Download presentation
Presentation is loading. Please wait.

1
Anaesthesia for intracranial vascular surgery Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab.DCA, Dip. Software statistics,Phd (physio) Mahatma Gandhi Medical college and research institute, puducherry, India
, Dip. Diab.DCA, Dip. Software statistics,Phd (physio) Mahatma Gandhi Medical college and research institute, puducherry, India.")
2
What is it ?? A localized dilation or ballooning of blood vessels Dr SPS

3
Incidence and sites Incidence : 1 to 6% Incidence of ruptured aneurysm: 12/100,000 Age: any age, peaks 40 - 60. Sex: M/F 2:3 Sites : 30% ICA 40% ACA( Anterior Communicating) 20% MCA 10% Vertebro-basilar systems
 20% MCA 10% Vertebro-basilar systems.")
4
Anterior – 85 % 85 %

5
Types Berry (pedunculated) Fusiform Dissecting
 Fusiform Dissecting")
6
Mostly asymptomatic Subarachnoid hemorrhage (SAH) due to aneurysmal rupture –Lethal event: 25% don’t even get to the hospital –In hospital mortality rate up to 50% –Most survivors have permanent disability Size – 24 mm Neuronal injury due to bleed Vasospasm Rebleeds
 due to aneurysmal rupture –Lethal event: 25% don’t even get to the hospital –In hospital mortality rate up to 50% –Most survivors have permanent disability Size – 24 mm Neuronal injury due to bleed Vasospasm Rebleeds")
7
The three main predictors of mortality and dependence impaired level of consciousness on admission, advanced age, and large volume of blood on initial cranial computed tomography

8
Clinical features Incidental finding if un ruptured Hematoma and edema Ruptured: sudden severe headache “worse headache of my life”, nausea, vision impairment, vomiting, & LOC Hydrocephalus- blood clots on Subarachnoid granulations & ventricles ↓ CSF absorption & obstruct CSF drainage Increased ICP, stroke Lethal event: 25% don’t even get to the hospital

9
Hunt and hess scale 2 Mo rtal ity 35 %

10
Fischer - CT scan based features

11
World federation of neuro surgeons

12
Vasospasm- 13.5% cause of mortality & morbidity. Most feared complication of SAH Occurs 1 to 2 weeks following initial hemorrhage Patho physiology not well understood Blood in SAS→ inflammation → entrapped macrophages and neutrophils → endothelins & free radicals → vasospasm → stroke New onset neuro signs

13
Vasospasm Magnetic resonance angiography (MRA) Ct angiography Transcranial doppler ultrasonography (TCDs) Intra-arterial digital subtraction angiography GOLD STANDARD but invasive
 Ct angiography Transcranial doppler ultrasonography (TCDs) Intra-arterial digital subtraction angiography GOLD STANDARD but invasive")
14
Nimodipine Improve outcome in vasospasm Oral 60mg 4Hly, max dose 360mg for 21 days IV 1mg/hr during the first 6 hrs, increase gradually to max 2mg/hr Maintain SBP 130-150mmhg risk of hypotension central line to avoid thrombophlebitis.

15
Hypertension, hypervolumia,hemodilution ( 3 H ) SBP 120-150 mmhg in unclipped 160-200 mmHg in clipped aneurysm. CVP 8-12mmHg HCT 30-35% Intraarterial papaverine

16
Rebleeds The overall incidence of re bleeding is 11%. 1 – 12 days Deterioration 70 % mortality Prevention BP maintain, seizure control,ICP maintenance

17
What should we do ??

18
From outside

19
Or from inside Thrombogenic – new intima will grow inside

20
When to touch 0- 3 days 4 – 10 days Controversial

21
Preoperative evaluation Careful medical history Physical examination Baseline BP, fluid status Hyponatremia (brain natriuretic peptide) Prolonged bed rest runs the risk of atelectasis and pneumonia. CNS examination

22
Pre op work up Investigations --- for the diagnosis Routine + ECG, ECHO, CxR, coagulation profile T wave inversion & ST depression (most common), Prolong QT (atrial & ventricular dysrhythmias) -- catecholamine surge Pregnancy test ( pregnant ruptures the aneurysm) Talk to the surgeon also
, Prolong QT (atrial & ventricular dysrhythmias) -- catecholamine surge Pregnancy test ( pregnant ruptures the aneurysm) Talk to the surgeon also")
23
Neuro radiology Cerebral Angiogram Site of the aneurysm Prepare for intraop positioning, surgical exposure & monitoring CT scan Amount of subarachnoid blood in the basal cisterns is good predictor of delayed vasospasm Increase ICP from IC haemorrhage, hydrocephalus or cerebral oedema TCD facilitate vasospasm management.

24
Premedication Calcium channel-blocking drugs, anticonvulsants, and steroids are continued. No sedatives No narcotics Possible acid aspiration prophylaxis preoperative administration of erythropoietin in elective cases might reduce injury from reversible ischemia during temporary clipping

25
Cardiac evaluation Elevated Troponin 17-28% Elevated CKMB 37% Echo LV dysfunction Syndrome of neurogenic-stunned myocardium Cardiogenic shock pulmonary oedema But OK – don’t postpone – no added treatment

26
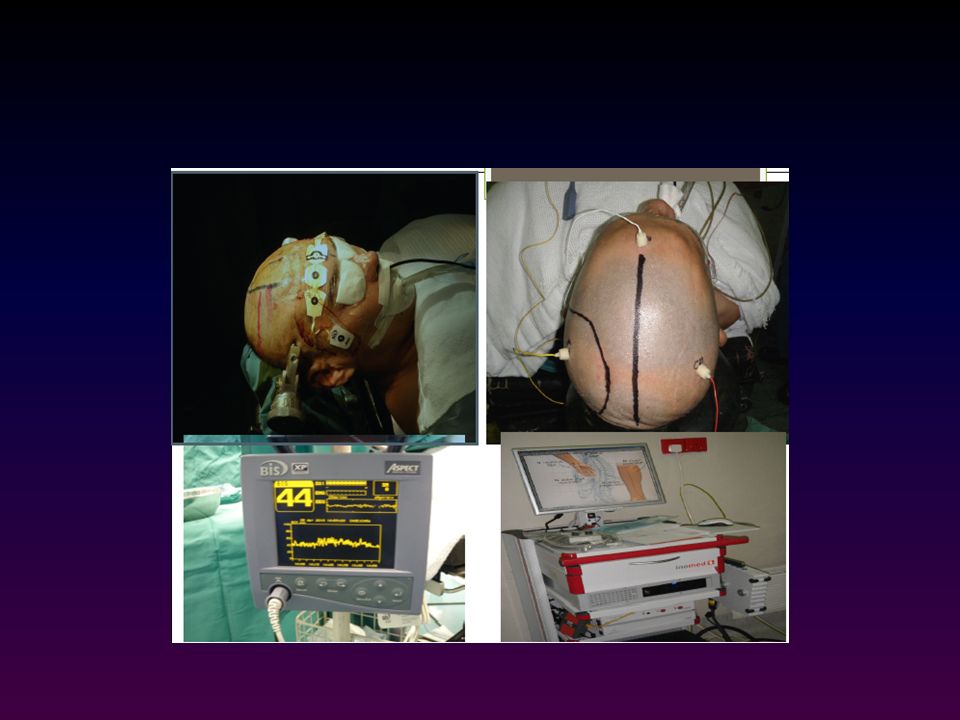
Monitoring 1.CVS : ECG, Arterial line (IBP), CVP (cubital fossa) 2.RESP : SpO2, End tidal CO2, oesophageal stethoscope 3.NEUROMUSCULAR : Train of 4 (by PNS) (it is essential that these patients do not move) 4.CNS : Either BIS/EEG or EPs 5.RENAL : U/O, all these patients are catheterised the U/O provides an indication that the diuretics are working
, CVP (cubital fossa) 2.RESP : SpO2, End tidal CO2, oesophageal stethoscope 3.NEUROMUSCULAR : Train of 4 (by PNS) (it is essential that these patients do not move) 4.CNS : Either BIS/EEG or EPs 5.RENAL : U/O, all these patients are catheterised the U/O provides an indication that the diuretics are working")
27
Monitoring brain temperature Intermittent arterial blood gases, glucose, electrolytes, osmolality, hematocrit, urine output EEG evoked potentials – duration of occlusion? IV anaesthetics better Jugular bulb oxygen monitoring can also be helpful in patients at risk for global cerebral ischemia.

29
Can we place the leads ?? SSEP monitoring has mostly been used during aneurysm surgery in the territory of both anterior and posterior cerebral circulation, BAEP monitoring has been used during operations in the territory of the vertebral- basilar circulation.

30
Anesthetic Management Goals Decrease transmural pressure gradient Don’t try to control ICP much !!

31
Goals maintaining adequate CPP and cerebral oxygenation; preventing the development of a “tight” brain from cerebral edema or vascular engorgement.

32
Induction !!!

33
Induction Thio – 5- 6 mg/Kg Smooth induction – narcotics IV lignocaine or esmolol Scoline – OK Vecuronium – complete muscle relaxation Local and fentanyl for pinning Normotension

34
Maintenance Nitrous ??, fentanyl, propofol - infusion BP should be kept within previously defined limits according to the patient’s baseline BP. Target is usually 20 mm Hg below baseline Prior Beta blockade may help Mannitol (1.5 gm/kg) combined with Frusemide (0.3mg/kg) is given to shrink the brain
 combined with Frusemide (0.3mg/kg) is given to shrink the brain.")
35
Crucial times Securing of head with Mayfield pins Skin Incision Periosteal Flap elevation and Bone cutting. Narcotic, propofol, Local

36
The basics of brain slackness crucial for safe surgical dissection to proceed. implement moderate hypocapnia (PaCO2 25– 30 mmHg); elevate the head position; Add diuretics and mannitol; Drain spinal fluid; Avoid cerebral vasodilators
; elevate the head position; Add diuretics and mannitol; Drain spinal fluid; Avoid cerebral vasodilators.")
37
BP ?? !! Before clipping – get down the BP After clipping - increase to just above baseline is acceptable – 10 minutes Hypothermia – not acceptable – vasospasm is more common

39
Intra op problems

40
Coiling problems 1. The aneurysm may rupture with the angiographic manipulation 2. Secondly part of the coil could embolise out of the aneurysm into a more distal artery 3. The thrombus formation may extend out of the aneurysm and cause thrombus formation in the feeding vessels 1. Propofol or Thio 2. No vasodilators 3. Control angiographically 4. Rarely done with IV sedation

41
Aneurysmal rupture 11% of patients with previously ruptured aneurysm (compared with an incidence of 1.2% in previously un ruptured aneurysms). Maintain fluid and BP ?? Clamp before and after the aneurysm

42
Reversal The patient is not extubated until they are awake and breathing well BP should be controlled with Propofol or Narcotics infusion Further agents to control BP (Beta blockers) during extubation might be used if infusions are found unsatisfactory
 during extubation might be used if infusions are found unsatisfactory")
43
Post op problems Neuro deficits – new Then do CT scan If normal Do angio for vasospasm Vasospasm Rebleeds Infarction Fluid status Urine output Hyponatremia

44
Summary Worst headache ( neuro, vasospasm, rebleeds) Incidence ( impending doom!!) Hunt, Fischer WFNS Ecto and endo Pre op – CNS, general, investigations Induction – maintenance - recovery Post op monitoring
 Incidence ( impending doom!!) Hunt, Fischer WFNS Ecto and endo Pre op – CNS, general, investigations Induction – maintenance - recovery Post op monitoring")
45
Thank you all

Similar presentations

 Prof. Dr. Leónidas M. Quintana Prof. Dr. Leónidas M. Quintana Department.>")












, Dip. Diab.DCA, Dip. Software statistics PhD (physio) Mahatma gandhi medical college and.>")





