Download presentation
Presentation is loading. Please wait.

1
Referrals to Palliative Care Services Medical Oncology perspective Kavi Capildeo MBBS FRCP(Edin) DM SMO, Eastern Regional Health Authority
 DM SMO, Eastern Regional Health Authority")
2
Cancer as a cause of mortality Cancer: W.H.O. estimates – ≈ 40% preventable- ∴ ≈ 60% are not –≈ 40% curable- ∴ ≈ 60% are not Trinidad and Tobago –3 rd leading cause of death (after cardiovascular disease and diabetes) Death from cancer generally not sudden/instantaneous http://www.who.int/cancer/WHA_cancer_presentation_final.pdf Accessed Oct 16http://www.who.int/cancer/WHA_cancer_presentation_final.pdf Accessed Oct 16, 201140% www.cso.gov.tt
 Death from cancer generally not sudden/instantaneous Accessed Oct 16http:// Accessed Oct 16, %")
3
Cancer mortality in Trinidad and Tobago Jan 1997- Dec 2006: 12616 deaths –Male: 6876 Female: 5740 Top 5 causes of cancer death –Prostate20% –Breast11% –Colorectal10% –Bronchus and Lung8% –Leukemia6% Elizabeth Quamina Cancer Registry Elizabeth Quamina Cancer Registry

4
Death High Low Time Function Death High Low Time Function Gradual decline e.g.Dementia, frailty Death High Low Time Function Rapid decline eg. Cancer Palliative care - trajectories Erratic decline eg organ failure Source: NHS Scotland

5
Oncology clients and palliative care What palliative care needs can oncologist meet? When should client be referred for palliative care? –What palliative care services exist in T&T? –Adequate? If not, how to fix system? When can patients receiving palliative care benefit from intervention by oncologists?

6
Oncology services in T&T National Radiotherapy Centre Regional clinics: ERHA, SWRHA, Tobago 2 private centres Radiation and medical oncologists Oncology nurses Social workers Pharmacists

7
Palliative care within Oncology Clinics Evaluation of pain and other symptoms Pain medications, other drug therapies Psychosocial support: Medical Social Worker Oncologic intervention with palliative intent –Radiation –Chemotherapy –Endocrine therapy –Targeted therapies –Palliative surgery

8
Palliative care in oncology clinic setting: limitations Limited community outreach No care facility for terminally ill in MoH service Staff have other duties –Radiation planning/delivery, chemo etc –No staff exclusively assigned to palliative/supportive care Patient/family may not perceive clinic as source of supportive care (or even interested) –“doctors can’t do anything more”
 – doctors can’t do anything more")
9
No safety net? Fall from clinic system → a hard landing for the client? ? Pressure to maintain status quo with continued efforts at chemo/RT

10
Palliative care services in TT 3 hospices –1 exclusively for cancer, 1 for HIV/AIDS –All NGO based –All in POS Community-based, nurse-led service –St. Andrew/St. David only GPs with experience in palliative care –Private sector –? <10

11
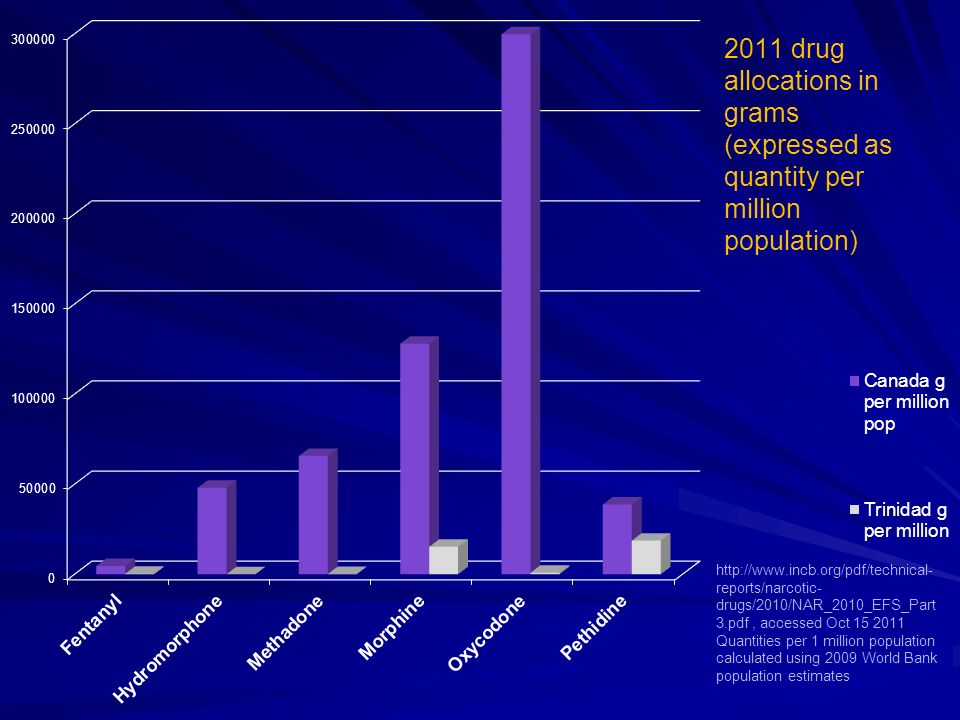
INCB and Trinidad United Nations agency Regulates international sale of narcotic drugs T&T- severe limits Chronic shortages

13
Why?

14
Palliative care in TT Limitations and challenges Community-based, public-sector services –Absent in most areas –MoH support required Hospice facilities Outpatient clinics Personnel Training and education Equipment and drugs Public awareness

15
Oncology and Palliative Care Both multidisciplinary, client centred Overlapping objectives –Quality of life and death –Symptom relief –Supportive care Complementary roles

16
Kaplan–Meier Estimates of Survival According to Study Group. Temel JS et al. N Engl J Med 2010;363:733-742. Randomized trial of early palliative care referral vs standard care in pts with metastatic NSCLC Higher QOL scores Improved mood Improved survival Less aggressive end- of-life care

17
Appropriate referrals Oncology staff, clients, families –Awareness of available services –Timely referral –Aware of referral pathways/protocols Palliative care services –Refer when appropriate for intervention to control symptoms Palliative RT: bone pain, SVCO, etc Systemic treatments

18
DEFINING PALLIATIVE CARE World Health Organisation Approach to care that ↑ QoL of patients/ families with problems associated with life threatening illness Prevention and relief of suffering –early identification and impeccable assessment and treatment : pain other problems other problems – physical – psychological – spiritual

19
Palliative care- whose responsibility? Palliative care is the responsibility of all health and social care professionals delivering care (NICE, 2004) Specialist palliative care services
 Specialist palliative care services.")
20
“When they lack the skills, confidence or expertise to cope adequately with a problem…” Uncontrolled/complicated symptoms Uncontrolled anxiety or depression Complex emotional needs involving children, family or carers Complex issues relating to physical and human environment (i.e home, finances etc) Unresolved spiritual issues around self worth, loss of meaning and hope (may include euthanasia issues) When should a Service refer to Specialist Palliative Care? Bradford & Airedale Managed Clinical Network Palliative / End of Life Care Education Programme

21
21 Specialist Palliative Care Provision Bradford & Airedale Managed Clinical Network Palliative / End of Life Care Education Programme

22
Three triggers for Supportive/ Palliative Care 1.The surprise question: ‘Would you be surprised if this patient were to die ‘Would you be surprised if this patient were to die in the next 6-12 months?’ 2.Choice: The patient with advanced disease makes a choice for comfort care 3.Clinical indicators: Specific to each of the three main end of life groups - cancer, organ failure, elderly frail/dementia Holmes, S. Practicalities of palliative care. www.bradfordvts.co.uk Accessed Oct 16, 2011

24
Supportive and Palliative Care Indicators tool (1) Ask Does this patient have an advanced long term condition, a new diagnosis of a progressive life limiting illness, or both? Would you be surprised if this patient died in the next 6-12 months? Holmes, S. Practicalities of palliative care. www.bradfordvts.co.uk Accessed Oct 16, 2011

25
Supportive and Palliative Care Indicators Tool (2) Look for one or more general clinical indicators Performance status poor or deteriorating Progressive weight loss (>10%) over past 6 months 2 or more unplanned admissions in last 6 months Patient is in a nursing /care home, or needs more care at home Holmes, S. Practicalities of palliative care. www.bradfordvts.co.uk Accessed Oct 16, 2011

26
Cancer- palliative care indicators Performance status deteriorating due to metastatic cancer and/or comorbidities Persistent symptoms despite optimal palliative oncology treatment Too frail for oncology treatment Holmes, S. Practicalities of palliative care. www.bradfordvts.co.uk Accessed Oct 16, 2011

27
Clinical indicators for terminal care Q1. Could this patient be in the last days of life? Confined to bed/chair or unable to self care Difficulty taking oral fluids or not tolerating artificial feeding/hydration No longer able to take oral medication Increasingly drowsy Holmes, S. Practicalities of palliative care. www.bradfordvts.co.uk Accessed Oct 16, 2011

28
Clinical indicators for terminal care Q2. Was this patient’s condition expected to deteriorate in this way? Q3. Is further life-prolonging treatment inappropriate? Q4. Have potentially reversible causes of deterioration been excluded? Holmes, S. Practicalities of palliative care. www.bradfordvts.co.uk Accessed Oct 16, 2011

29
Summary Palliative care for patients with cancer –Responsibility of all involved HCWs –Teamworking to improve quality of life, end- of-life care –Appropriate and timely referral to specialist palliative care services (where available) –Gaps in system need to be addressed
 –Gaps in system need to be addressed")
30
Patient Family/ Carers Palliative care team Social work, community services Oncology team

Similar presentations










 Sara Smith – Nurse Practitioner- End of Life Care.>")









