less frequently in blacks, more in orientals. Boys affected more often than females In ratio of 3:2. Cleft of lip more frequently in boys

15
Epidemiology cont… Whereas isolated cleft palates are more common in in girls. Oral clefts commonly affects lip, alveolar, hard and soft palate. Three fourth are unilateral clefts. One fourth are bilateral clefts.

16
Embryology Face develop around shallow ectodermal depression (stomatodeum). At first stomatodeum closed by the bucopharyngeal membrane which ruptures the 3rd week of embryonic life. Stomatodeum is surrounded on all sides by mesodermal swellings Unpaired frontal prominence (process) Paired maxillary prominence Paired mandibular prominence.
 Paired maxillary prominence. Paired mandibular prominence.")
17
Embryology cont… Bilateral nasal placodes develop in the ectoderm covering the frontal process above the stomodeum. Frontal process divided into medial and lateral nasal processes as nasal placodes appear. 5th week the nasal placodes become flanked by these medial and lateral nasal processes.

18
Embryology cont… Nasal pit formed when the swelling unite above and below the placode. Medial processes meet each other and fuse forming intermaxillaty segment. Intermaxillary segment will for; Middle portion of the nose The philtrum of the upper lip Premaxilla (for 4 incisors) Primary palate
 Primary palate.")
19
Embryology cont… Lateral processes will form the alae of the nose.
Nasal pit are temporary continuous ventrally with the stomodeum. But are closed off again as the medial frontonasal and maxillary processes unite beneath them. Furrow between the lateral frontonasal swellings and maxillary swellings is continuous laterally with that maxillary and frontomedial swellings and run from upper lip to the region of the developing eye. This is the nasolacrimal groove. It is eventually bridged by the processes on each side to form part of the nasolacrimal (tear) duct.
 duct.")
20
Embryology cont… Primary palate Secondary palate
Form from the intermaxillary segment. Secondary palate Originates from as shelf like outgrowths which appear 6th week from deep surface of each maxillary processes. When first formed these palatine processes are directed medially and downwards on either sides of the developing tongue.

21
Embryology cont… The processes reorientate themselves horizontally starting posteriorly so that they approach each other above the tongue. Eventually fusion occurs; Between the free edges of the palatine processes Between each process and the free edge of the primary palate anteriorly Between the newly formed secondary palate and the inferior margin of the nasal septum.

22
Embryology cont… Palate is usually completed by 60 days.
The point of union of the apex of the primary palate and the two processes of the secondary palate is marked by the incisive foramen.

23
Clinical aspects of embryology
Failure of fusion of maxillary processes –cleft lip. Failure in fusion of secondary palatal processes gives cleft palate. Cleft of lip and premaxilla gives “hare lip”

24
Etiological factors Hereditary is contributary factor
Environmental factors play contributory role at critical time of embryologic development when the lip and palatal halves are fusing. Nutritional deficiencies Radiation Several drugs Hypoxia Vitamin excess and defiencies.

25
Problems of the cleft Cleft of alveolus affect development the primary and secondary dentition and jaw itself. Most common problem is absence of teeth. Usually between lateral incisor and canine. Malocclusion Skeletal discrepancy between size, shape and position of teeth. Class III malocclusion in most cases. Mandibular prognathism most common finding, caused by maxilla retrusion than mandibular protrusion (Pseudoprognathism).
.")
26
Problems of the cleft cont…
Nasal deformity If clefts extend from into the floor of the nose, alar cartilage on that is flared, columella of the nose is pulled towards the non cleft side There is lack of underlying bony support to the base of the nose. Feeding Difficulty of producing negative pressure during sucking either breast or bottle milk. But baby can swallow normally once milk fed reaches the hypopharynx.

27
Problems of the cleft cont…
Ear problems Middle ear infection is common in children with cleft of the palate. Review anatomy of soft palate musculature (tensor veli palatini and levator veli palatini) are inserted into same muscles opposite side, And have origins directly or near auditory tube. The muscles allow opening of the ostium of this tube. Without action of this muscles the ostium is closed – no drainage mechanism, serous fluid accumulate.
 are inserted into same muscles opposite side, And have origins directly or near auditory tube. The muscles allow opening of the ostium of this tube. Without action of this muscles the ostium is closed – no drainage mechanism, serous fluid accumulate.")
28
Problems of the cleft cont…
Speech difficulties Created by cleft of lip and palate. Retardation of consonant sounds (p,b,t,d,k and g). Hypernasality is usual in cleft of nasal palate. Associated anomalies Associated congenital problems can be clubfoot to neurological disturbances (30%). Congenital heart disease (10%) Mental retardation (10%), etc.
. Hypernasality is usual in cleft of nasal palate. Associated anomalies. Associated congenital problems can be clubfoot to neurological disturbances (30%). Congenital heart disease (10%) Mental retardation (10%), etc.")
29
Treatment Cleft lip and palate
Aim of repair is to correct the cleft and associated problems, thus remove the anomally so that patient can live normal life. Surgical correction of deformity Vocal apparatus that permit intelligible speech Dentition that allows optimal function and esthetics

30
Treatment cont… Timing of surgical repair
Cleft lip (rule of 10). Cleft lip repaired earlier than palate. Exact time still debatable. Rule of 10- health baby is fit for surgery. 10 weeks of age 10 pounds in body weight At least 10 g/dl of Hb. Soft palate cleft closed between 18 and 24 moths of age. Hard palate cleft is closed between in preschool age that is between 4 and 5 years.
. Cleft lip repaired earlier than palate. Exact time still debatable. Rule of 10- health baby is fit for surgery. 10 weeks of age. 10 pounds in body weight. At least 10 g/dl of Hb. Soft palate cleft closed between 18 and 24 moths of age. Hard palate cleft is closed between in preschool age that is between 4 and 5 years.")
31
Treatment cont… Cheilorrhaphy is the surgical correction of the cleft lip deformity. Objectives; Functional Aesthetics Palatorrhaphy is the surgical correction of palate. May be performed in one or two operation In two operation staphylorrhaphy (soft palate closure) is usually performed first and Hard palate closure (Uronorrhaphy) is performed second.
 is usually performed first and. Hard palate closure (Uronorrhaphy) is performed second.")
32
Treatment cont… Objective; to create mechanism capable of speech and deglutition without significantly interfering with subsequent maxillary growth. Alveolar cleft grafts Alveolar cleft defects not corrected in the original surgical correction. Alveolar cleft bone graft provide several advantages

33
Treatment cont… Advantages of alveolar cleft graft
Unite alveolar segments and help prevent collapse and constriction of the dental arch. Provide bone support for teeth adjacent to the cleft and for those that will erupt into area of cleft. Closure of the oroantral fistulla

34
Correction of maxillomandibular disharmony
People with cleft exhibit maxillary retrusion and transverse maxillary constriction resulting from the cicatricial contraction of previous surgeries. Secondary surgical procedures are performed after the initial repair of the clefts defects in an effort to improve the speech or correct residual defects.

35
Dental needs of cleft affected patients
Placing a denture to replacing congenitally missing lateral incisor before alveolar ridge graft. Frequent prophylaxis and special oral hygiene instructions with carefully reinforcement, because of the malformed or absent teeth, sometimes are in the cleft, predisposing them to periodontitis.

36
Dental needs of cleft affected patients cont…
Prosthetic speech appliances Teeth missing should be replaced. Patients who have failed to obtain velopharyngeal competence need speech appliance to decrease hypernasal speech.

37
Treating clefts is as playing chase, think, plan, see and do as you see.
Remember when you hear you forget, when you see you remember, and when you do you understand.

Similar presentations