Download presentation
Presentation is loading. Please wait.

1
It’s an adventurous Journey
Billing and Coding It’s an adventurous Journey

2
Class 5 Billing, Coding and Collections
Part 1

3
Understanding Billing
Means understanding today’s healthcare system….GOOD LUCK

4
Why do you think we bill insurance?
Why do patient’s think we bill insurance? Discuss that providers perspective and patients perspective are different. Have them write down in workbook

5
Patients believe We MUST bill Insurance
That if they have insurance they don’t have to pay Its ok to NOT pay at time of service Cost must equal service Patients who do not pay for care at time of service value it much less!!

6
Provider Knows We bill as a Courtesy
We bill to reduce financial burden to patient Billing take a great deal of time We could just be cash practice We invest time and money to effectively bill for our patients to received optimum insurance benefit. Many medical practice bill once and send you to collections!

7
Billing When speaking about insurance billing for a medical office, we need to understand the language of insurance, which has its own special terminology. Here are some terms and acronyms you will need to understand. You cant bill what you don’t understand. Billing staff need to understand, anatomy, terminology, chiropractic care and have great communication skills

8
Billing Terminology Adjustment- a positive or negative change to a patient account Assignment of benefits - The patient assigns the right of payment to the doctor. Charges- The amount a patient is charged for a procedure

9
Billing Terminology Chief complaint - Primary reason for seeking care
Claim- A request to an insurance company for payment for services Co-pay - The part the patient is responsible for. It is either a percentage or a set amount. Deductible - The part the patient is responsible for paying before the insurance company becomes responsible for payment. Diagnosis - Tell what is wrong with the patient or what the doctor’s thinks is wrong. Every claim submitted must have a diagnosis. Deductible: The important thing about deductibles determining what the rules are on the individual plans. Does it apply to all charges or does it only apply to office visit and exclude diagnostic procedures. How does the deductible run? Is it an annual deductible or a calendar year deductible? Most important is for staff to verify deductible PRIOR to visit

10
Billing Terminology Explanation of Benefits- Explanation from the insurance company of why certain services were covered and others not Medical necessity - Simply put “There must be a problem that needs fixing in order for insurance companies to pay. Medical Necessity: The expected health benefits from a medical service are clinically significant and exceed the expected natural history of recovery, and the expected health risks by a sufficient margin.

11
Billing Terminology Functional Improvement Improved level of function
Meaningful relief 11. Expected health benefits include: They write this in

12
Billing Terminology Medicare - Our national health insurance program for the elderly and disabled. Part B pays for medical expenses including chiropractic adjustments. Medicaid - A state and federal program. Chiropractic is covered in some states and not others. Many pregnant women and children qualify for this program. Personal injury claims - Any bodily injury that occurs, in and about a vehicle, at a residence or place of business. Will discuss PI in detail later in the day

13
Billing Terminology Pre-authorization - Some insurance companies require prior authorization before initiating care or claim will not be paid. Pre-existing - When insurance companies limit their liability to problems that occur after the insurance takes effect. Primary insurance - The insurance company that must pay first and usual the greater portion of the care Procedure - Something that is performed in the office to diagnosis or treat the patient’s problem. Case histories, exams and x-rays are examples of diagnostic procedures. Spinal manipulations, extremity manipulations, ultrasound and back braces are examples of therapeutic or rehabilitative procedures. Primary Insurance: For most insurance companies the patients insurance is primary

14
Billing Terminology Scope of Practice - Refers to the laws that govern the rights and responsibilities in each state. Scope of Practice law defines the procedures that chiropractors can legally perform. You doctor should be familiar with what the state scope of practice is. The reason this is important to you is because you should not be billing for anything that is out of the scope of practice for your particular state. Secondary insurance - The insurance used after the primary company has paid Usual Reasonable and Customary - The UCR is an arbitrary amount arrived at by the insurance company by which insurers attempt o pay a percentage of what is usual, customary or reasonable in a given geographical region. Worker’s compensation - Any bodily injury that occurs during the course of work. The injured worked may be covered under their state Worker’s Compensation program. The injury needs to be reported to their employer's Secondary-Example Betty has Cigna and her husband has Aetna. Cigna is billing first as her primary and than Aetna is billed as her secondary **Not many providers will not bill secondary insurances if they do not have skilled billing staff…

15
You are called on to perform a wide spectrum of daily tasks.
815 You are called on to perform a wide spectrum of daily tasks. Face to face contact with patients Interaction with insurance companies Dealing with massive amounts of paperwork Complying with legislative requirements Numerous Responsibilities Biller must be great communicators (get the money/get claims paid) Must be have patience and tolerance as insurance companies love to annoy you Bill only for what procedures are performed and documented
 Must be have patience and tolerance as insurance companies love to annoy you. Bill only for what procedures are performed and documented.")
16
Why are your billing procedures so important?
Defines tasks Creates Expectation Ensures Better Outcomes We cant meet expectations for billing if we don’t know what they are! What if you get hit by the bus or retire, can someone else in office bill out claims?

17
Top Three Reasons that Patients Leave Your Office
820 Attitude of indifference of doctor or staff Misunderstanding around fees Lack of professionalism by doctor or staff Many doctor wait till last minute to know billing changes The doctor should never talk about money(aka pts will whine and not pay) Have a list of what patient owes in advance, look prepared
 Have a list of what patient owes in advance, look prepared.")
18
Procedures, procedures, procedures
Every office not using written and proper billing procedures leaves their office at risk If you have more than one person billing everyone needs to perform procedures the same Front decks needs to understand billing if that is not the billing person as they get lots of questions at time of service

19
Example-Patient Angry
CA “Ms. Jones that will be $93 for today's visit as you have a deductible that has not yet been met Patient “sighs” and gets out her checkbook CA “Thank you Ms. Jones” Patient “Your not welcome. Now I cant buy groceries this week”

20
Example-Wrong way CA “Mr. Donut your co-pay is $ 25 for today's visit” Patient “I will just pay it next time” CA “OK” ** Patient uses this excuse each visit Ask how do you handle it when an elderly person is on limited income and cant pay?

21
Example-Correct way CA “Mr. Donut your co-pay is $ 25 for today's visit” Patient “I will just pay it next time” CA “Mr. Donut, our office policy requires payment at the time of service” Patient “I don’t have it today” CA “That ok, let me have to speak with our billing supervisor and they can set up payment arrangements”

22
What is process if they refuse to pay
Key Elements Who asks for payment When do you ask What is process if they refuse to pay Its again all about procedures

23
Proper Tools National Provider Identifier (NPI) Provider number
Procedures for gathering information HIPAA compliant computer Good Copier Current coding books Many doctors try to get along without You can use the story I told in class about Florida doctor who never took license test in Florida but treated and billed patients for 2 years and was jailed!

24
Provider Numbers Single Doctor Multi-doctor Office
830 Provider Numbers Single Doctor Required to have provider numbers for all insurances that require them. Multi-doctor Office Each doctor must have his/her own individual provider number. The office has to have a group number. It is fraudulent and illegal to bill for services under the name of a provider when they did not personally provide the services.

25
Do you have written procedures to follow?
Yes That is great But are they current? NO Start working on it today

26
Why Written Procedures?
If a staff member submits bills improperly it can result in several problems: Denial of claims that were payable Loss of income Liability for fraud Increased stress Billing must know proper reasons claims can be denied Doctors need MONEY to run a practice and improper billing can ruin a doctor

27
Telephone Procedure What expectations does your staff give to patients on the phone before they begin treating with you Your billing and collection procedures start with the very first contact with the patient, usually the telephone

28
What Type of Patient is it?
New patient? Personal Injury Workers Compensation Cash/self pay Insurance Medicare If yes what category of patient? This information allows you to be ready for the patient when they arrive in your office

29
What Type of Patient is it?
840 If yes, why did they stop treating A reactivated patient Will need a new exam to be completed Most providers Might need updated X-rays Needs to be treated as new patient Over 3 years since last visit Put great emphasis that if patient has NOT been treated in 3 years they are required to re-establish as new patient By CPT definition, a new patient is “one who has not received any professional services from the physician, or another physician of the same specialty who belongs to the same group practice, within the past three years.”

30
What Type of Patient is it?
840 Should be quick visit Active patient with no changes? Will need more time Active patient with a new condition? If front desk answering phone does not ask right questions, it can set the doctor behind schedule This information allows you to be ready for the patient when they arrive in your office

31
Common Scheduling Codes
SD same day appointment Means they called in that day to schedule F/U follow up appointment ROF report of findings These are just examples

32
Common Scheduling Codes
NP new patient RE re-exam CIC change in condition NC New Condition

33
845 ELA-Go to your Boards List what you feel the top 5 five mistake are in each of these areas that affect billing; Documentation by staff Documentation by doctors Charge entries by front desk/billing Give them 15 minutes

34
9 Review List what you feel the top 5 five mistake are in each of these areas that affect billing; Documentation by staff Documentation by doctors Charge entries by front desk/billing

35
Coding books CPT Book Current Procedural Terminology
910 Coding books CPT Book Current Procedural Terminology Allows you to select the correct procedure codes for billing Updated yearly so you always need to have the current years edition in your office Only use codes within your scope of practice. Indicate you should ALWAYS have most current. Note that ICD10 is almost complete (I will go into great detail on that) The CPT and ICD-9 books include every code in existence for any type of practice.
 The CPT and ICD-9 books include every. code in existence for any type of practice.")
36
Coding books CPT Book International Classification of Disease
910 Coding books CPT Book International Classification of Disease 9 (means 9th edition Indicate you should ALWAYS have most current. Note that ICD10 is almost complete (I will go into great detail on that) The CPT and ICD-9 books include every code in existence for any type of practice.
 The CPT and ICD-9 books include every. code in existence for any type of practice.")
37
ChiroCode Deskbook In most instances, a specialty specific CPT & ICD-9 coding book will suffice. One of the best written and least expensive books available is the “ChiroCode Deskbook”. Chirocode offers best books for Chiropractors

38
Newest Update The ChiroCode Institute and the American Chiropractic Association (ACA) merged forces last year by combining the Chiro- Code DeskBook with ACA’s Chiropractic Coding and Compliance Manual. The relationship simply makes sense in terms of ensuring a universal standard for the profession to follow in the sometimes contentious and ambiguous field of coding and compliance. Just an FYI Now we have best book ever!
 merged forces last year by combining the Chiro- Code DeskBook with ACA’s Chiropractic Coding and Compliance Manual. The relationship simply makes sense in terms of ensuring a universal standard for the profession to follow in the sometimes contentious and ambiguous field of coding and compliance. Just an FYI Now we have best book ever!")
39
Do You Speak “Billing” Relevant chiropractic terminology
915 Do You Speak “Billing” Each chiropractic assistant needs to know… Relevant chiropractic terminology Relevant medical terminology For Chiropractic and Medical How to pronounce the words As you will be calling Insurances Common clinical abbreviations So you can validate Provider notes Read part in circle and corresponding text in white box

40
Cardinal Rule of Billing and Fraud Prevention
If it isn’t written, it didn’t happen! It is scary how many provider don’t document while treating, but wait till later and there is NO WAY they can remember it all

41
Documentation Basics What to write with? Blue ink Black ink
Avoid light colored pens because when you make copies it is hard to read.

42
Documentation Basics Draw a line through it and initial it.
920 Documentation Basics Do not write in pencil Do not use white out Do not scratch out FOR EMR, do not allow others to use your log in Draw a line through it and initial it.

43
Billing & Coding Basics
Only bill for services rendered Make sure you bill for services on the date they were performed

44
Billing & Coding Basics
Only bill procedures that are within the scope of practice of your doctor Make sure you have documentation for any services billed Diagnose and bill according to patient history of chief complaints and not according to doctor technique Lazy documentation leads to law suits!

45
The Good News It is fairly easy to learn how to code and document for chiropractors. Compared to other professions there aren’t that many codes that we use. WOW YOUR DONE. GREAT JOB ROCKSTAR B

49
Evaluation & Management Codes
Evaluation and management (E/M) coding isn't hard; it just seems that way.
 coding isn t hard; it just seems that way.")
50
Evaluation & Management Codes
Staff submitting the billing are liable for fraud, just like the doctor is. Understanding and meeting the requirements for proper coding will limit your liability to fraud. 945

51
Patients Perspective

52
When Are E & M Codes Used? When a significant and separate identifiable service has been performed that is different from the routine services done within the basic “Chiropractic Manipulation Treatment” (CMT) E.g , 98941, 98942, 98943
 E.g , 98941, 98942,")
53
Chiropractic Manipulation Treatment
“ CMT is a form of manual treatment to influence joint and neurophysiological function…The CMT codes include a pre-manipulation patient assessment.”

54
Code Selections Process by Key Components
Select the category and sub-category of the service provided. Determine the level of service in each component. Select the appropriate code. The most commonly used E & M codes in a chiropractic office are Office Visits. Category Sub-Category Code Range Office visits New Patient Established Patient

55
Usual E/M Service Encounters Include:
Initial evaluation Periodic re-evaluation Exacerbation or re-injury Counseling Release/Discharge from active care 950

56
Inappropriate Billing
It is not appropriate to bill an E/M code to cover an adjustment.

57
General Categories Office Visits Consultations

58
Office Visits New Patients or Established Patients

59
New Patient By CPT definition, a new patient is “one who has not received any professional services from the physician, or another physician of the same specialty who belongs to the same group practice, within the past three years.”

60
Established Patient One who has received professional services from the physician or another physician of the same specialty who belongs to the same group practice, within the past three years. When a physician is on call for or covering for another physician, the patients encounter will be classified as it would have been if seen by the physician who is not available.

61
Consultation A type of service provided by a physician whose opinion or advice regarding the evaluation and/or management of a specific problem is requested by another physician or other appropriate source. Be careful, this service is not usually provided by chiropractic offices. If a MD refers a patient to you for treatment, the visit does not qualify for a consultation code.

62
E & M Coding The E & M codes are an area where most doctors are either: Not getting paid Not billing at all Wrong coding Lost revenue Billing codes lower Up coding Fraud Billing codes Too high

63
Three Key Components Patient History Examination
Evaluation & Management Codes are based on 7 Components Three Key Components Patient History Examination Clinical Decision Making 955

64
Three Contributory Components
Evaluation & Management Codes are based on 7 Components Three Contributory Components Counseling Co-ordination of Care Nature of Presenting Problem

65
One Other Component Time Evaluation & Management Codes
are based on 7 Components One Other Component Time

66
E & M Codes The Key Components
Code selection is based on the level of service provided in each of these three key components during the office visit. New Patients and Established Patients have a varying number of these three key components, which must be met.

67
Key Component Overview
Let’s go over the 3 key components and how to choose the proper level of patient history, exam and decision-making.

68
History The subjective information received from the patient answering questions asked by the healthcare provider. We must be great listeners 10

69
History Included in a complete history:
Review of Systems (ROS) of all body parts An exam requires at least “3” vitals area measured which could include; Height Use simple wall scale Weight Use digital Temperature Rules out infection Pulse Respiration Blood Pressure Pulse ox
 of all body parts. An exam requires at least 3 vitals area measured which could include; Height. Use simple wall scale. Weight. Use digital. Temperature. Rules out infection. Pulse. Respiration. Blood Pressure. Pulse ox.")
70
History The amount of history obtained is dependent on the level of information required for the presenting problem. There are four levels of history. Each level has specific requirements that have to be met. 1. Problem Focused – Chief complaint (CC)and brief history of present illness or problem. Example: Patient complains of low back pain with spasms, never had before, no other symptoms, just occurred with no injury and no other disease
and brief history of present illness or problem. Example: Patient complains of low back pain with spasms, never had before, no other symptoms, just occurred with no injury and no other disease")
71
History There are four levels of history. Each level has specific requirements that have to be met. 2. Expanded Problem Focused – CC, brief history and problem pertinent systems review. Patient has back pain which causes some numbness, trouble ambulating and has been problematic before

72
History There are four levels of history. Each level has specific requirements that have to be met. 3. Detailed – CC, extended history of present illness, extended system review, pertinent past, family and/or social history. History of all past and present illness. System review, family history of disease, all ADL issues

73
History There are four levels of history. Each level has specific requirements that have to be met. 4. Comprehensive – CC, extended history of present illness, complete system review, complete past, family and social history. History of all past and present illness. System review, family history of disease, all ADL issues. Will include reviewing other treatment records, sometimes coordination of care, specialized testing

74
Examination The process used to obtain objective data relevant to the presenting problem. The amount of time required will be dependent on the actual clinical situation. 10 1020

75
Examination techniques include;
Tissue and tone changes Gait Inspection Of involved areas Palpation For abnormalities Auscultation To discover areas of weakness or tenderness Percussion To obtain measurable data to determine if WNL Mensuration 10

76
Medical Decision Making
Medical decision making refers to the complexity of establishing a diagnosis and/or selecting a management option. No mystical magical ball 1025

77
Medical Decision Making
There are four levels of medical decision making. Each level has specific requirements. 1. Straightforward -minimal # of diagnoses or management options, minimal or no amount and/or complexity of data to be reviewed, minimal or no risk of complications and/or morbidity or mortality

78
Medical Decision Making
There are four levels of medical decision making. Each level has specific requirements. 2. Low Complexity - limited # of diagnoses or management options, limited amount and/or complexity of data to be reviewed, limited risk of complications and/or morbidity or mortality

79
Medical Decision Making
There are four levels of medical decision making. Each level has specific requirements. 3. Moderate Complexity - multiple # of diagnoses or management options, moderate amount and/or complexity of data to be reviewed, moderate risk of complications and/or morbidity or mortality

80
Medical Decision Making
There are four levels of medical decision making. Each level has specific requirements. 4. High Complexity - extensive # of diagnoses or management options, extensive amount and/or complexity of data to be reviewed, high risk of complications and/or morbidity or mortality

81
Three Contributory Components
Counseling Co-ordination of Care Nature of Presenting Problem

82
Counseling and Co-ordination of Care
The continuous discussion of the problem, from history to exam to diagnosis and management with the patient, for patient understanding, along with coordinating necessary treatments by the assistant or to other involved parties. 1035

83
Counseling and Co-ordination of Care
In the case where visits consist predominantly of counseling and coordination of care, time is the key or controlling factor to qualify for a particular level of E & M service.

84
Nature of the Presenting Problem
A disease, condition, illness, injury, symptom, sign, finding, complaint or other reason for the encounter.

85
Nature of the Presenting Problem
Minimal – a problem that may not require the presence of the physician, but service is provided under the physician’s supervision. Self-limiting or Minor – a problem that runs a definite and prescribed course, is transient in nature and is not likely to permanently alter health status or has a good prognosis with management/compliance. Low Severity – a problem where the risk or morbidity without treatment is low; there is little to no risk of mortality without treatment; full recovery without functional impairment is expected.

86
Nature of the Presenting Problem
Moderate Severity – a problem where the risk of morbidity without treatment is moderate; there is moderate risk of mortality without treatment; uncertain prognosis or increased probability of prolonged functional impairment. High Severity – a problem where the risk of morbidity without treatment is high to extreme; there is a moderate to high risk of mortality without treatment or high probability of severe, prolonged functional impairment.

87
Chiropractic Manipulative Treatment (CMT) codes
The CMT codes cover: 5 spinal regions Cervical Thoracic Lumbar Sacral Pelvic 1040

88
Chiropractic Manipulative Treatment (CMT) codes
5 extra-spinal regions Head, including TMJ Upper extremities Lower extremities Anterior ribs Abdomen B

89
Chiropractic Manipulative Treatment (CMT) codes
There are Three Spinal CMT codes 98940: One to two spinal regions 98941: Three to four spinal regions 98942: Five spinal regions 11

90
Chiropractic Manipulative Treatment (CMT) codes
There is One Extraspinal CMT code 98943: 1 or more Extraspinal regions

91
Documentation requirements for all CMT codes
Proof the patient was in your office (sign in sheet) Date the chart entries (service date) Show a relationship between the: Presenting problem History Exam findings X-ray findings Symptoms Diagnosis
 Date the chart entries (service date) Show a relationship between the: Presenting problem. History. Exam findings. X-ray findings. Symptoms. Diagnosis.")
92
Documentation requirements for all CMT codes
Doctor’s notes (On each visit, make sure the doctor’s notes include each region of the spine and/or the Extraspinal regions adjusted) Doctor must verify their notes (sign/initial)
 Doctor must verify their notes (sign/initial)")
93
Proper CMT coding Your doctor’s technique cannot dictate the level of CMT used

94
For Example Patient presents with neck pain. A cervical exam and x-ray show a subluxation and tenderness at C2. No other findings.

95
For Example Even if your doctor’s technique is full spine, you can only bill a one area code, a 98940, due to the patient’s presenting problem and clinical documentation.

96
Documentation and Coding Billing CMT
Many doctors are billing one level of CMT for every adjustment they perform regardless of the services rendered, this is; Incorrect billing procedures Huge loss of revenue

97
Documentation and Coding Billing CMT
Code correctly If they are adjusting 1-2 areas, bill a 98940 If they are adjusting 3-4 areas, bill a 98941 If they are adjusting 5 areas, bill a 98942 And, if they are adjusting extra-spinal areas, bill a 98943

98
X-Ray Codes The decision to take x-rays of a patient should be based on their history and physical exam findings 1110

99
Code Procedure Performed
Example: 72010 is a two-view full spine study typically used for postural/biomechanical evaluation such as scoliosis 72020 – are individual studies typically used to rule out pathologies and to evaluate for regionally specific structural/biomechanical faults

100
Code Procedure Performed Use independent component codes not 72010:
72040 Cervical 72070 Thoracic 72100 Lumbar Make sure to document the medical necessity for taking films in any regions being x-rayed.

101
Supervised 97010 Hot packs/cold packs 97012 Traction, mechanical

102
Constant Attendance (Time Based)
97032 Electrical stimulation (manual) 97035 Ultrasound
 Ultrasound.")
103
Therapeutic Procedures (Time Based)
97140 Manual therapy techniques

104
Others Cold Laser ?

105
97140 Manual Therapy Three things that should be documented.
1. Technique: (manual traction, myofascial release, mobilization) 2. Location: (cervical, lumbar, shoulder) This helps to show a different area when used in conjunction with a CMT code 3. Time The minimum for one unit is 8 –23 minutes
 2. Location: (cervical, lumbar, shoulder) This helps to show a different area when used in conjunction with a CMT code. 3. Time. The minimum for one unit is 8 –23 minutes.")
106
Documentation of Physical Therapy
On time based codes document the start and end time bill in units one unit 8-23 minutes two units minutes if more than one time based service is performed the times are bundled E.g. 6 minutes ultrasound and 6 minutes attended electric stimulation performed; you can only bill one of them, not both Therapy notes should indicate where the therapy was placed Settings of the machine (when applicable) Needs to be initialed by who provided the service 1120
 Needs to be initialed by who provided the service")
107
Coding and Documentation Other Codes After Hours Services
Services requested after posted office hours in addition to basic service. Services requested between 10PM and 8AM in addition to basic service. Services requested on Sundays and holidays in addition to basic service.

108
Coding and Documentation Modifiers
Modifiers can help you improve your reimbursement They say “Pay attention, this code has been altered” Any use of modifiers must be supported with documentation

109
Modifier -25 A significant and separately identifiable management and service by the same physician on the same day of a procedure or other service.

110
Modifier -25 Same Day Services
When E & M codes are used on the same day as CMT codes You need to add the modifier -25 to the E & M codes only This indicates that the patient’s condition required a significant separately identifiable E/M service beyond the usual pre-service and post-service work associated with the procedure

111
Modifier -50 Bilateral procedure

112
Modifier - 50 73560 is the two view code for knee x-rays
If taking films of both knees, don’t just charge 2x for the views Indicate on the claim form that bilateral procedures were performed at the same session by use of the modifier –50 only on the second charge 73560

113
Modifier -51 Multiple procedures other than E & M service

114
Modifier - 51 A spinal adjustment and an extra spinal adjustment performed on the same day the 51 modifier needs to be added to the Extraspinal CMT code. It should be

115
Modifier -52 Reduced services (less than 8 min)
This is a modifier you would add to time based codes that don’t meet the coding time guidelines An example would be

116
Modifier -76 Repeat procedure by same physician
(came in AM and returned in PM) Example:
 Example:")
117
Claims,Explanation of Benefits (EOBs), Denials and Appeals
The majority of claim rejections and billing problems are due to: inaccurate and deficient coding lack of supporting documentation incomplete claims not billing for services rendered EOB 1130

118
Claims, EOBs, Denials and Appeals
The reimbursement process is a sequence of steps that starts with the chiropractor providing a service.

119
Claims, EOBs, Denials and Appeals
The steps are: Chiropractic service Documentation of the service to support your claim We’ve covered this extensively already Capture of all billable services Make sure the doctor/staff who performs the service conveys this information to the person charging for the services Make sure the person charging is properly trained and there is a system in place to not miss charging for billable services

120
Claims, EOBs, Denials and Appeals
Steps: Coding of all billable services Choose the correct CPT that accurately represents the procedure or service rendered Validate the diagnosis Link the diagnosis to the procedure code

121
Claims, EOBs, Denials and Appeals
Steps: Billing for services that are supported by documentation Make every effort to rank the procedures on a given date of service in descending value order Check modifiers Confirm the diagnosis is linked properly and is appropriate for the procedure

122
Claims, EOBs, Denials and Appeals
Steps: Collection of the portion due from the patient Payer settlement of claim

123
Claims, EOBs, Denials and Appeals
Prompt Pay Laws Each state has laws governing how and when claims are paid.

124
Claims, EOBs, Denials and Appeals
You have a prompt pay complaint if: You are a provider The claim has not been paid in the time specified by your state The claim has not been denied in the time specified by your state

125
Claims, EOBs, Denials and Appeals
No additional information has been requested on the claim The claim is not to a self-funded plan (a plan in which the employer pays health care costs directly instead of purchasing insurance)
")
126
Claims, EOBs, Denials and Appeals
After you have provided services to a patient, the next step is to send a claim to the insurance company for payment. At this point, we are assuming benefits have been assigned.

127
Claims, EOBs, Denials and Appeals
Payers often request documentation instead of paying on the claim. EOB states please send medical records so we can determine medical necessity or something to that effect.

128
Claims, EOBs, Denials and Appeals Payment for Medical Records
As long as it is not contractually prohibited, you are entitled to receive payment from the insurance company for sending out records. The insurance companies should be paying clean claims without additional information.

129
Claims, EOBs, Denials and Appeals Payment for Medical Records
You cannot receive payment if it is a Medicare or claim.

130
Claims, EOBs, Denials and Appeals
Do not file away EOBs just because they have a dollar amount on them. Always, compare the EOB to the actual charges. Many times, the EOB will not have all the charges listed and the staff will just write these off. Appeal denials as soon as possible.

131
Claims, EOBs, Denials and Appeals
Common Denials E&M code was denied when performed on the same day of service as the adjustment. This is almost always due to incorrect coding (no modifier on E&M –25) Three to four area adjustment performed, one to two areas paid. This is almost always a diagnosis issue.
 Three to four area adjustment performed, one to two areas paid. This is almost always a diagnosis issue.")
132
Reasons claims are denied
Did you verify coverage Deductible not met Did you verify at time of service Coverage no longer effective Why Non Covered service

133
Reasons claims are denied
Why Not Medically Necessary Specifically what? Need additional information Based on what? Pt reached Maximum Medical Improvement (MMI)
")
134
Claims, EOBs, Denials and Appeals
Common Denials X-rays taken: 72040 Cervical 72070 Thoracic 72100 Lumbar Often the insurance company will try to bundle these together into (radiological exam, spine, entire, survey study, AP and lateral).
.")
135
Claims, EOBs, Denials and Appeals
72010 is typically used for a scoliosis study or other postural/biomechanical evaluations. If that is what you are doing, that should be the code billed, but if you bill the other codes and they bundle it, you need to appeal it. Again, if you take cervical films, a cervical diagnosis should be linked to it. Thoracic films, thoracic diagnosis. Lumbar films, lumbar diagnosis.

136
Claims, EOBs, Denials and Appeals
Appeal it ! A two-view full spine study (72010) is typically used for postural/biomechanical evaluation such as scoliosis. Individual studies (72020 – 72220) are typically used to rule out pathologies and to evaluate for regionally specific structural/ biomechanical faults.
 is typically used for postural/biomechanical evaluation such as scoliosis. Individual studies (72020 – 72220) are typically used to rule out pathologies and to evaluate for regionally specific structural/ biomechanical faults.")
137
Claims, EOBs, Denials and Appeals
Read your EOBs carefully.

138
Claims, EOBs, Denials and Appeals
So far we have focused on what happens after you send in your claim and receive the EOB. Many times you receive nothing and need to have procedures to capture these “lost” claims.

139
Claims, EOBs, Denials and Appeals
Remember filing insurance is a service you provide for your patients. Get your patients involved early on difficult claims. State clearly in your financial policies “if claims are not paid in _____ amount of time, the patient is responsible for payment”.

140
Validation of claims

141
What does your team needs to know about billing?

142
Common errors Chiropractic assistants make

143
Super CA TIPS A

144
Increasing productivity when billing
Understanding how to organize, prioritize and simplify you’re billing procedures will make billing easier, more effective and less stressful.

145
Increasing productivity when billing
Organize-Set times for each component of billing Preparing claims Responding to requests for additional information Auditing patient accounts Troubleshooting denials Calls to insurance Patient statements

146
Prioritize Submit correct claims daily Take action immediately on denied or partially paid claims Simplify Follow procedures Make sure each member of your team is doing their part Use a to-do list

147
1

148
Why are patients with Medicare a challenge?
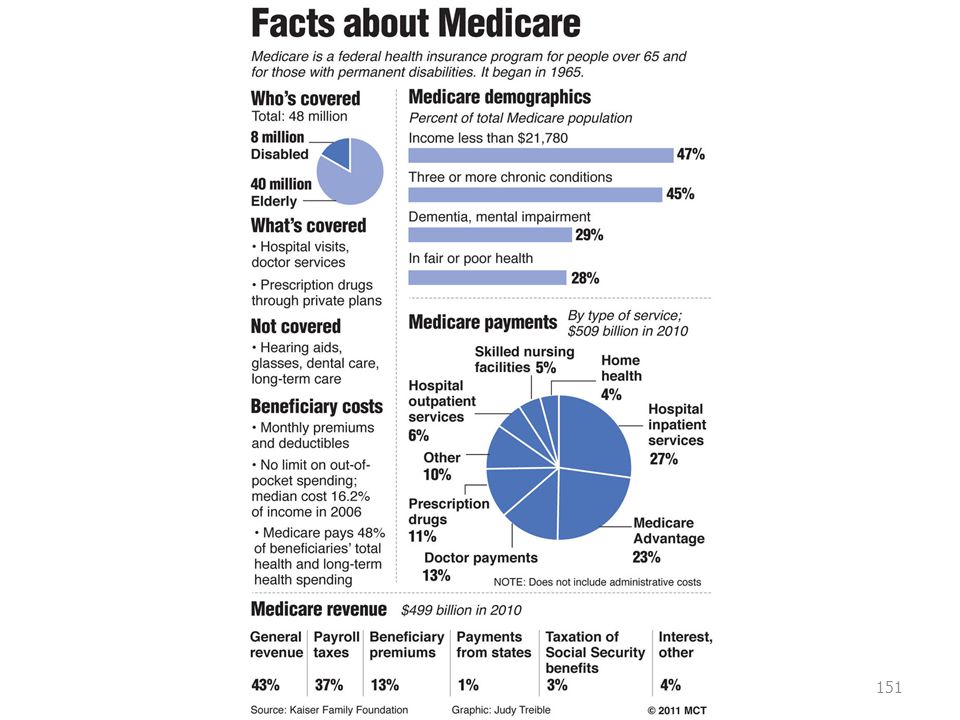
They many times need care more than other patients Recovering time is usually slower Insurance coverage is very limited Patients ability to pay is sometime a problem

149
Who is Eligible People age 65 and over.
People under age 65 who have been a disabled beneficiary under Social Security or the Railroad Retirement Board for more than 24 months. Certain government employees and certain members of their families when they are disabled for more than 29 months. People under age 65 who received continuing dialysis for permanent kidney failure or who have a kidney transplant.

150
The Medicare Program Two Parts
Part A is hospital insurance Part B is medical insurance and includes chiropractic If they don’t have Part B, they do not have chiropractic benefits.

153
Assignment Assignment refers to an agreement between the provider of services and the Medicare beneficiary.

154
Assignment When the provider accepts assignment, he or she agrees to accept the allowed amount on the covered services as payment in full The provider cannot bill the patient for or accept payment from any source in an amount that when added to Medicare’s payment exceeds the allowed amount

155
Assignment Deductible Co-insurance Statutorily non-covered charges
The patient is liable for:

156
Routinely Waiving Medicare Co-payment and Deductibles?
Routine waiver of deductibles and co-payments by charge-based providers, practitioners or suppliers is unlawful because it results in False claims Violations of the anti-kickback statute Excessive utilization of items and services paid for by Medicare.

157
Real World Violations Not having the assignment signed
Not collecting the deductibles Not collecting co-insurance Not collecting statutorily non-covered charges Keeping overpayments

158
Penalties for Violation
Loss of license Fines Jail

159
Prosecutors say chiropractor case shows fraud won't be tolerated
(AP) -- The prosecution of two chiropractors and a consultant who scammed more than $2.8 million from Medicare and private insurers sends a message that health care fraud will not be tolerated, federal authorities said Tuesday. The indictment said the men submitted or caused to be submitted false claims to private insurance companies and Medicare for tests, treatments and other services they said were performed by medical doctors who determined medical necessity. The services were performed by chiropractors trying to evade some health care benefit programs' limits on chiropractic care, federal authorities said.
 -- The prosecution of two chiropractors and a consultant who scammed more than $2.8 million from Medicare and private insurers sends a message that health care fraud will not be tolerated, federal authorities said Tuesday. The indictment said the men submitted or caused to be submitted false claims to private insurance companies and Medicare for tests, treatments and other services they said were performed by medical doctors who determined medical necessity. The services were performed by chiropractors trying to evade some health care benefit programs limits on chiropractic care, federal authorities said.")
160
Eliminating Fraud and Abuse
We have reviewed some of the common problems encountered in chiropractic offices. In your workbook you will find specifics on fraud and abuse.

161
Participating vs. Nonparticipating Physicians
Participating physicians are providers who voluntarily enter into an agreement to accept assignment for all services to Medicare beneficiaries Non- participating physicians do not accept assignment 115

162
Participating vs. Nonparticipating Physicians
Non-participating physicians can accept assignment on a claim by claim basis Have limits on charges billed to Medicare and amounts collected from beneficiaries on unassigned claims Reimbursed at 95% of the participating physician fee schedule amount on all services that could be or are paid under the physician fee schedule

163
Documentation Requirements Demonstration by Physical Examination
Two of the four following four criteria are required. One of which must be asymmetry/misalignment or ROM abnormality Pain/tenderness evaluated in terms of location, quality and intensity Asymmetry/misalignment identified on a sectional or segmental level Range of motion abnormality (changes in active, passive, and accessory joint movements resulting in an increase or a decrease of sectional or segmental mobility) Tissue, tone changes in the characteristics of contiguous or associated soft tissues, including skin, fascia, muscle and ligament
 Tissue, tone changes in the characteristics of contiguous or associated soft tissues, including skin, fascia, muscle and ligament.")
164
Documentation Requirements Patient History Documentation
Symptoms causing patient to seek treatment Family history if relevant Past health history (general health, prior illness, injuries, or hospitalization Medications; surgical history) Mechanism of trauma
 Mechanism of trauma.")
165
Documentation Requirements Patient History Documentation
Quality and character of symptoms/problem Onset, duration, intensity, frequency, location, and radiation of symptoms Aggravating or relieving factors Prior interventions, treatment, medications, secondary complaints.

166
Documentation Requirement Initial Visit
History and description of present illness Physical Examination Diagnosis Treatment Plan Date of Treatment

167
Documentation Requirements Subsequent Visits
History Review of chief complaint Changes since last visit System review if relevant Physical Exam (P.A.R.T.) Documentation of treatment given on day of visit
 Documentation of treatment given on day of visit.")
168
Documentation Requirements Treatment Phase must be Documented
Acute – When the patient is being treated for a new injury. The chiropractor is afforded the opportunity to effect improvement or arrest or retard deterioration of subluxation within a reasonable and generally predictable period of time. 130

169
Documentation Requirements Treatment Phase
Chronic -implies the condition has existed for a longer period of time and that, in all probability, the involved joints have already (set) and fibrotic tissue has developed.
 and fibrotic tissue has developed.")
170
Documentation Requirements Treatment Phase
Recurrence - A recurrence is a return of symptoms of a previously treated condition that has been quiescent for 30 or more days. This may require the reinstitution of therapy.

171
Documentation Requirements Level of Subluxation
The precise level of the subluxation must be specified by the Chiropractor to substantiate a claim for manipulation of the spine. Areas of the spine: Neck – Occiput, Cervical, C1 & C2 Back – Thoracic/dorsal, Costovertebral, Costotransverse Low Back – Lumbar Pelvis – Ilia (left & right) Sacral – Sacrum, Coccyx
 Sacral – Sacrum, Coccyx.")
172
Documentation Requirements Level of Subluxation
Two ways in which the level of subluxation may be specified: Exact bones (e.g. L5, L4, etc.) Area (e.g. Lumbo-sacral, sacro-iliac)
 Area (e.g. Lumbo-sacral, sacro-iliac)")
173
Coding Guidelines The Diagnosis
The level of the subluxation must be specified on the claim and must be listed as the primary diagnosis. The neuromusculoskeletal condition necessitating the treatment must be listed as the secondary diagnosis. All ICD-9 diagnosis codes must be coded to the highest level of specificity, (4th or 5th digit) and the primary diagnosis must be supported by x-ray or documented by physical examination.
 and. the primary diagnosis must be supported by x-ray or documented by physical examination.")
174
Coding Guidelines The Diagnosis
CMT If you are doing a 5 area adjustment, to legally bill, you would have to have 10 diagnoses in the record 230

175
Converting A Medicare Patient to Wellness Care
When your Medicare patient has been under care and their condition is stabilized and no functional improvement is expected, it is time to convert them to a cash paying wellness care patient Medicare law requires you to continue filing claims, coded correctly, that show you are providing maintenance care

176
Wellness Care to Symptom Care
Remind the patient that if they have an exacerbation or a new condition, they need to notify you. At this point Medicare may pay again with proper documentation and coding. This does not guarantee coverage. 140

177
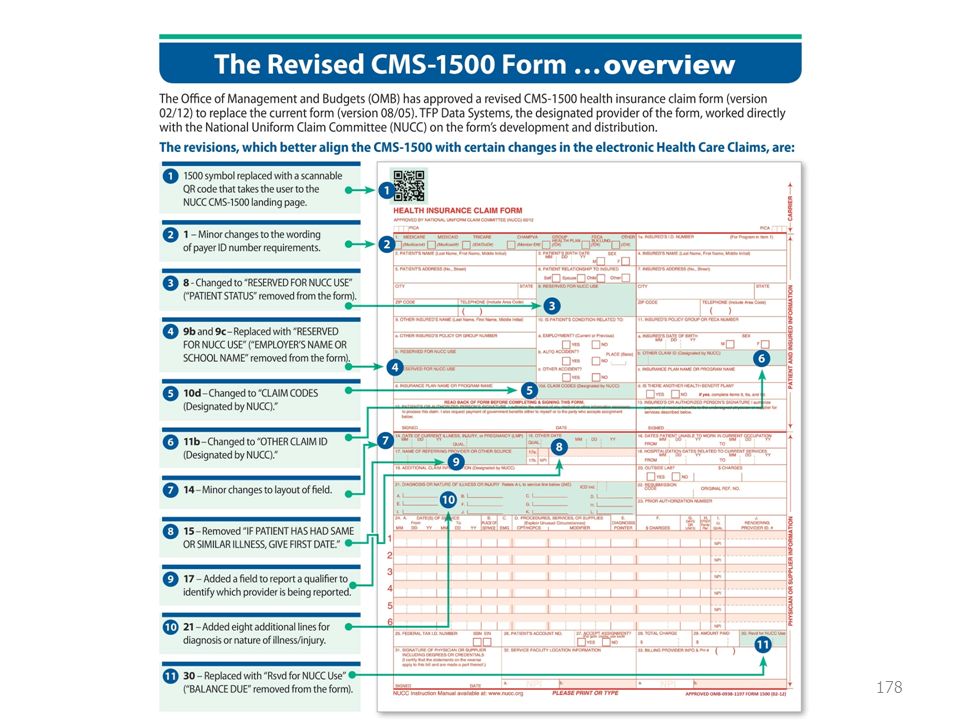
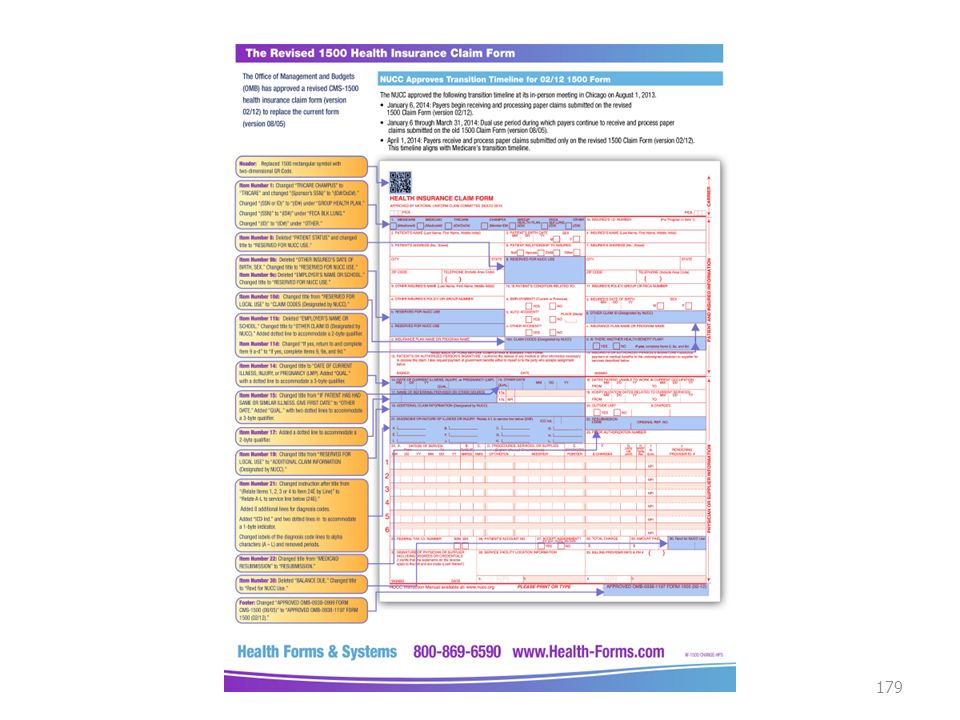
CMS-1500 Your workbook contains the Medicare line by line instructions for filling out this form 245

180
Primary Care Changes Effective Jan. 1, 2015, Medicare began paying for chronic care management (CCM), recognizing the value that primary care brings to health care
, recognizing the value that primary care brings to health care.")
181
Every office Needs to Know
Helpful Tools Every office Needs to Know Go ROCKSTAR 230

182
This is Scary!

183
10 Tips for billing success in your office
Update as needed Create a procedure manual Touch each area daily Set times for each component of billing Have in-service Train all staff on billing basics Share with team Print AR reports and follow up .99 cents well spent Have a continual to-do list 230

184
10 Tips for billing success in your office
5 random-monthly Audit Files And stick to it Set office policy for payment Or no money DON’T let patients run the office Errors occur when hurried Take the time to do things correctly Motivate team Set rewards for achieving set goals Continue to drive home procedure, procedure, procedure!

185
Procedures Continually update Review your front office procedures If yes do they read and sign it? Do they get a copy? Do you provide a financial or billing policy? If not why? Do you enforce the payment rules? In past 12 months? How many front desk CA’s Does the doctor discuss payment with the patient? On last bullet if doctor talk money, they wont get paid, it slows down care and doctor should always refer billing question to staff who handle this

186
Action Steps Find out balances on all patients
Incorporate financial review in staff meetings Organize your work area Actually read the code descriptions Order your 2015 coding book Find out and write down how much your office wrote off last year Make a list of all past due accounts Find out balances on all patients They are key factors 240

187
Insert Example Financial

188
Helpful Tips Set times for each component of billing Hurry=error
Have In-service Train all staff on billing basics Review with team Print AR reports and follow up DON’T let patients run the office Set office policy for payment Motivate team Set rewards for achieving set goals But you cant give staff the impression office is JUST about money

189
Just Think Asking might equal payment
Knowing how to turn a not to a yes for payment is Key Be prepared in advance for most common excuses for non payment Staff have to be training to ask for payment at time of service If they say no, be persuasive Common excuses include, forgot checkbook, lets wait for insurance, and I just don’t have it 245

190
Learning Activity Get with your group at your board
As a patient, list 5 reasons you would refuse to pay for service at the end of an office visit? 255

191
Review-Learning Activity
As a patient, list 5 reasons you would refuse to pay for service at the end of an office visit? 305

192
Financial Report of Findings

193
Financial Report Of Findings
We have talked a lot about your procedures, your coding, your documentation and determining your fees All of these are integral components, which will enable you to clearly explain your financial policies and expectations to your patients Financial ROF is key to patient understanding costs associates with care 315

194
Financial ROF Survey after survey shows a major cause of patient attrition is misunderstandings related to financial obligations You would not buy a Porsche and have them send you bill

195
What happens during the ROF
After doctor discusses care recommendations staff reviews financial aspect Not all practices use these

196
Financial Report of Findings Detailed Explanation
Complete this before your financial consultation with the patient. Patient & Insurance information Fill in the lines based on the doctors treatment plan. Have your fees preprinted on form Run the math Total it

197
Financial ROF Be very thorough Patients should feel informed
Collection %’s will be higher when your patients are informed of their financial obligations and held accountable for payments

198
What’s Next? Follow-up Financials
Re-financial each patient after every visits You want to make sure Patient is paying as agreed The insurance is paying as it was quoted The patient is made aware of any financial ramifications of any treatment variations that may have occurred Doctors many times stop treating when patients refuse to pay

199
Learning Activity What Can You DO???
List what do you need to do to improve your billing processes? If you would change just two things about your collection process what would they be? 325

200
Learning Activity What Can You DO???
List what do you need to do to improve your billing processes? If you would change just two things about your collection process what would they be? 335

201
2016 Challenges Are you Ready 345

202
Increasing prices??? When was the last time you increased costs for your services? When is the best time to increase? Are you getting hit with Usual Customary & Reasonable(UCR) reductions? Best time to increase fees if all, not right after Christmas when pts are broke
 reductions Best time to increase fees if all, not right after Christmas when pts are broke.")
203
Budget How much does it cost to run your practice? Payroll
Overhead expenses Clinical supplies Technology Upgrades The cost of running a practice today is at an all time high, due to increasing need for technology

204
Staffing How much staff do you need
If your staff working 100% of their potential How to you know?? Do you check on them and evaluate them

205
HIPAA updates Training Updating forms
Making sure all patient sign a consent

206
Give staff more Keep them on treatment plans Flex schedules
Lunch once in a while Motivated staff, motivated patients

207
Reduce Credit card fees
Shop your credit card vendors Sam's offers monthly flat rate

208
Demographics Keep updated Phone Email Cell Emergency contact Address
Employer Make them show proof of insurance This allows you to easily contact patients is there is a balance

209
Tips for effectively training your Front Office Staff on Collections
Select Staff Written procedures Show Them Observe Them Provide Input Follow-up Every Step Matters 355

210
1st Choice 2nd Choice Select Staff be suited for position
1st Choice is the one who can handle stress, communicate well, stay focused 2nd choice work only when 1st choice is off work or quits

211
Imagine if you just made up processes as you went along. SCARY
Written Procedures Dictate Actions Drive Success Control Income Reduce Error Imagine if you just made up processes as you went along. SCARY

212
What to do if no payment received
How to collect Show them To Collect When Have a plan What to do if no payment received Don’t expect staff to KNOW the right way

213
Observe Actions Reactions Non-Verbal Communication We learn by observation, even if they have been there for years, people tend to slack over time 4

214
Where They Can Improved
Provide Input What They Did Well Any Steps Missed Where They Can Improved Positive Comments Positive support

215
Its never ends if you’re a great manager
Follow-up Daily Weekly Monthly On-Going Its never ends if you’re a great manager

216
Your Biggest Challenge in Training Is Managing Change!
ICD/CPT Codes Fee Schedules State and Federal Laws Insurance Plans Insurance is like food, there is always something newer, different and challenging

217
Billing Leader 1040 Is air traffic control, look away and your money flow crashes and burns Effective offices have one individual who is considered the team lead. 410

218
Specific Duties and Responsibilities:
1. Enter charges daily for Current days office visits To be done daily If you wait until the next day the date of service and dates of chart not may not matching depending on computer system This is bad as data of service (DOS) billed and chart note data must match
 billed and chart note data must match.")
219
2. Prepare daily deposit Should be completed by 1pm daily from previous day Any discrepancies from front desk should be addressed Have a process for money flow to ensure all money is deposited

220
3. Monthly review of special procedures performed in office
Review x-ray log Review product log Don’t leave money on the table

221
Daily from incoming mail
4. Post payments Daily from incoming mail Notify office manager of an contractual discrepancies Many billing systems auto post payments electronically

222
5. Oversees daily operation of billing department
Ensure accuracy and timeliness in all areas of billing 6. Coordinates revisions as needed to procedure codes to obtain correct reimbursement, identifies and resolves discrepancies. This need to be kept current If any book or resources are needed inform Office Manager 420

223
7. Patient account reviews in office
8. Demonstrate a thorough understanding of and oversees all aspects of coding functions To include monitoring and interpreting insurance reimbursements Implementing procedures that ensure optimum reimbursement and compliance with regulations.

224
9. Reports due 10. Collection accounts Credit balance report
Total AR without credits Total AR with credits 10. Collection accounts Patient name Date sent to collections Starting Balance Current balance

Similar presentations






 Use 99211 Many physicians and coders still struggle with.>")








 Codes: Terminology Review contracting with insurance Review old and new CPT’s Summarize.>")


 APA CPT Alternate.>")



