Download presentation
Presentation is loading. Please wait.

1
Department of Pathology
Biliary Tract Kimiko Suzue MD, Ph.D. Department of Pathology

2
Biliary Tract Extrahepatic biliary tract Intrahepatic biliary tract
Gallbladder Cystic duct Common hepatic duct Common bile duct Intrahepatic biliary tract

3
Biliary Disease Gallbladder Disorders Extrahepatic Bile Duct Disorders
-Cholelithiasis -Cholesterolosis -Cholecystitis Extrahepatic Bile Duct Disorders -Choledocholithiasis -Cholangitis -Biliary Atresia -Choledochal cysts Tumors

4
GALLBLADDER Contraction of the muscle induced by cholecystokinin
Storage and concentration of bile

5
Gallbladder Gallstones (cholelithiasis)
Afflict 10% of adult population in Western countries Costs of management: $6 billion a year 20 million patients are estimated to have gallstones totalling several tons Made of cholesterol, bilirubin and calcium salts with different concentrations

6
Cholelithiasis In West, >90% are cholesterol stones
Usually radiolucent (10% radiopaque due to calcium) Risk factors: -Native Americans -Women > Men -Advancing Age (25-30% of people over 80) -Estrogenic influence Pregnancy, Oral contraceptives -Clofibrate -Obesity -Gallbladder stasis (neurogenic or hormonal) -Hereditary (bile acid metabolism)
 Risk factors: -Native Americans. -Women > Men. -Advancing Age (25-30% of people over 80) -Estrogenic influence. Pregnancy, Oral contraceptives. -Clofibrate. -Obesity. -Gallbladder stasis (neurogenic or hormonal) -Hereditary (bile acid metabolism)")
8
Cholelithiasis Pigmented bilirubin stones
Usually radiopaque (calcium bilirubinate) Risk factors: -Chronic hemolytic states (increased bilirubin in bile) Sickle cell, hereditary spherocytosis, cardiac valve replacement, malaria) -Ileal disease (bile salt malabsorption) Crohn’s disease, bowel resection -Biliary tract infection/infestation Ascaris lumbricoides, Clonorchis sinensis -Liver disease (alcoholic cirrhosis)
 Risk factors: -Chronic hemolytic states (increased bilirubin in bile) Sickle cell, hereditary spherocytosis, cardiac valve replacement, malaria) -Ileal disease (bile salt malabsorption) Crohn’s disease, bowel resection. -Biliary tract infection/infestation. Ascaris lumbricoides, Clonorchis sinensis. -Liver disease (alcoholic cirrhosis)")
10
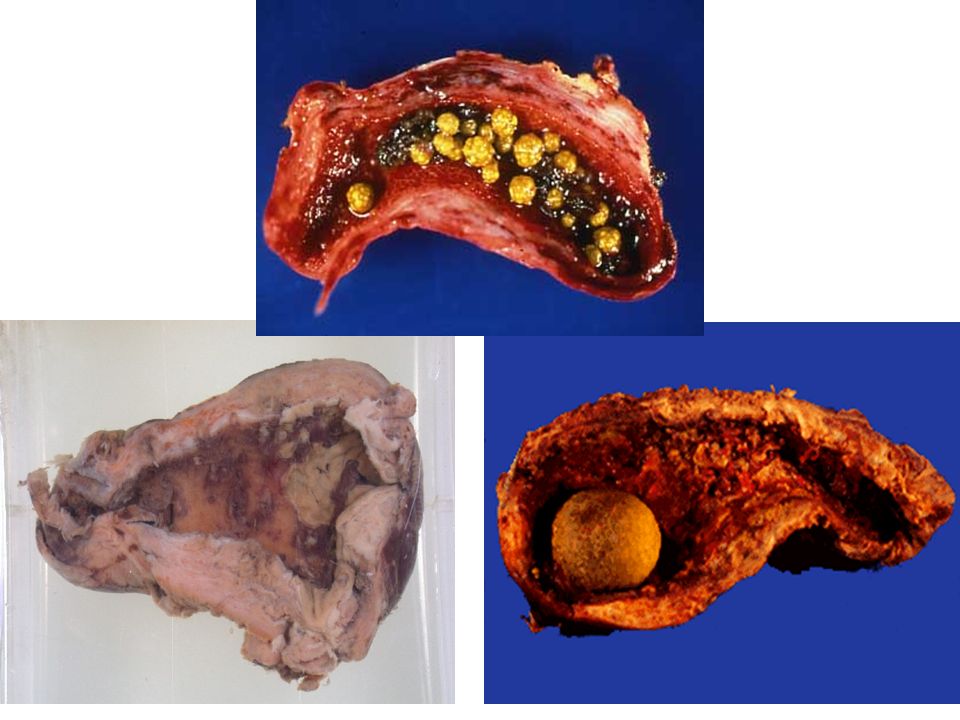
Cholelithiasis Hepatolithiasis Choledocholithiasis

11
Cholelithiasis Asymptomatic: 70% Obstruction: Biliary Colic
Spasmodic right upper quadrant pain Symptoms are relieved if stone passes Infection: Cholecystitis, cholangitis Acute Pancreatitis Gallbladder cancer Principal therapeutic modality: Laporascopic cholecystectomy (late 1980’s)
")
12
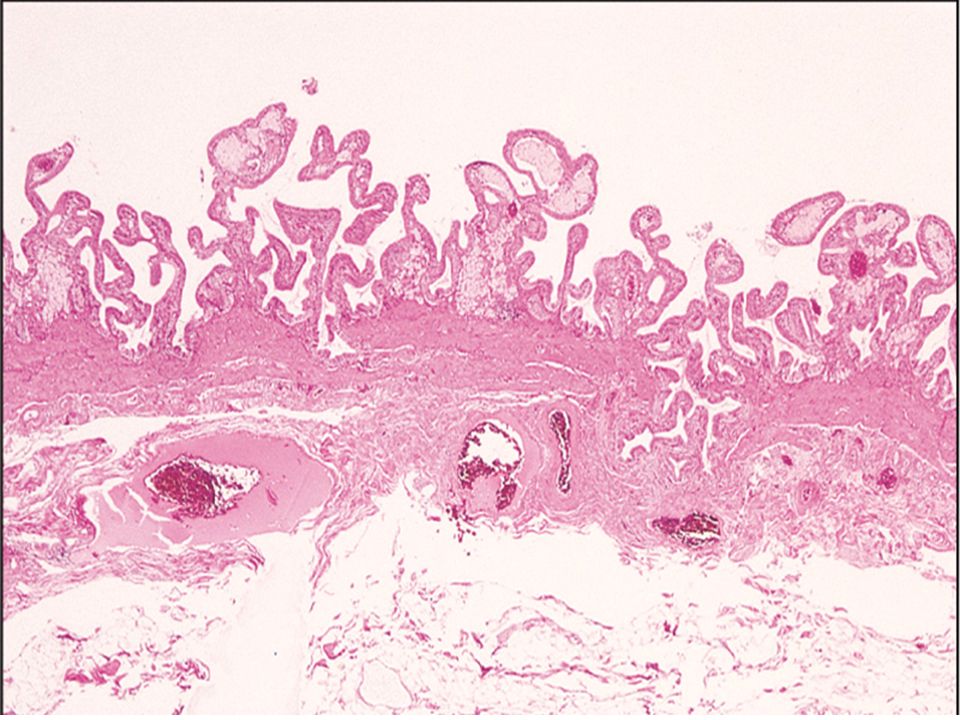
Cholesterolosis Aggregates of lipid-containing macrophages in lamina propria of gallbladder Debated clinical relevance “Strawberry gallbladder”

13
Cholesterolosis

14
Polypoid cholesterolosis
Abundant foamy macrophages forming polypoid excrescences

15
Cholecystitis General Features
Present in autopsy series in half of the population Female, obese, multiparous, 5th and 6th decades Acute (Chemical irritation and inflammation) Suppurative (Empyema, purulent contents) Emphysematous (clostridia and coliforms) Gangrenous (Necrotic) Chronic
 Suppurative (Empyema, purulent contents) Emphysematous (clostridia and coliforms) Gangrenous (Necrotic) Chronic.")
16
Cholecystitis Clinical Picture
Acute: RUQ pain referred to right shoulder Rigidity of abdominal wall (RUQ) Fever, nausea, vomiting, leukocytosis Jaundice (25% of cases) Increased WBC count Increased serum alkaline phosphatase (duct damage) Chronic: Fatty food intolerance Epigastric distress, nausea Vague RUQ pain Complications: Ca or obstructive jaundice
 Fever, nausea, vomiting, leukocytosis. Jaundice (25% of cases) Increased WBC count. Increased serum alkaline phosphatase (duct damage) Chronic: Fatty food intolerance. Epigastric distress, nausea. Vague RUQ pain. Complications: Ca or obstructive jaundice.")
17
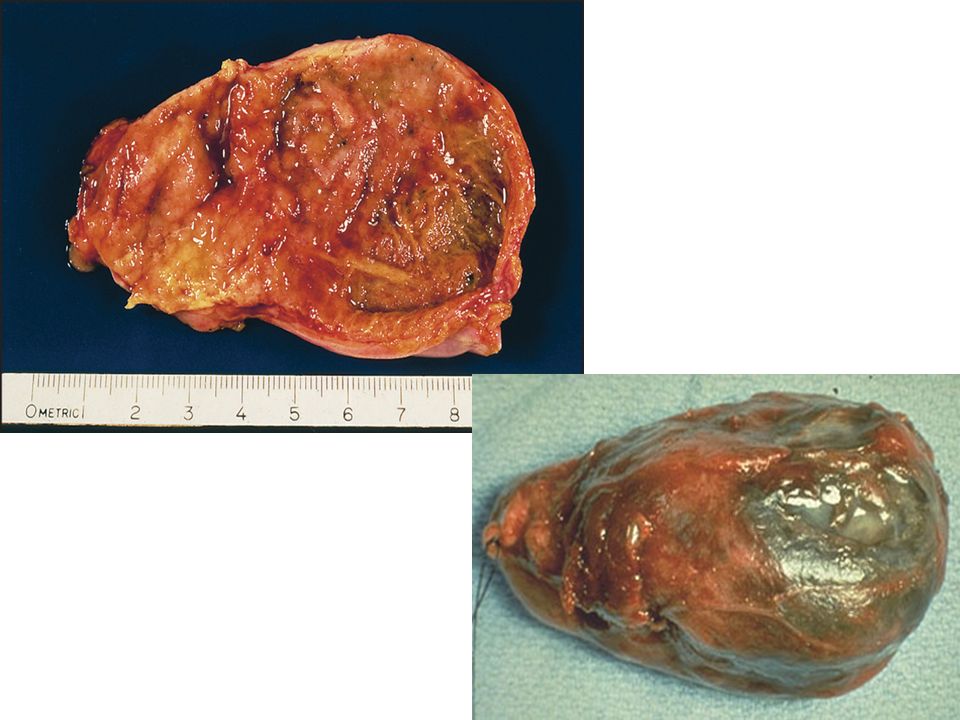
Acute Cholecystitis Gross Pathology
The gallbladder is enlarged (x2 or x3) The gallbladder wall is thickened (x10) The serosa is covered by fibrin with subserosal hemorrhages The lumen is filled with turbid bile, fibrin or pus The mucosa is hyperemic, ulcerated or frankly necrotic Gallstones are present in 80% of cases
 The gallbladder wall is thickened (x10) The serosa is covered by fibrin with subserosal hemorrhages. The lumen is filled with turbid bile, fibrin or pus. The mucosa is hyperemic, ulcerated or frankly necrotic. Gallstones are present in 80% of cases.")
19
Acute Cholecystitis Histology
Edema and neutrophilic inflammation Vascular congestion Abscess formation & gangrenous necrosis Later neutrophils → eosinophils (subacute) Ca++ deposition: “porcelain gallbladder”
 Ca++ deposition: porcelain gallbladder")
20
Porcelain Gallbladder

21
Porcelain Gallbladder with Stones

23
Chronic Cholecystitis Gross Pathology
The gallbladder wall thickened (about x5) It is contracted, enlarged or of normal size Serosa is smooth and glistening with subserosal fibrosis Lumen contains normal bile Stones are present in 90% of cases
 It is contracted, enlarged or of normal size. Serosa is smooth and glistening with subserosal fibrosis. Lumen contains normal bile. Stones are present in 90% of cases.")
24
Chronic Cholecystitis Histology
Mucosa is preserved or atrophic Mononuclear cell infiltration Subepithelial and subserosal fibrosis Severe fibrosis with replacement of smooth muscle Outpouchings of mucosal epithelium through wall “Rokitansky-Aschoff sinuses”

28
Choledocholithiasis Passage of gallstones into common bile duct occurs in 10-15% of patients with cholelithiasis Majority are cholesterol stones formed in gallbladder Primary calculi arising de novo in ducts are typically pigmented stones in pts with: -Chronic recurrent cholangitis -Congenital anomalies of bile ducts (Caroli’s disease) -Dilated, sclerosed or strictured ducts -MDR3 gene defect leading to impaired biliary phospholipid secretion
 -Dilated, sclerosed or strictured ducts. -MDR3 gene defect leading to impaired biliary phospholipid secretion.")
29
Choledocholithiasis May remain asymptomatic
May pass spontaneously into duodenum May present as biliary colic or complications -Cholangitis -Obstructive jaundice -Pancreatitis -Secondary biliary cirrhosis

30
Cholangitis Acute or chronic
Bacteria present in 75% of pts with acute cholangitis Charcot’s triad Intermittent abdominal pain Spiking fevers with chills Jaundice

31
Biliary Atresia Complete or partial obstruction of lumen of extrahepatic biliary tree within first 3 months of life Perinatal type (80% to >90%) -Presumed normal biliary tree is destroyed at birth -Jaundice develops within 2 weeks -No associated congenital anomalies -Etiology unknown(?viral, ?autoimmunity) Fetal type (less common) -Jaundice at birth or within a day or 2 -Assoc cardiac and vascular malformations, sinus inversus, polysplenia, midgut malrotation -Presumed aberrant intrauterine development of extrahepatic biliary tree
 -Presumed normal biliary tree is destroyed at birth. -Jaundice develops within 2 weeks. -No associated congenital anomalies. -Etiology unknown( viral, autoimmunity) Fetal type (less common) -Jaundice at birth or within a day or 2. -Assoc cardiac and vascular malformations, sinus inversus, polysplenia, midgut malrotation. -Presumed aberrant intrauterine development of extrahepatic biliary tree.")
32
Biliary Aresia Histologic features: Bile ductular proliferation
Portal fibrosis Bile plugs in bile ducts/ductules Parenchymal cholestasis

33
Biliary Atresia Type I – Disease limited to common bile duct
Type II – Disease limited to hepatic bile ducts Type III – Obstruction of ducts above porta hepatis

34
Biliary Atresia Normal birth weight and postnatal weight gain
Initially normal stools but become acholic stools Present with neonatal cholestasis Timing of biopsy Liver biopsy shows nonspecific changes at less than 4 weeks Fairly good sensitivity/specificity at 6-8 weeks Diagnostic at >8 weeks Cirrhosis develops within 3 to 6 months if not recognized Kasai procedure for types I and II Liver transplantation for rest Without surgery, death within 2 years

35
Choledochal Cysts Congenital dilatations of bile duct

36
Choledochal Cysts Present most often before 10 yrs of age
Jaundice, abdominal pain, abdominal mass Delayed diagnosis can lead to complications: Pancreatitis Spontaneous perforation Cholelithiasis Cholangitis Secondary biliary cirrhosis Portal hypertension Carcinoma

37
Carcinoma of Gallbladder
Close to 50% of gallbladder carcinomas are diagnosed incidentally in cholecystectomy specimens for cholelithiasis Most important risk factor is cholelithiasis -Gallstones present in >80% of gallbladders with carcinomas -But low incidence of carcinoma in pts with gallstones, <0.2% Slightly more common in women Most frequent in seventh decade of life Mean 5 year survival of 5 to 12%

38
Carcinoma of the Gallbladder Clinical Symptoms
Pain % Weight loss 60% Jaundice 50% Gallstones % Palpable mass 60% Ascites %

39
Carcinoma of the Gallbladder Histologic Types
Adenocarcinoma Adenosquamous carcinoma Squamous cell carcinoma Intracystic or intraductal papillary neoplasm with an associated invasive carcinoma Mucinous cystic neoplasm with an associated invasive carcinoma Undifferentiated carcinoma Neuroendocrine neoplasms Mesenchymal tumors

40
Dysplasia

41
Adenoca. of Gallbladder

42
Adenoca of Gallbladder

43
Adenoca of Gallbladder

44
Adenoca of Gallbladder

45
Biliary Disease Gallbladder Disorders Extrahepatic Bile Duct Disorders
-Cholelithiasis -Cholesterolosis -Cholecystitis Extrahepatic Bile Duct Disorders -Choledocholithiasis -Cholangitis -Biliary Atresia -Choledochal cysts Tumors

Similar presentations







.>")

 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FIVE Dr. Essam H. Aljiffri.>")












 Gallstones afflict 10-20% of adult populations in northern hemisphere Western countries. Adult prevalence rates.>")

what is a reverse mortgage australia