Download presentation
Presentation is loading. Please wait.

1
R و ما أوتيتم من العلم الا قليلا د.برع سلطان مدرس \جراحة الفم والوجه والفكين BDS, MSc, FICMS

2
PRE-OPERATIVE ASSESSMENT of the difficulty of tooth extraction.

3
1 -patient cooperation and consent. 2- Age of the patient : children – small mouth ----- difficult access “ uncooperative ”, in old age patients : roots are brittle and bone is dense.(glass in a concrete syndrome). 3- General build up of the patient : obesity, heavily built patient differ from slim thin patient. 4- Mouth opening of the patient : Patients with scar, burn, acute pericoronitis or TMJ dysfunction may have difficulty in mouth opening.
. 3- General build up of the patient : obesity, heavily built patient differ from slim thin patient. 4- Mouth opening of the patient : Patients with scar, burn, acute pericoronitis or TMJ dysfunction may have difficulty in mouth opening..")
4
5- The general cleanliness of the patient and his mouth ( oral hygiene) are observed. Wherever possible, a careful pre-extraction scaling should be performed, at least one week before tooth extraction, because local healing processes may be delayed unless the mouth is thoroughly cleaned prior to removal of teeth.

5
It is also possible for the patient to inhale fragments of calculus during the extraction, especially when the surgery is performed under general anesthesia in the dental chair. This may cause a pulmonary infection.

7
6- Crown of the tooth to be extracted. 1- Size of the crown. 2- Extensive crown destruction by caries, abrasion, and attrition complicate forceps application. 3- Teeth with large filling may be fractured during extraction. 4- Crowned tooth : the cover may be separated from the tooth during extraction & it may cause difficulty for forceps adaptation.

8
5- Crowns that are united to adjacent teeth by a bridge or an orthodontic wire should be separated before extraction. 6- level of eruption : Extraction of completely erupted tooth is simpler than impacted tooth. 7- site of the tooth: Rotated or malposed teeth are difficult to be removed. 8- Isolated teeth are more difficult to remove than non- isolated.

10
7 - Clinical evaluation of the periodontium 1- In a tooth with increased mobility ( periodontal disease )alveolar bone will be replaced by granulation tissue thus gain difficulty in securing anesthesia. Removal of granulation tissue may cause post operative hemorrhage and delay in healing process.

11
2- Draining fistula or mucosal tract adjacent to the tooth to be extracted should excised. 3- In gingival conditions that suggest an underlying blood dyscrasia ( leukemia ), all extractions should be delayed until these conditions controlled or treated.
, all extractions should be delayed until these conditions controlled or treated..")
12
8- Clinical examination of Adjacent structures. 1- Large fillings on neighboring teeth may be fractured or displaced during the process of tooth extraction. 2- Adjacent teeth if Malposed or crowned are easily fractured or subluxated. 3- size of the tongue ( MACROGLOSSIA ) increase difficulty of tooth extraction. 4-size of the cheek: Heavily muscular cheeks will increase difficulty of tooth extraction. 5- Large mesially carious & mesially drifted 1 st molar ( deep contact with crown of 2 nd premolar ) increase the difficulty to extract the lower 1 st molar.
 increase difficulty of tooth extraction. 4-size of the cheek: Heavily muscular cheeks will increase difficulty of tooth extraction. 5- Large mesially carious & mesially drifted 1 st molar ( deep contact with crown of 2 nd premolar ) increase the difficulty to extract the lower 1 st molar..")
13
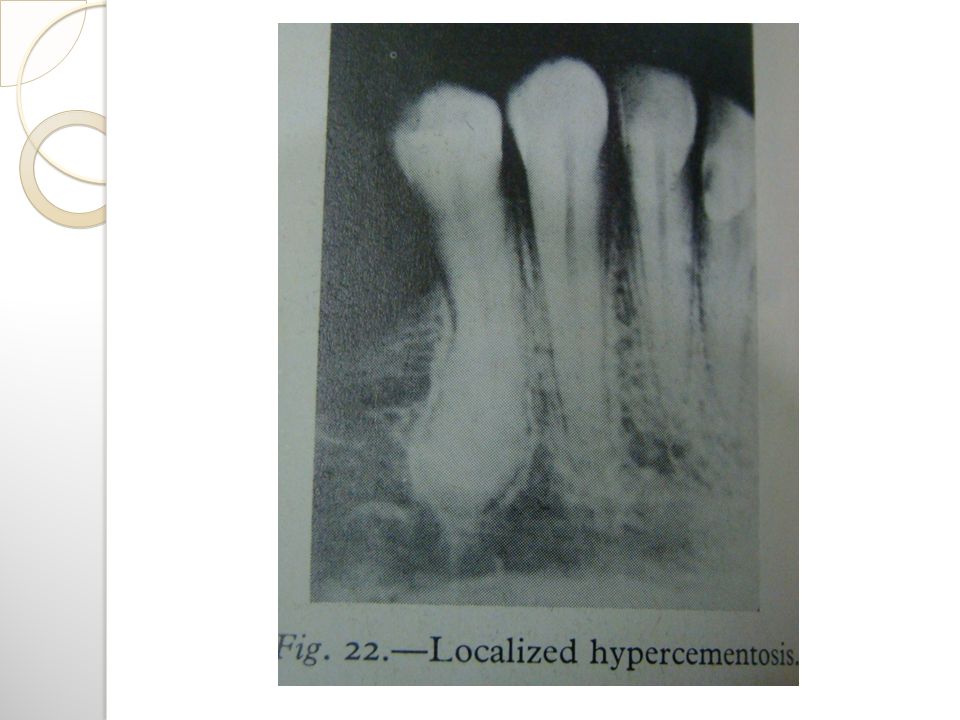
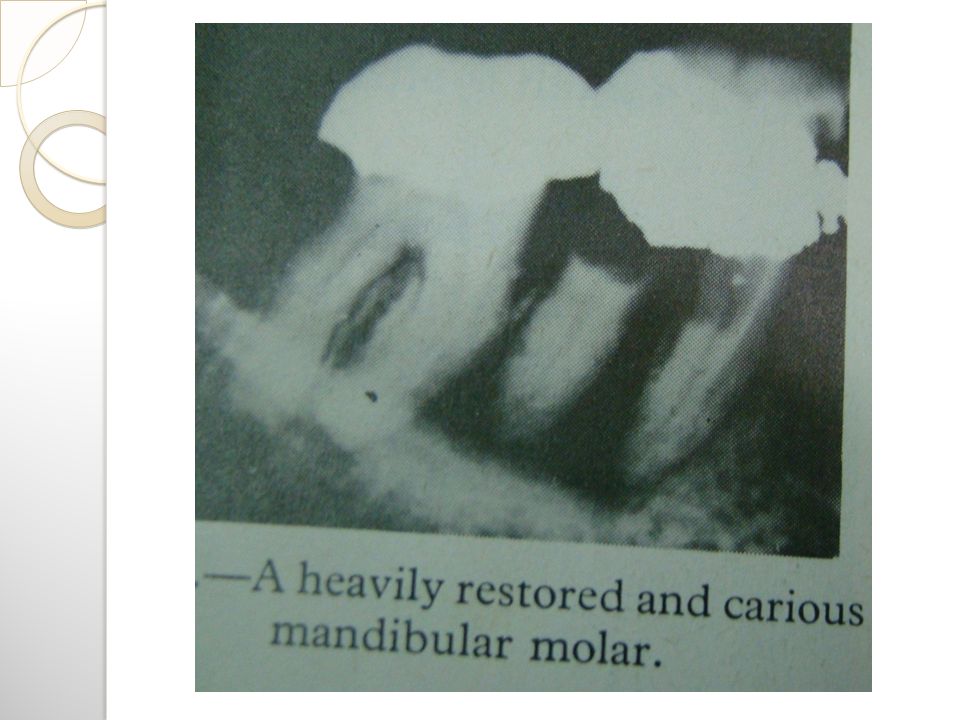
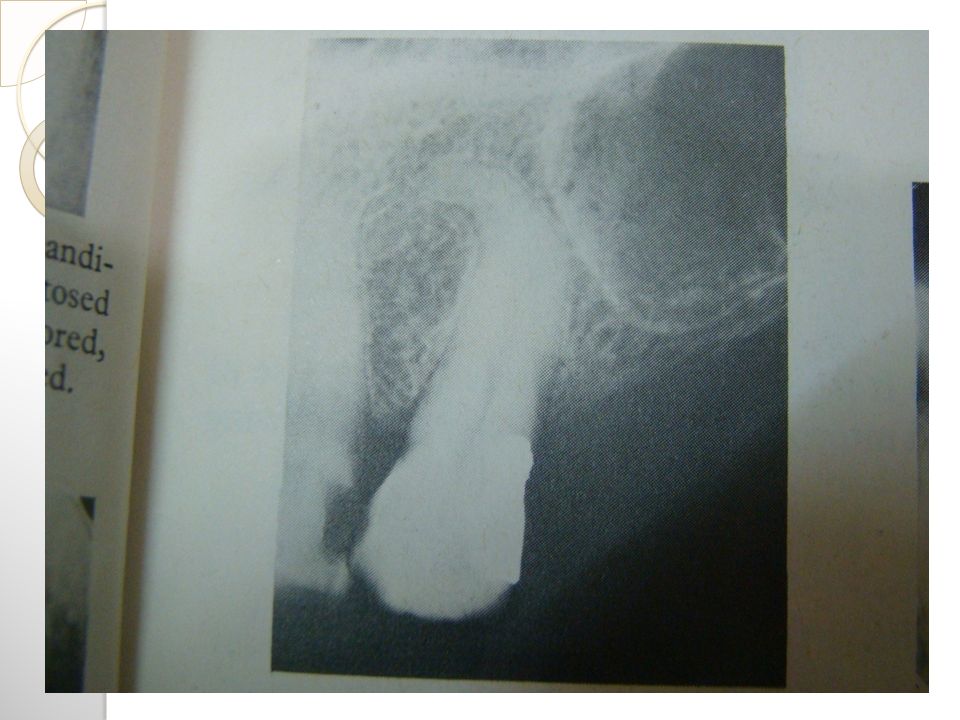
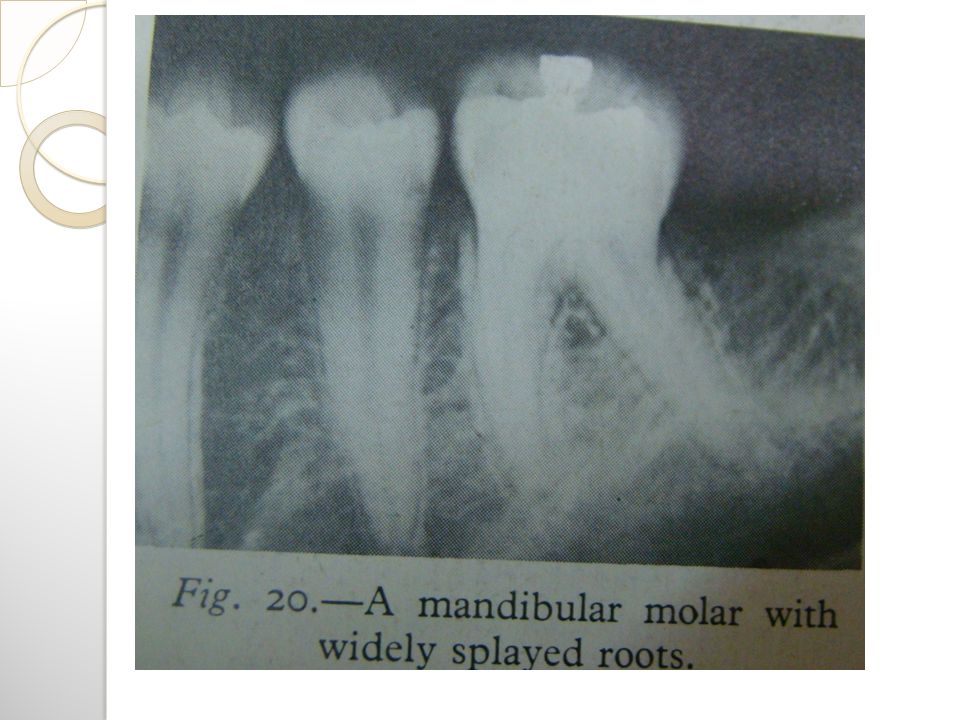
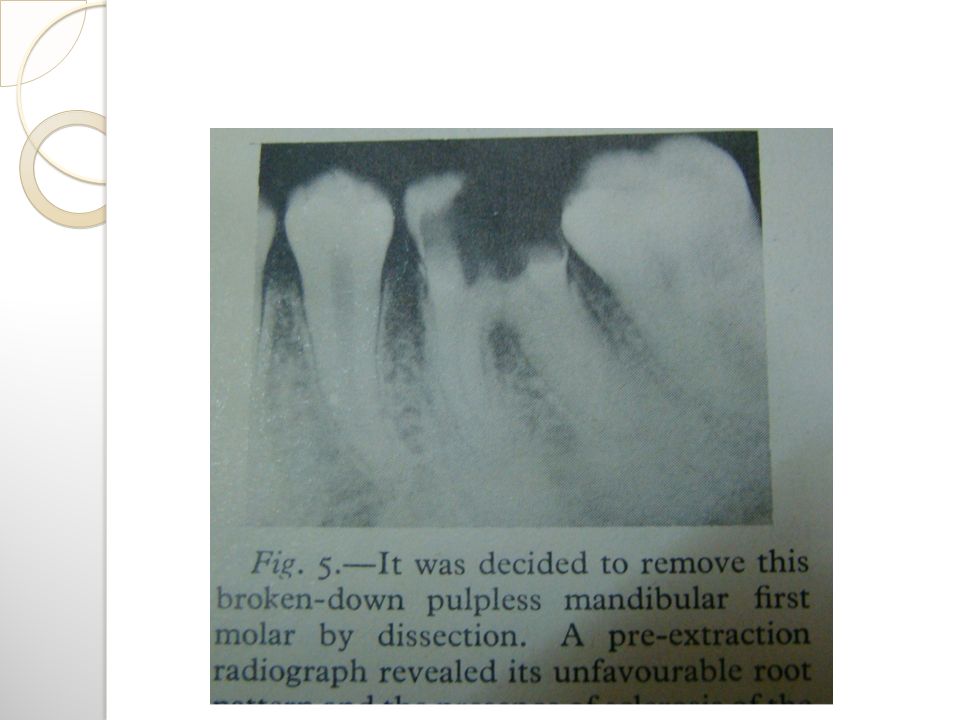
RADIOGRAPHICAL EVALUATION 1.Crown : sub-gingival proximal caries, heavily restored tooth. 2.Root : a- Long thin, abnormal no. of roots fracture. b- Curved, dilacerated roots. c- Prominent bulbous & hypercementosed roots are indicated for open extraction. d- Root caries, deciduous roots or roots affected by internal or external resorption are liable to fracture.

14
14

15
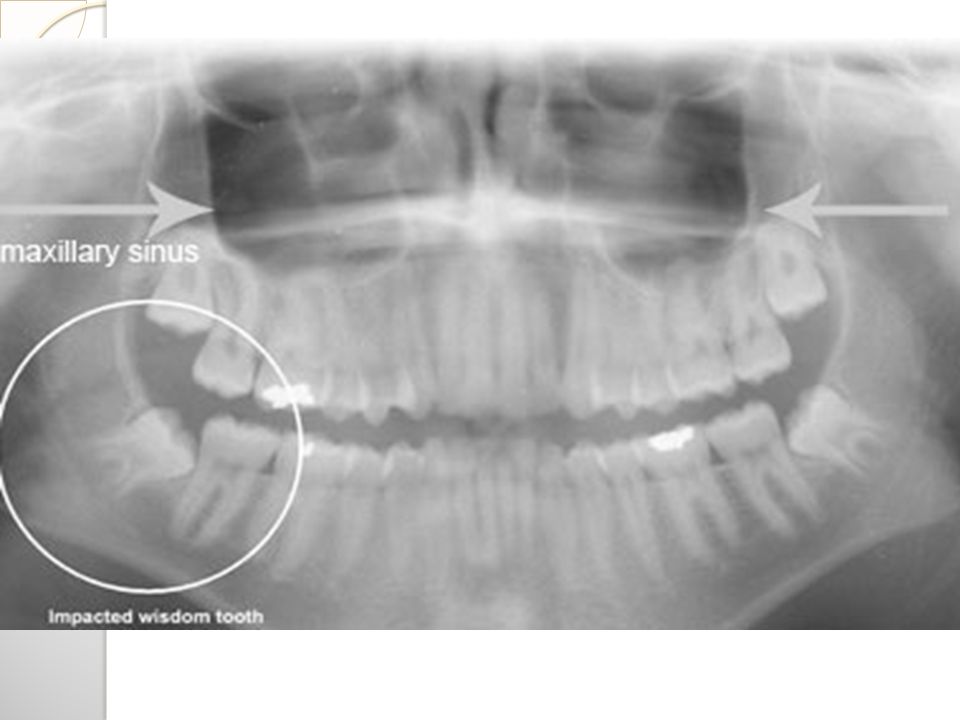
2.Root (cont.): e- any endodontically treated teeth are expected to fracture. f- Ankylosis …. open extraction is indicated. g- The radiograph reveals the proximity to adjacent vital structures like maxillary sinus, nasal cavity, and inferior alveolar canal.

17
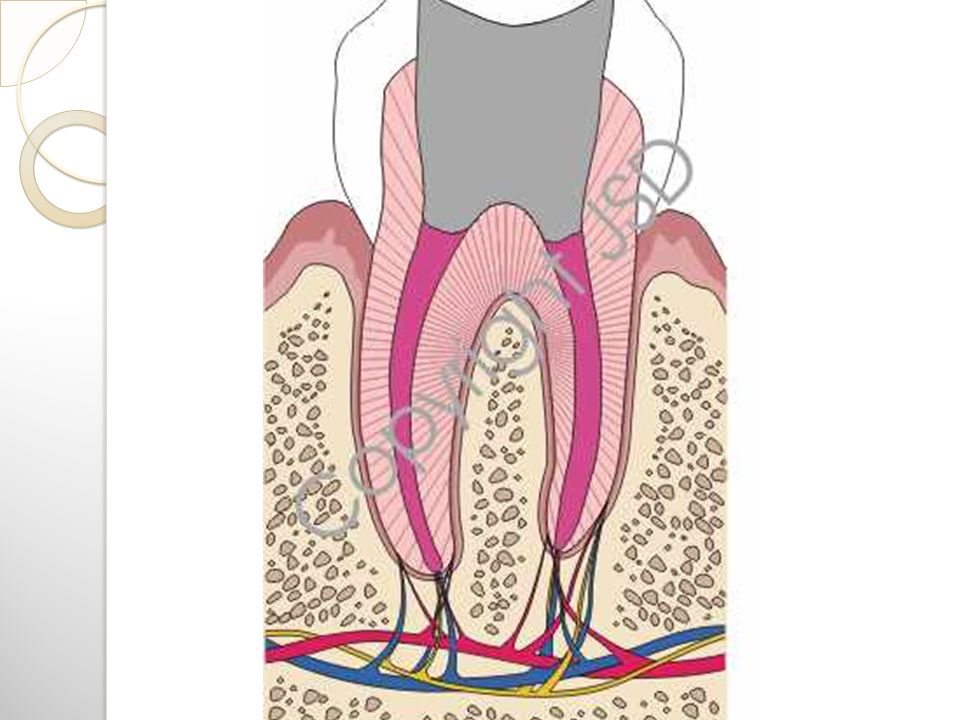
3- The bone : A PERIAPICAL FILM gives accurate information about a- Degree of mineralization of the investing bone. b- Condition of periodontal ligament. A PANORAMIC RADIOGRAPH SHOWS : Inferior border of mandible, inferior alveolar canal, mental foramen, maxillary sinus, fracture of mandible, etc ….

18
Density of the bone

20
A good radiograph is wasted unless it is carefully interpreted. The use of a hand lens and viewing box greatly aid interpretation.

21
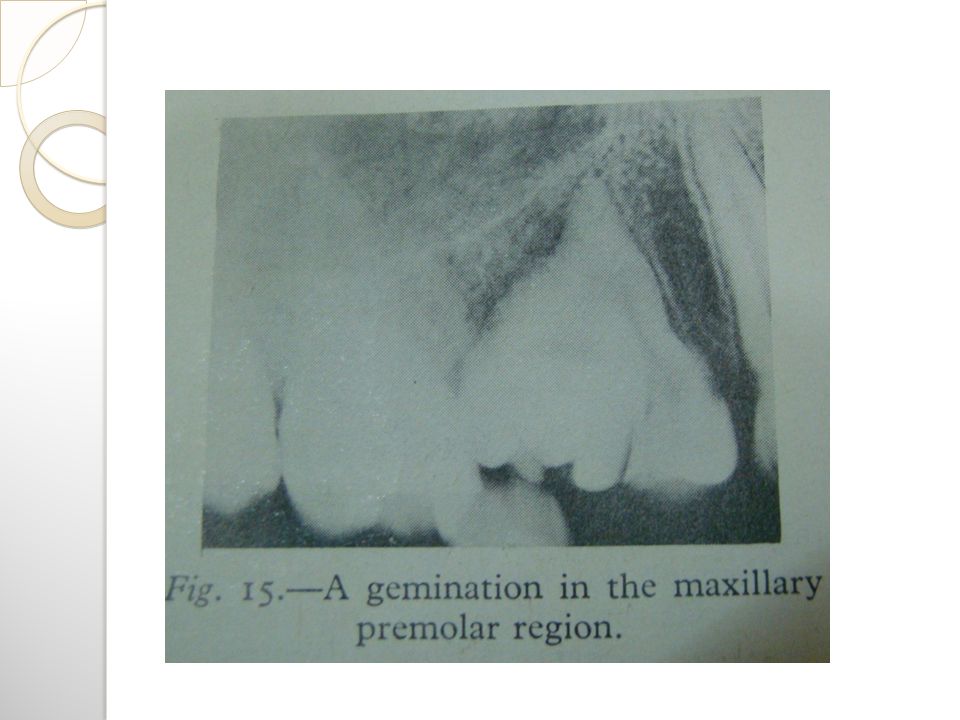
The following factors causing difficulty of tooth extraction to be detected radiographically. A- abnormal roots number. B- abnormal roots shape. C- caries extending into the root mass. D- pathological lesion. E- root resorption F- impaction, ankylosis, gemination.

24
Careful interpretation of the radiograph may reveal the possibility of the following complications: 1- damage to the inferior alveolar and mental nerves. 2- creation of an oro- antral or oronasal communication. 3- Fracture of the maxillary tuberosity 4- displacement of a tooth or root into the maxillary antrum. 5- retention of intra-bony pathological lesion.

27
Indications of pre-extraction radiograph 1.History of difficult extraction. 2.A tooth abnormally resistant to forceps extraction. 3.Teeth in close proximity to vital structures. 4.Any mandibular 3 rd molars or malposed canines or premolars. 5.Any tooth which has been subjected to trauma.

28
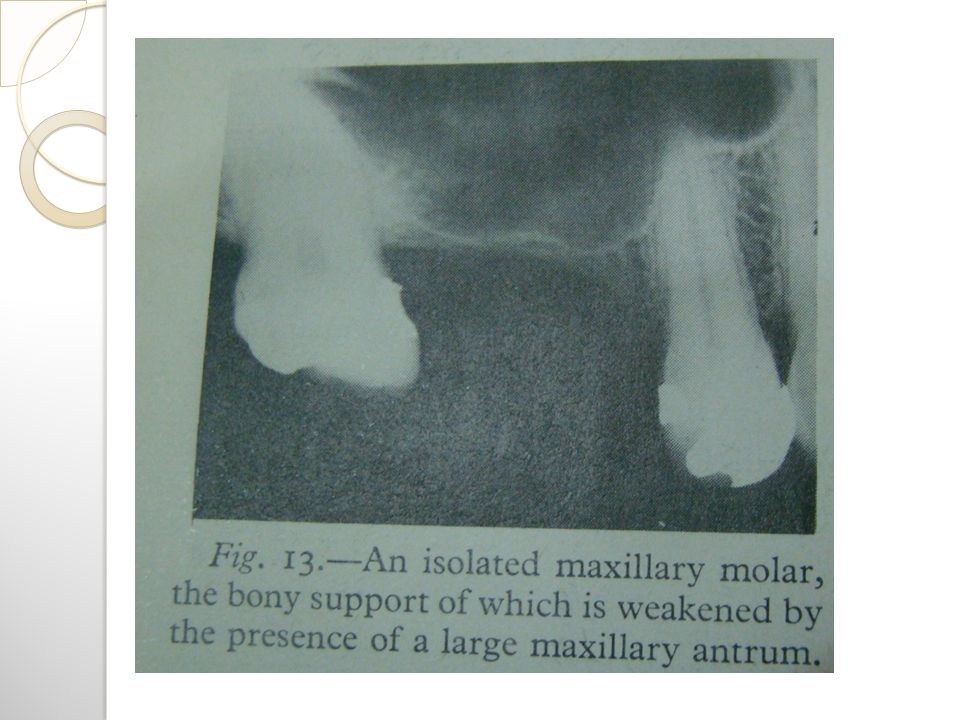
6.Any isolated maxillary molars, especially if it is unopposed or over erupted. 7.Any partially erupted or unerupted teeth. 8.Tooth with an abnormal crown shape. 9.Patients who have received therapeutic radiation.

33
Any antibiotics that are prescribed should always be taken as directed. Failure to do so can lead to the development of bacterial resistance to the antibiotic. If have any problems associated with taking antibiotics (including the development of a generalized rash or itching) should report immediately
 should report immediately.")
34
Explanation of the possible complications to the patient before the surgical procedure, it is a type of information, while explanation of the complication to the patient after they happened, it is a type of excuse.

35
Thank you

Similar presentations