Download presentation
Presentation is loading. Please wait.

1
Urinary diversion

2
Introduction Diversion of urinary pathway from its natural path Types:
Temporary Permanent

3
Indications of permanent urinary diversion
When the bladder has to be removed When the sphincters of the bladder & the detrusor muscle have been damaged or have lost their normal neurological control When there is irremovable obstruction in the bladder & distal to that Ectopic vesicae Incurable vesico- vagina fistula

4
Temporary urinary diversion
Suprapubic cystostomy Pyelostomy or nephrostomy or urethrostomy (with indwelling catheters)
")
5
Illustration of suprapubic tube placed to aid bladder drainage

6
A nephrostomy is a surgical procedure by which a tube, stent, or catheter is inserted through the skin and into the kidney.

7
Permanent urinary diversion
Uretero - sigmoidostomy Ileal conduit Colon conduit Ileocaecaecal segment Lowsley’s operation

8
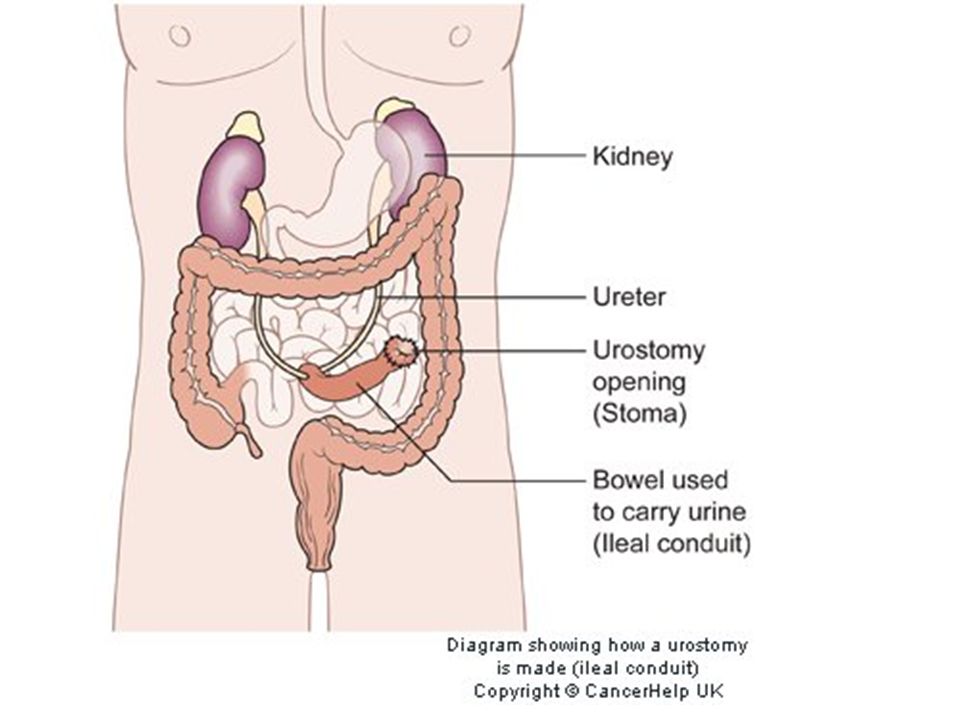
Types of urinary diversions
Cutaneous urinary diversions Ileal conduit (ileal loop) A 12 cm loop of ileum led out through abdominal wall Stents used The space at cystectomy site drained by a drainage system After surgery a skin barrier and a transparent disposable urinary drainage bag Constantly drains
 A 12 cm loop of ileum led out through abdominal wall. Stents used. The space at cystectomy site drained by a drainage system. After surgery a skin barrier and a transparent disposable urinary drainage bag. Constantly drains.")
10
Complications of ileal conduit
Wound infection Wound dehiscence Urinary leakage Ureteral obstruction Small bowel obstruction Ileus Stomal gangrene Narrowing of the stoma Pyelonephritis Renal calculi

11
Cutaneous Ureterostomy…

12
Vesicostomy

13
Nephrostomy…

14
Uretero- sigmoidostomy
Complications: Reflux of urine Hyperchloraemic acidosis Renal infection Stricture formation

15
Continent Urinary Diversions
Continent Ileal Urinary Reservoir Indiana Pouch Most common continent urinary diversion Periodically catheterized Koch Pouch Charleston Pouch Ureterosigmoidostomy Voiding occurs from rectum

18
Koch Pouch II

19
ureterosigmoidostomy

20
Potential complications
Peritonitis due to disruption of anastomosis Stomal ischaemia and necrosis due to compromised blood supply to stoma Stoma retraction and separation of mucocutaneous border due to tension or trauma

22
Bladder reconstruction

23
Recto sigmoid pouch

24
Nursing process : The patient undergoing urinary diversion surgery
Preoperative assessment : Cardiopulmonary assessment Nutritional assessment Learning capcity assessment Preoperative nursing diagnosis Anxiety Knowledge deficit Preoperative planning and goals Relief of anxiety Ensuring adequate nutrition Explaining surgery and its effects

25
Nursing Management In the immediate postoperative period urine volumes are monitered hourly An output below 30 ml/h dehydration or obstruction Promote urine output – a catheter may be inserted through urinary conduit Provide stoma and skin care – consult with enterostomal therapist Skin care specialist consulted Stoma looked for color – dark purplish –blood supply compromised Skin inspected for irritation Bleeding Wound infections

26
Postoperative nursing interventions
Monitor urinary function Prevent complications infection, sepsis, respiratory, complications, fluid and electrolyte imbalances, fistula formation. Ryle’s tube aspiration Ambulate quickly Maintain peristomal integrity Relieve pain Improve body image Exploring sexuality issues Treat peritonitis Look for stomal ischaemia and necrosis Look for stomal retraction and separation

27
Neomycin, kanamycin Immediately after operation – catheter in rectum – to prevent reflux into ureters and infection of the newly formed ureteric opening into the intestines Monitoring fluid and electrolytes : intestinal mucosa absorb urine water and electrolytes; diarrhoea due to potassium and magnesium; maintain the balance. Pt advised to empty the rectum every 2 hours to ↓ build up of pressure and thereby the absorption of urinary salts Retrain the rectum – special sphincteric exercises – learn the differentiate between the need to defaecate and the need to urinate

28
Promoting dietary measures – avoid chewing gum, smoking.
Salt intake restricted to prevent hyperchloremic acidosis. Potassium increased to make up for potassium lost in acidosis Monitoring and managing potential complications : - pyelonephritis due to reflux of bacteria from rectum – long term antibiotics – late complication due to irritation - adenocarcinoma

29
Managing ostomy appliance
Empty the pouch when 1/3 full to prevent weight pulling down A small amount of urine is left to prevent collapse of the bag against itself The collecting bottle and tubing is rinsed with cold water daily and once in a week with a 3:1 solution of water and white vinegar Continuing care – look for metastases

30
Look for leakage of urine from the appliance
Urine pH is kept below 6.5 by administration of ascorbic acid Appliance to be fitted properly to prevent skin from getting irritated by urine If the urine is foul smelling C&S done Ileal conduit – mucosa – mucus produced – urine gets mixed with mucus – patient encouraged to take lot of fluid to wash out the mucus. Appliances : reusable or disposable Skin barrier used to protect skin from urine

31
Promoting home and community care
Teach patients self care Control odour : food that gives odour to urine avoided e.g. Cheese, eggs Deodorizers or dilute white vinegar introduced into the drainage bag Ascorbic – acidifies – suppresses odour Aspirin introduced into bag to deodorize may cause ulceration of the stoma

32
Home and community care
Teaching self care Continuing care

33
Future aspects More than 40 variants of continent diversion, no single best technique Which bowel segment ? Which continent technique ? Which anti-reflux technique ? Only long term follow up can answer these questions

Similar presentations