Download presentation
Presentation is loading. Please wait.

1
CELL ADAPTATIONS CELL INJURY CELL DEATH DR.SAMINA QAMAR AP PATHOLOGY.

2
OBJECTIVES Understand the concepts of cellular growth adaptations---Hyperplasia, Hypertrophy, Atrophy, Metaplasia, Dysplasia Reversible, irreversible cell injury

3
OBJECTIVES Understand the pathologic mechanisms at the SUB-cellular level---ATP, Mitochondria, Ca++, Free Radicals, Membranes Understand and differentiate the concepts of APOPTOSIS and NECROSIS Understand SUB-cellular responses to injury---Lysosomes, Smooth endoplasmic reticulum, Mitochondria, Cytoskeleton

4
OBJECTIVES Identify common patterns of cellular swelling and fatty change. Cell aging

5
To maintain a steady state of structure and function is HOMEOSTASIS

6
Cellular response to injury Non-lethal injury: cell will adapt Hypoxia, chemical injury, infection: Reversible injury will result in fatty change. Irreversible injury will result in death Repeated Injury: cellular aging

7
ADAPTATIONS: Non-lethal injury. Altered/changed steady state in structure and function of cell. WHY: In response to physical/ pathological stimuli. Increased or decreased stimulation or any irritation.

8
The –plasia brothers HYPER- HYPO- (A-) NORMO- META- DYS- ANA- “Frank” ANA-
 NORMO- META- DYS- ANA- Frank ANA-")
9
HYPER-PLASIA IN-CREASE IN NUMBER OF CELLS, if they can divide.

10
Examples: Endometrium,breast,liver.

11
The –trophy brothers HYPER- HYPO- (A-) DYS-
 DYS-")
12
HYPER-TROPHY IN - CREASE IN SIZE OF CELLS

13
Examples:Myocardium, Myometrium, Muscle

14
Hypertrophy v/s Hyperplasia.

15
Can both occur simultaneously?

16
A-TROPHY*? DE - CREASE IN SIZE OF CELLS? YES SHRINKAGE IN CELL SIZE DUE TO LOSS OF CELL SUBSTANCE

17
ATROPHY DECREASED WORKLOAD DENERVATION DECREASED BLOOD FLOW DECREASED NUTRITION AGING (involution) PRESSURE “EXHAUSTION”
 PRESSURE EXHAUSTION")
18
Examples: Brain, Muscle.

19
METAPLASIA A SUBSTITUTION of one NORMAL CELL or TISSUE type, for ANOTHER –COLUMNAR SQUAMOUS (Cervix) –SQUAMOUS COLUMNAR (Esophagus) –FIBROUS BONE –WHY?
 –SQUAMOUS COLUMNAR (Esophagus) –FIBROUS BONE –WHY")
20
Examples: Respiratory epithelium, Barrett’s, myositis ossificans.

21
Dysplasia: disorganized epithelium.

22
Dysplasia:

23
Normal-hyperplasia-dysplasia- carcinoma.

24
CELL DEATH

25
What is DEATH? –DEATH is IRREVERSIBLE –But in cell its either reversible or irreversible. APOPTOSIS vs. NECROSIS

26
REVERSIBLE CHANGES REDUCED oxidative phosphorylation ATP depletion Cellular “SWELLING”

27
IRREVERSIBLE CHANGES MITOCHONDRIAL IRREVERSIBILITY IRREVERSIBLE MEMBRANE DEFECTS LYSOSOMAL DIGESTION

28
REVERSIBLE = INJURY IRREVERSIBLE = DEATH SOME INJURIES CAN LEAD TO DEATH IF PROLONGED and/or SEVERE enough

29
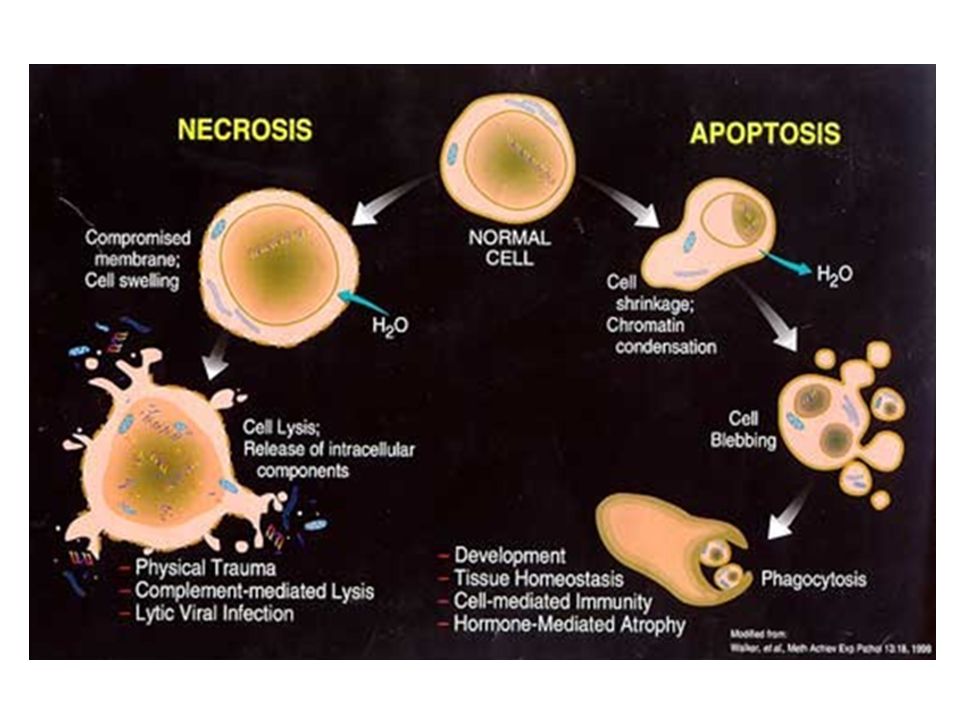
CELL DEATH APOPTOSIS (“normal” death) programmed death. NECROSIS (“premature” or “untimely” death
 programmed death. NECROSIS ( premature or untimely death")
30
Death is of two types

33
INJURY CAUSES (REVERSIBLE) Hypoxia, (decreased O2) PHYSICAL Agents CHEMICAL Agents INFECTIOUS Agents Immunologic Genetic Nutritional
 Hypoxia, (decreased O2) PHYSICAL Agents CHEMICAL Agents INFECTIOUS Agents Immunologic Genetic Nutritional")
34
CHEMICAL INJURY “Toxic” Chemicals, e.g CCl4 Drugs, e.g tylenol Dose Relationship Free radicals, organelle, DNA damage

35
INJURY MECHANISMS (REVERSIBLE) DECREASED ATP MITOCHONDRIAL DAMAGE INCREASED INTRACELLULAR CALCIUM INCREASED FREE RADICALS INCREASED CELL MEMBRANE PERMEABILITY
 DECREASED ATP MITOCHONDRIAL DAMAGE INCREASED INTRACELLULAR CALCIUM INCREASED FREE RADICALS INCREASED CELL MEMBRANE PERMEABILITY")
36
What is Death? What is Life? DEATH is –IRREVERSIBLE MITOCHONDRIAL DYSFUNCTION –PROFOUND MEMBRANE DISTURBANCES LIFE is……..??? Till death hasn’t occurred.

37
DEATH: ELECTRON MICROSCOPY B-Microvillus incorporated in cell, Blebs extruded from cell. C- Mitochondrial swelling.

38
DEATH:PINK IN LIGHT MICROSCOPY Nuclei

39
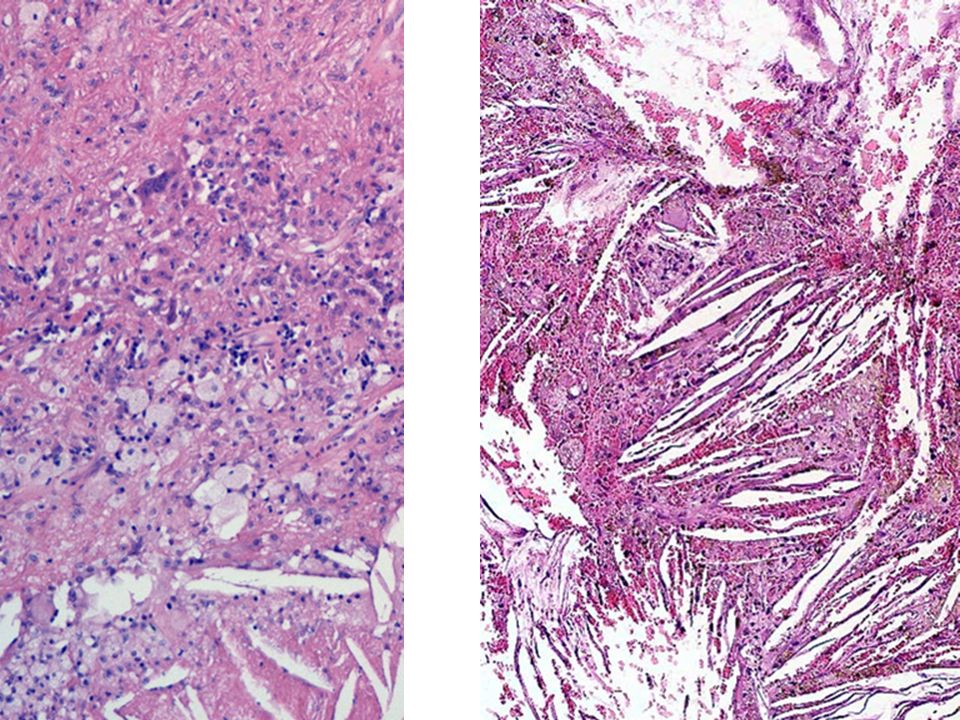
LIQUEFACTIVE NECROSIS, BRAIN

40
FIBRINOID NECROSIS

41
APOPTOSIS: falling off. NORMAL (preprogrammed) PATHOLOGIC (associated with Necrosis)
 PATHOLOGIC (associated with Necrosis)")
42
“NORMAL” APOPTOSIS Embryogenesis Hormonal “Involution” Cell population control, e.g., “crypts” Post Inflammatory “Clean-up” Elimination of “HARMFUL” cells Cytotoxic T-Cells cleaning up

43
“PATHOLOGIC” APOPTOSIS “Toxic” effect on cells, e.g., chemicals, pathogens Duct obstruction Tumor cells Apoptosis/Necrosis spectrum

44
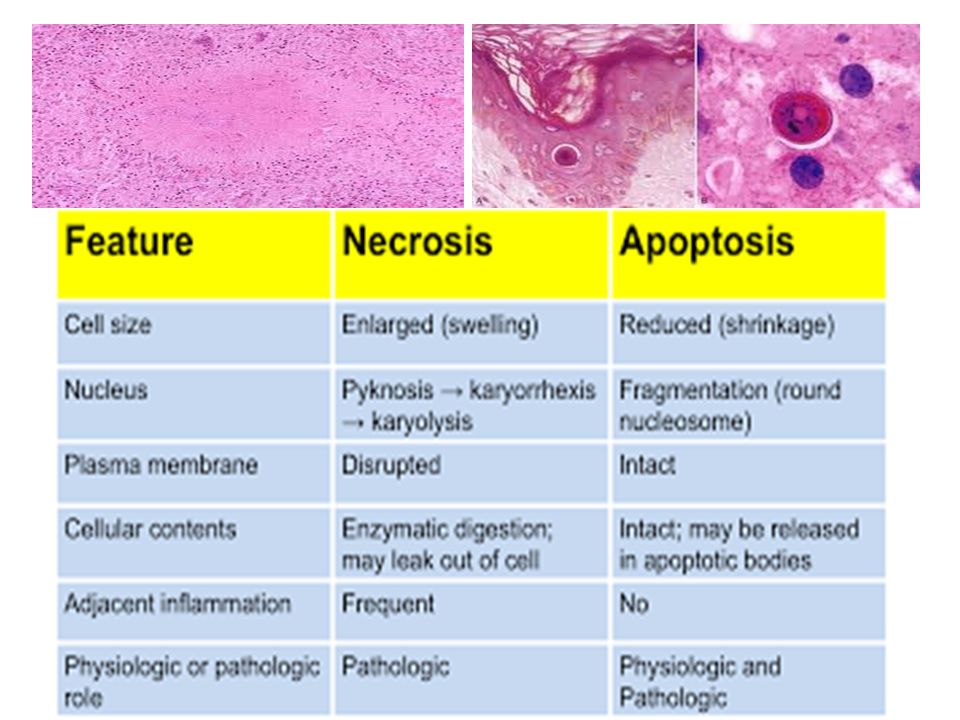
APOPTOSIS MORPHOLOGY DE-crease in cell size, i.e., shrinkage IN-crease in chromatin concentration, i.e., hyperchromasia, pyknosis karyorhexis karyolysis IN-crease in membrane “blebs” Phagocytosis

45
SHRINKAGE/HYPERCHROMASIA Karryorhexis, karryolysis.

46
PHAGOCYTOSIS

48
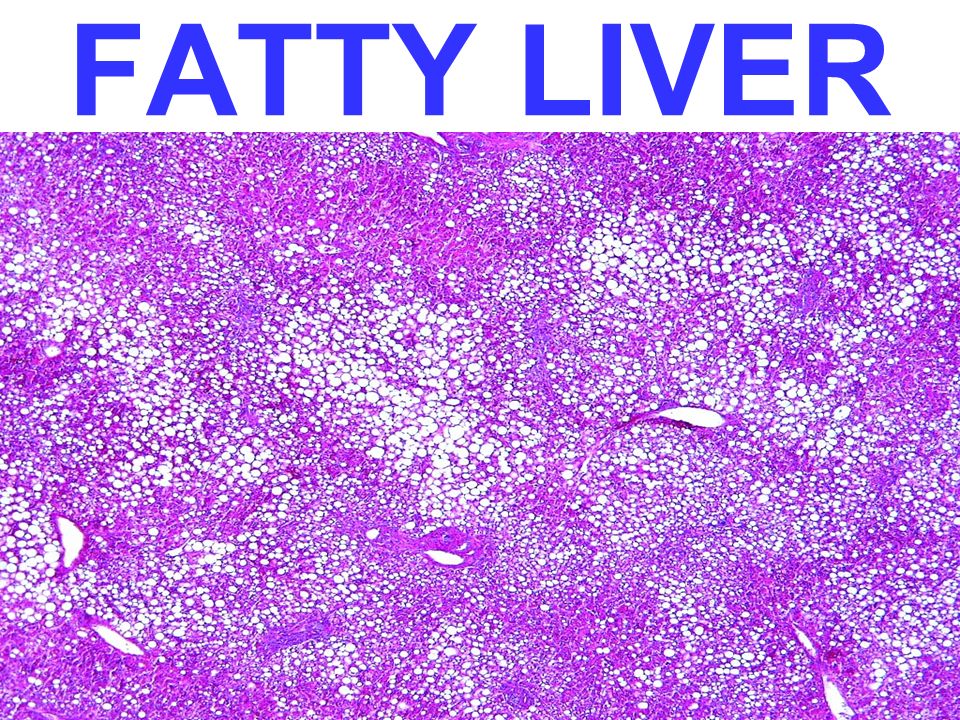
Damaged/necrotic cells can accumulate fat: Fatty change Commonly occurs in Liver, heart. Due to defective uptake, catabolism or secretion of lipid. Severe fatty change can alter cellular structure and function. Seen in diabetes, alcoholism, obesity.

49
LIPID LAW ALL Lipids are YELLOW grossly and WASHED out (CLEAR) microscopically
 microscopically")
50
FATTY LIVER

53
CELL AGING It is due to progressive decline in cellular function resulting from exposure to exogenous influences. Cell can undergo limited number of divisions and goes into non-dividing or senescence phase. Accumulation of metabolic and genetic changes that damage DNA.

54
TELOMERES Telomeres are sequences of DNA present at ends of chromosomes. They become shorter with every division. Once shortened they cannot protect ends of chromosome and appear as damaged DNA. Cell goes into cell cycle arrest.

Similar presentations







: Fatty Change (Steatosis): Abnormal accumulation of triglycerides within parenchymal cells seen in.>")





. Causes of cell injury Hypoxia (oxygen deprivation) Occurs due to Loss of blood supply - Ischaemia Inadequate.>")








>")