Download presentation
Presentation is loading. Please wait.

1
Issues in the Design and Implementation of Pay-for-Performance Programs Issues in the Design and Implementation of Pay-for-Performance Programs Gary J. Young, J.D., Ph.D. Professor and Director Northeastern University Center for Health Policy and Healthcare Research Boston, MA Presentation for Agency for Healthcare Research and Quality, Annual Meeting September 20, 2011 Financial support from the Agency for Healthcare Research and Quality and the Robert Wood Johnson Foundation Investigator Award for Health Policy Research

2
Design and Implementation Issues Multi-year study of over 70 provider organizations with quality-related incentive arrangements. Multi-year study of over 70 provider organizations with quality-related incentive arrangements. Surveys of Physicians Interviews with senior leaders from physician organizations and hospitals Analysis of Clinical Data

3
Design and Implementation Issues Selecting unit of accountability Managing provider attitudes toward pay-for-performance program

4
Unit of Accountability Individuals Organizations Teams (within or across organizations – e.g., ACOs)
")
5
Interviews with Senior Leaders from Physician Organizations and Hospitals Telephone Interviews and Site Visits Setting # Senior Leaders Massachusetts26 California37 Michigan10

6
Interviews with Senior Leaders General attitudes and issues: –Quality incentives (better than utilization) –Adequacy of dollars (new or old money) –Awareness and involvement of physicians (grass roots vs. system engineering) –Internal distribution of financial rewards (where individual physicians were not the unit of accountability) -- $ individual performance on P4P criteria -- $ individual performance on non-P4P criteria -- $ equally independent of performance -- $ retained at group level for investment (unit of accountability issue)
 –Internal distribution of financial rewards (where individual physicians were not the unit of accountability) -- $ individual performance on P4P criteria -- $ individual performance on non-P4P criteria -- $ equally independent of performance -- $ retained at group level for investment (unit of accountability issue).")
7
Interviews with Group Practice Executives “We have a point system, but I would not classify that under the heading of necessarily a quality system. I’d call it more of a participation system. I think the outcome spills over a little into quality because again, the camaraderie and the communication improve and that’s always a good thing when PCPs are talking to specialists, interfacing more….”

8
Incentives and Unit of Accountability Individual Provider Individual Provider Efficiency Physician Organization of ofIncentive Hospital Hospital Investment in infrastructure

9
Provider Attitudes Theoretical Perspectives: Self Determination Theory Professional Control

10
Interviews with Senior leaders “ Plans just throw some money in our way and think we will notice and pay attention. They do not seem to understand that our physicians have deep concerns about what strings are attached. We are always worried about the hidden agenda and what a particular incentive opportunity means for our future.” “ Plans just throw some money in our way and think we will notice and pay attention. They do not seem to understand that our physicians have deep concerns about what strings are attached. We are always worried about the hidden agenda and what a particular incentive opportunity means for our future.”

11
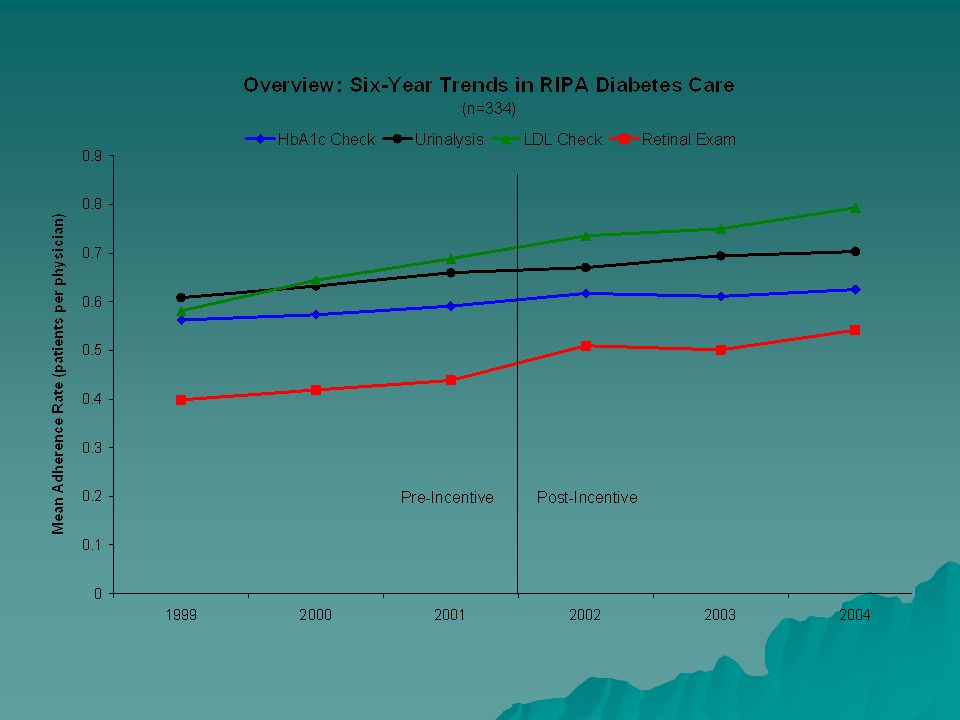
Attitudes and Responsiveness to Financial Incentives Study Setting: Physician network (IPA) in Rochester NY. –Implemented tournament-style P4P program for diabetes care –> 300 PCPs –Quality measure: Percentage of expected number of diabetic exams/screens (LDL, 2 HbA1c, urinanalysis, eye exam) conducted. –Financial incentive: 50 to 150% of withhold payment –Potential payout up to about $3,000 for diabetic component Survey of physicians at Baseline –Approximately 335 physicians surveyed –Approximately 48% response rate –No performance differences between respondents and non-respondents
 conducted. –Financial incentive: 50 to 150% of withhold payment –Potential payout up to about $3,000 for diabetic component Survey of physicians at Baseline –Approximately 335 physicians surveyed –Approximately 48% response rate –No performance differences between respondents and non-respondents.")
12
Measurement of Attitudes Five-point, multi-item Likert scales Autonomy: “The incentive system interferes with my autonomy for how I care for patients.” (reverse scaled) Goal importance: “This financial incentive is tied to a quality target that is clinically meaningful for diabetic patients.”
 Goal importance: This financial incentive is tied to a quality target that is clinically meaningful for diabetic patients.")
17
Summary Points The unit of accountability carries possible tradeoffs between infrastructure investment and power of incentives. Provider attitudes toward incentive programs may be an important moderator of an incentive program’s success. Attitudes among providers toward same incentive program may vary markedly. –Identify providers with negative attitudes –Create opportunities for providers to have input into program design/implementation

Similar presentations




 Boston University School of Public Health and Department of Veterans Affairs Dan Berlowitz, MD, MPH Matthew Guldin, MPH.>")

















