Download presentation
Presentation is loading. Please wait.

1
Insulin Elixir of life Dr. Sergio Diez Alvarez Staff Specialist Physician

2
The Challenge Mr XL has type 2 diabetes and has been on Oral Hypoglycemic Agents (metformin + glibenclamide) for 8 months, his HbA1c is 8.3% and you have decided to offer him the option of going on to insulin. Mr XL has type 2 diabetes and has been on Oral Hypoglycemic Agents (metformin + glibenclamide) for 8 months, his HbA1c is 8.3% and you have decided to offer him the option of going on to insulin.
 for 8 months, his HbA1c is 8.3% and you have decided to offer him the option of going on to insulin..")
3
In theory, there is no difference between theory and practice. In practice, there is a big difference. - Unknown

4
Understand the Stakeholders The Willing Patient The Willing Patient The Willing Clinician The Willing Clinician The Insulin type and Regimen The Insulin type and Regimen The Delivery Device The Delivery Device Safety Accessories Safety Accessories Other factors Other factors

5
The Patient Insulinopaenia – beta cell reserve Insulinopaenia – beta cell reserve Insulin Resistance – mainly hepatic, muscle, and adipose tissues Insulin Resistance – mainly hepatic, muscle, and adipose tissues Type 1 – complete insulin deficiency Type 1 – complete insulin deficiency Type 2 – Insulin dependent (LADA) vs. insulin requiring Type 2 – Insulin dependent (LADA) vs. insulin requiring
 vs. insulin requiring.")
6
DAWN Study Resistance to Insulin Therapy Among Patients and Providers Resistance to Insulin Therapy Among Patients and Providers Results of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) study Results of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) study Diabetes Care November 2005 vol. 28 no. 11 2673-2679 Diabetes Care November 2005 vol. 28 no. 11 2673-2679

7
Patients Patients rate the clinical efficacy of insulin as low and would blame themselves if they had to start insulin therapy. Patients rate the clinical efficacy of insulin as low and would blame themselves if they had to start insulin therapy. Self-blame is significantly lower among those who have better diet and exercise adherence and less diabetes-related distress. Self-blame is significantly lower among those who have better diet and exercise adherence and less diabetes-related distress. Patients who are not managing their diabetes well (poor perceived control, more complications, and diabetes-related distress) are significantly more likely to see insulin therapy as potentially beneficial. Patients who are not managing their diabetes well (poor perceived control, more complications, and diabetes-related distress) are significantly more likely to see insulin therapy as potentially beneficial.
 are significantly more likely to see insulin therapy as potentially beneficial. Patients who are not managing their diabetes well (poor perceived control, more complications, and diabetes-related distress) are significantly more likely to see insulin therapy as potentially beneficial..")
8
The Clinician Most nurses and general practitioners (50–55%) delay insulin therapy until absolutely necessary, but specialists and opinion leaders are less likely to do so. Most nurses and general practitioners (50–55%) delay insulin therapy until absolutely necessary, but specialists and opinion leaders are less likely to do so. Delay of insulin therapy is significantly less likely when physicians and nurses see their patients as more adherent to medication or appointment regimens, view insulin as more efficacious, and when they are less likely to delay oral diabetes medications. Delay of insulin therapy is significantly less likely when physicians and nurses see their patients as more adherent to medication or appointment regimens, view insulin as more efficacious, and when they are less likely to delay oral diabetes medications. Resources were considered barely adequate currently and there were concerns about worsening problems with increasing numbers of patients with diabetes, and increased use of insulin Resources were considered barely adequate currently and there were concerns about worsening problems with increasing numbers of patients with diabetes, and increased use of insulin
 delay insulin therapy until absolutely necessary, but specialists and opinion leaders are less likely to do so. Delay of insulin therapy is significantly less likely when physicians and nurses see their patients as more adherent to medication or appointment regimens, view insulin as more efficacious, and when they are less likely to delay oral diabetes medications. Delay of insulin therapy is significantly less likely when physicians and nurses see their patients as more adherent to medication or appointment regimens, view insulin as more efficacious, and when they are less likely to delay oral diabetes medications. Resources were considered barely adequate currently and there were concerns about worsening problems with increasing numbers of patients with diabetes, and increased use of insulin Resources were considered barely adequate currently and there were concerns about worsening problems with increasing numbers of patients with diabetes, and increased use of insulin.")
9
Clinicians Shifting 1980s - clinicians tended to be more pessimistic than patients and overestimate the barriers complying with treatment. 1980s - clinicians tended to be more pessimistic than patients and overestimate the barriers complying with treatment. Insulin was seen as efficacious but there was resistance because of a lack of support, a skills deficit, and a lack of confidence and experience in starting insulin. Insulin was seen as efficacious but there was resistance because of a lack of support, a skills deficit, and a lack of confidence and experience in starting insulin.

10
Psychological Resistance 6 Remember – at time of Diagnosis 50% of -cell function is already lost. 6 Insulin must be regarded as “expected therapy”. Not “Failure” Not “Failure” Not “Last Resort” Not “Last Resort” Not “End-stage therapy” Not “End-stage therapy” AND SHOULD BE STARTED MUCH EARLIER Innovators vs. Conservative Clinicians

11
History of Insulin Insulin first isolated 1921 by Banting and Best Insulin first isolated 1921 by Banting and Best Insulin first used as a treatment for diabetes in 1922 Insulin first used as a treatment for diabetes in 1922 Had short duration period and required several daily injections Had short duration period and required several daily injections Had to be given through reusable glass syringes with large often blunted needles Had to be given through reusable glass syringes with large often blunted needles

12
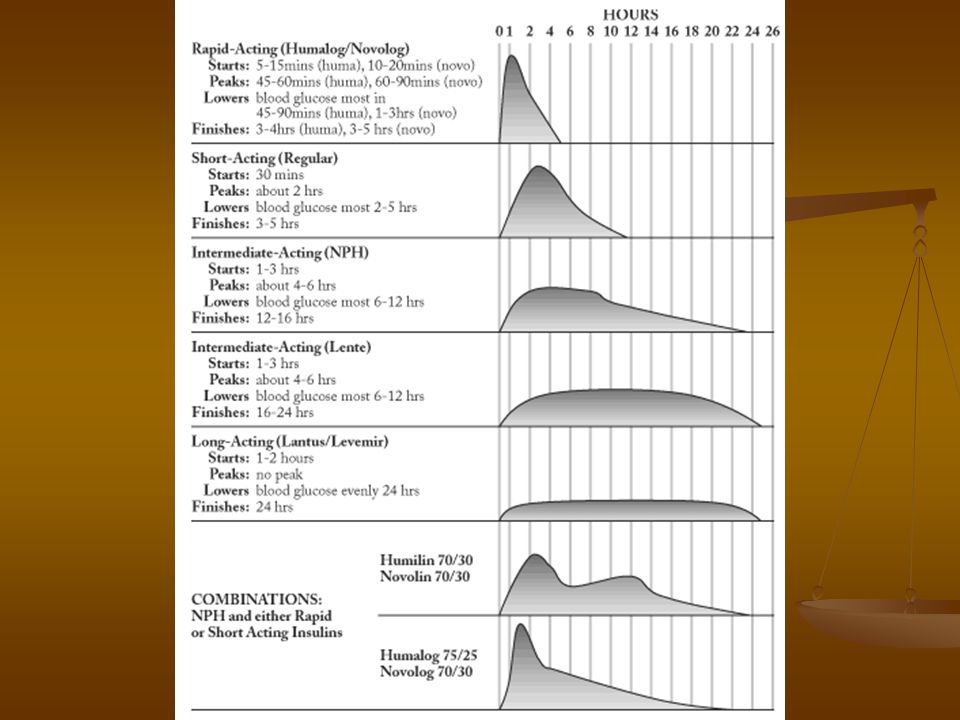
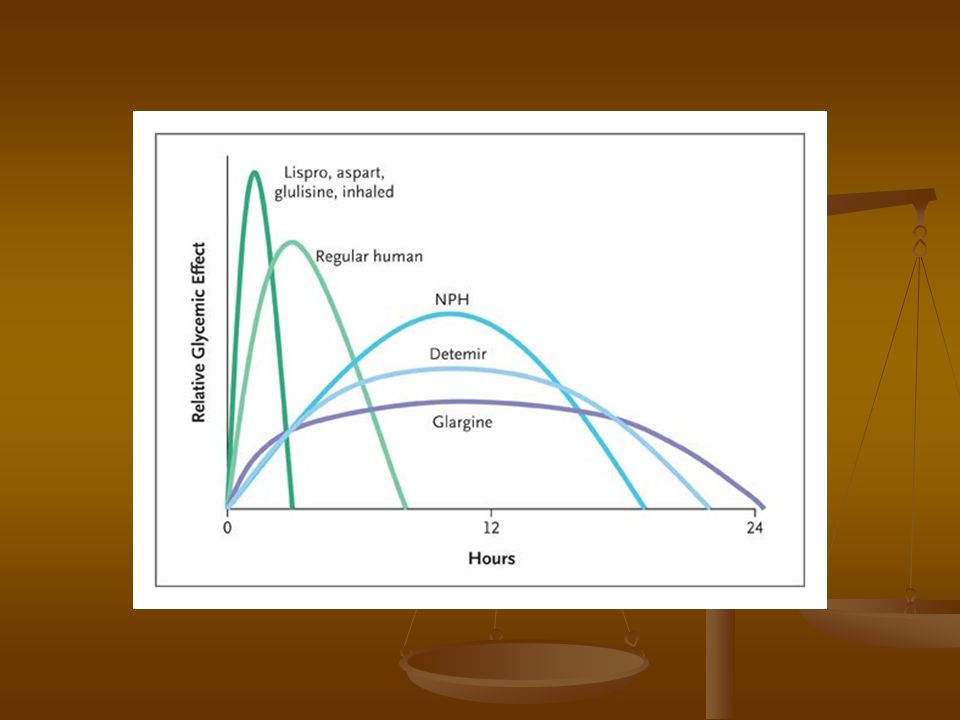
The Insulin Types Human vs. Analogs Human vs. Analogs Long Acting Insulin (Basal) Long Acting Insulin (Basal) Short Acting Insulin (Bolus) Short Acting Insulin (Bolus) Pre-mixed Insulins Pre-mixed Insulins
 Long Acting Insulin (Basal) Short Acting Insulin (Bolus) Short Acting Insulin (Bolus) Pre-mixed Insulins Pre-mixed Insulins.")
16
24-hour plasma glucose and insulin profiles in healthy individuals Owens DR et al. Lancet 2001;358:739–746 The Lancet, 2001, Vol 358, pages 739–746.

19
Insulin Regimens There is NO best Insulin – there is only the Right Insulin for the Right Patient There is NO best Insulin – there is only the Right Insulin for the Right Patient Daily Bolus (in combination with OHA's) Daily Bolus (in combination with OHA's) Twice daily Twice daily Basal bolus Basal bolus Basal plus 1,2,3 Basal plus 1,2,3 CIIS CIIS These can all be used in combination with OHAs ( especially insulin sensitizing agents) These can all be used in combination with OHAs ( especially insulin sensitizing agents)
 Daily Bolus (in combination with OHA s) Twice daily Twice daily Basal bolus Basal bolus Basal plus 1,2,3 Basal plus 1,2,3 CIIS CIIS These can all be used in combination with OHAs ( especially insulin sensitizing agents) These can all be used in combination with OHAs ( especially insulin sensitizing agents)")
20
Delivery Devices Syringes Syringes Pen-sets – disposable or Refill Pen-sets – disposable or Refill Continuous Insulin Infusion Pump Continuous Insulin Infusion Pump

21
Glucose Monitoring Standard (simplified) Glucometer Standard (simplified) Glucometer Blood Ketone measuring (for Insulin dependent patients) Blood Ketone measuring (for Insulin dependent patients) Continuous Glucose Monitoring Device Continuous Glucose Monitoring Device
 Glucometer Standard (simplified) Glucometer Blood Ketone measuring (for Insulin dependent patients) Blood Ketone measuring (for Insulin dependent patients) Continuous Glucose Monitoring Device Continuous Glucose Monitoring Device")
22
Other (important ) Factors Family Family Friends (peers or colleagues) Friends (peers or colleagues) Co-morbidities Co-morbidities Diabetic Complications e.g. retinopathy Diabetic Complications e.g. retinopathy Media (including internet) Media (including internet)
 Media (including internet).")
23
After Sales Strategy Match the regime to the patient What is the target HbA1c? What is the target HbA1c? How avidly should hypos be avoided? How avidly should hypos be avoided? How many injections is the patient willing to give? How many injections is the patient willing to give? Fasting or postprandial the greater problem? Fasting or postprandial the greater problem? What device can the patient use? What device can the patient use?

24
% contribution. 40 60 80 100 0 Relative contribution of FPG & PPG to hyperglycaemia. 65 17 31 FPG contribution. PPG contribution. 83 69 35 <7.3%7.3%-8.0%>8.0% HbA 1c tertiles : 20 p=0.048 p=0.001 (12 hour profile) Peter R, Owens DR et al- Diab Med- 2004
 Peter R, Owens DR et al- Diab Med")
25
Complications Lipodystrophy Lipodystrophy Lipoatrophy & lipohypertrophy Lipoatrophy & lipohypertrophy

Similar presentations


 Fellow of KIMS Endocrine, Diabetes and Metabolism.>")
 + GIP = incretin effect =Augmentation of insulin after oral glucose Type 2 diabetics little incretin effect Reduced GLP-1 secretion.>")
. 2 Hyperglycaemia Learning objectives >Can state what hyperglycaemia is >Is aware of the short term and.>")
>")

. 2 Insulin Learning outcomes >Understand the difference between insulin therapy in type 1 diabetes as compared to.>")











