Download presentation
Presentation is loading. Please wait.

2
OBSTRUCTIVE SLEEP APNEA HYPOPNEA SYNDROME BY AHMAD YOUNES PROFESSOR OF THORACIC MEDICINE Mansoura Faculty of Medicine

3
According to the American Academy of Sleep Medicine (AASM) OSA is characterized by repetitive episodes of complete (apnea) or partial (hypopnea) upper airway obstruction occurring during sleep.
 OSA is characterized by repetitive episodes of complete (apnea) or partial (hypopnea) upper airway obstruction occurring during sleep.")
4
The 2007 AASM diagnostic criteria and definitions:- Apnea is defined as the drop in peak airflow by >90% of baseline for 10 seconds or longer and at least 90% of the event duration meet the amplitude reduction. Obstructive apnea is defined as continued or increased inspiratory effort throughout the entire period of absent flow Mixed apneas ventilatory effort is not observed initially (central apneic component), but ventilatory effort follows (obstructive apnea component).
, but ventilatory effort follows (obstructive apnea component)..")
5
The 2007 AASM diagnostic criteria and definitions:- Hypopnea is defined as the drop in peak airflow by >30% of baseline for 10 seconds or longer associated with >4% desaturation from pre-event baseline and at least 90% of the event duration meet the amplitude reduction Or Hypopnea is defined as the drop in peak airflow by >50% of baseline for 10 seconds or longer associated with >3% desaturation from pre-event baseline or arousal and at least 90% of the event duration meet the amplitude reduction.

6
The 2007 AASM diagnostic criteria and definitions:- Respiratory effort related arousals is defined as the increase in respiratory effort or sustained respiratory effort for 10 seconds or longer leading to arousal from sleep when the sequence of breathes does not fulfile criteria of apnea or hypopnea The criterion standard to measure RERAs is esophageal manometry, as the AASM recommends. However, esophageal manometry is uncomfortable for patients and impractical to use in most sleep centers.

7
Complex Sleep Apnea (CompSA) Comp-SA consists of all or predominantly obstructive apneas which convert to all or predominantly central apneas when treated with a CPAP or bilevel devices. The RDI is defined as the number of apneas, hypopneas, and respiratory event–related arousals (RERAs) per hour. The RDI is preferred over the AHI because it includes flow-limitation events that end with arousals
 per hour. The RDI is preferred over the AHI because it includes flow-limitation events that end with arousals.")
8
Criteria for OSA: ( Diagnosis = A + B + D or C + D) A. At least one of the following applies: i. Complaints of unintentional sleep episodes during wakefulness, daytime sleepiness, unrefreshing sleep,fatigue, or insomnia. ii. Awakenings with breath-holding, gasping, or choking. iii. Bed partner reports loud snoring and/or breathing interruptions during the patient’s sleep. B. Polysomnography shows the following: i. Respiratory events (apneas + hypopneas + RERAs)/hr of sleep ≥ 5/hr. ii. Evidence of respiratory effort during all or a portion of each respiratory event OR C. Polysomnography shows the following: i. Respiratory events (apneas + hypopneas + RERAs)/hr of sleep ≥ 15/hr. ii. Evidence of respiratory effort during all or a portion of each respiratory event. D. The disorder is not better explained by: another current sleep disorder, medical or neurologic disorder, medication use, or substance use disorder.
/hr of sleep ≥ 5/hr. ii. Evidence of respiratory effort during all or a portion of each respiratory event OR C. Polysomnography shows the following: i. Respiratory events (apneas + hypopneas + RERAs)/hr of sleep ≥ 15/hr. ii. Evidence of respiratory effort during all or a portion of each respiratory event. D. The disorder is not better explained by: another current sleep disorder, medical or neurologic disorder, medication use, or substance use disorder..")
9
Historical perspectives In 1965, Gestaut, Tassinari, and Duron in France and Jung and Kuhlo in Germany provided the first accurate clinical descriptions of OSA at nearly the same time. The first known successful treatment for OSA was tracheostomy, which Elio Lugaresi and coworkers first described in 1970 in Italy. In 1981, Dr Colin Sullivan introduced continuous positive airway pressure (CPAP) as a treatment for OSA. In 1981, Fugita and colleagues introduced uvulopalatopharyngoplasty (UPPP).
 as a treatment for OSA. In 1981, Fugita and colleagues introduced uvulopalatopharyngoplasty (UPPP)..")
10
Frequency Although early investigators estimated the prevalence of sleep-disordered breathing (SDB) to be 2% for middle- aged women and 4% for middle-aged men, more recent research indicates a prevalence of 4% for women and 9% for men. The prevalence increases with age. OSA remains undiagnosed in approximately 92% of affected women and 80% of affected men.

11
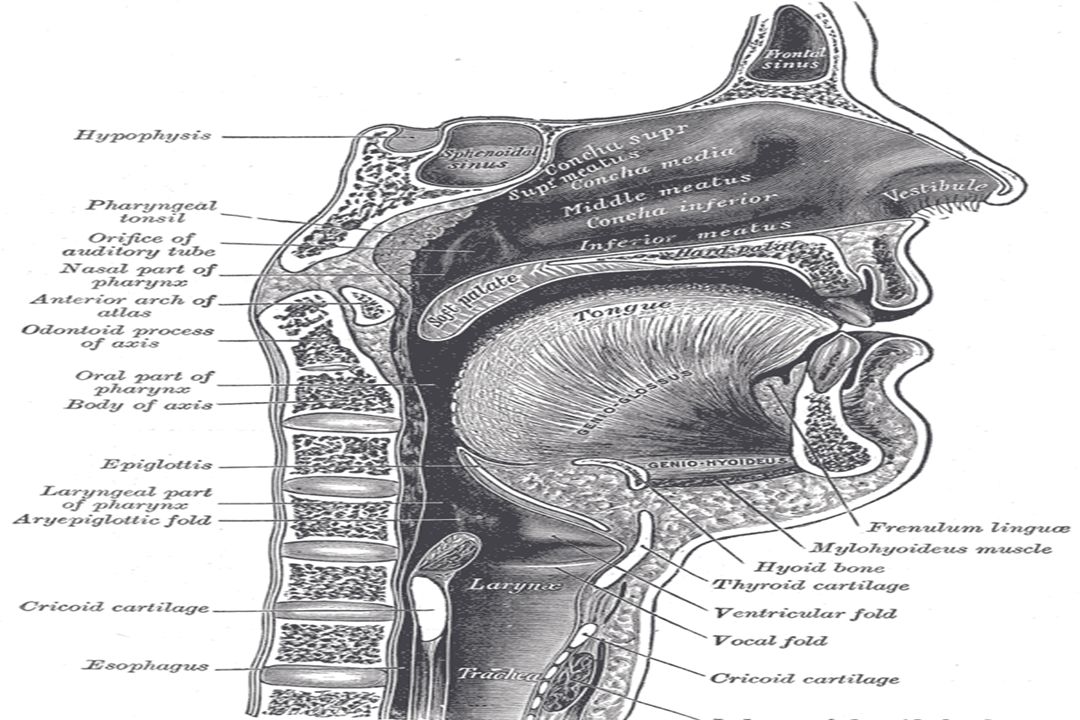
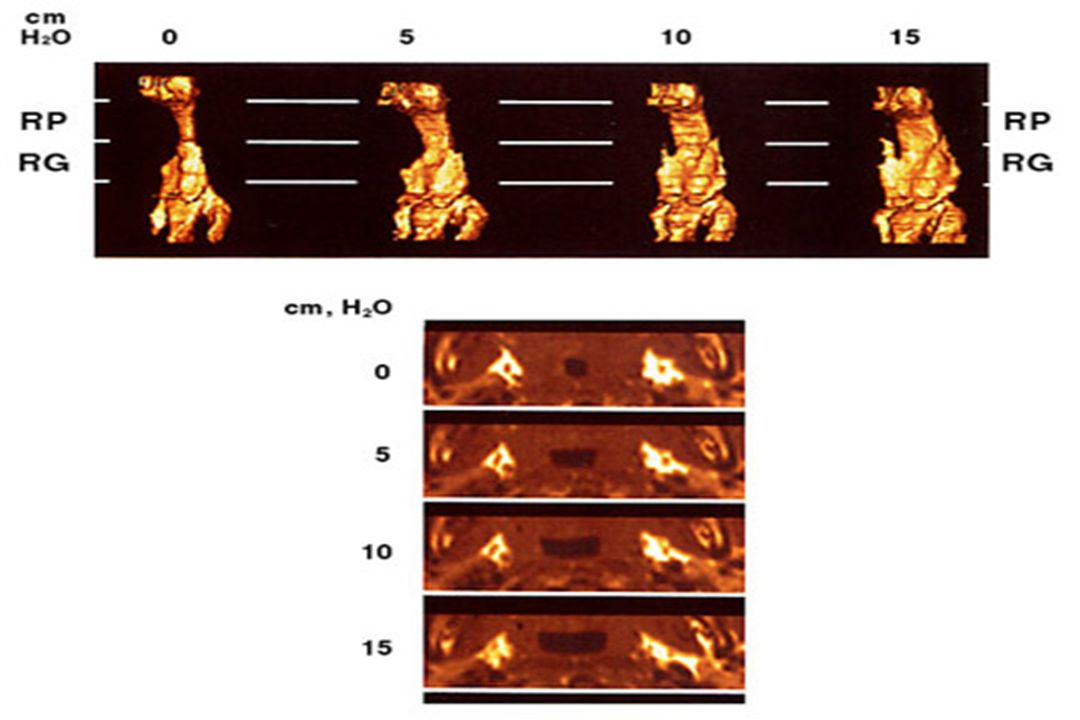
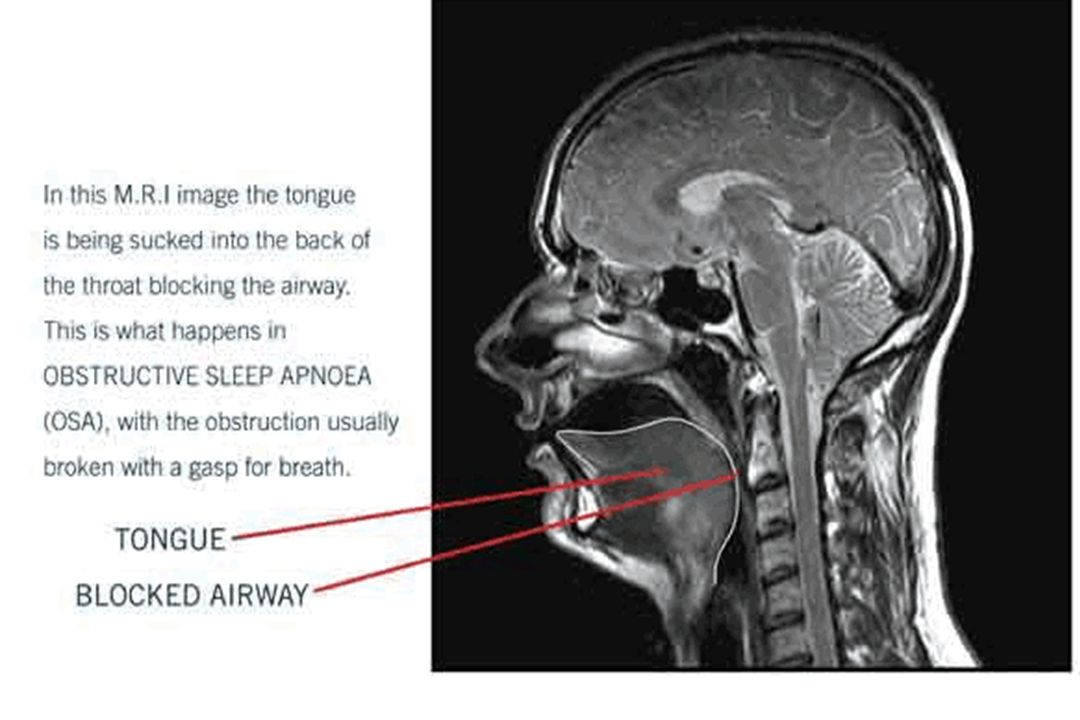
Pathophysiology pharyngeal collapse is responsible for the recurrent UA obstruction during sleep in patients with OSA. The retro-palatal area is the primary, but not only, site of airway narrowing. Airway narrowing occurs in ovoid geometric progression, with narrowing occurring both laterally and antero-posteriorly. During wakefulness, the pharyngeal airway appears to be smaller in patients with OSA compared with healthy subjects. In the absence of craniofacial abnormalities, the soft palate, tongue, para- pharyngeal fat pads, and lateral pharyngeal walls are enlarged.

13
Diagnosis Clinical history and physical examination findings are of paramount importance in the evaluation of a patient with suspected OSA. Management decisions should be made in the context of the complete clinical picture because: 1-PSG evidence by itself is insufficient to determine if a patient has clinically significant OSA. 2- Moreover, physical findings alone cannot predict OSA.

14
Cardinal symptoms of sleep apnea _ Loud, habitual snoring –Apneic events witnessed or reported by spouses – Daytime sleepiness Predictive value –A history of disruptive snoring has 71% sensitivity in predicting OSA –Disruptive snoring and witnessed apneas: These factors together have 94% specificity for OSA.

15
Other symptoms –Non-restorative sleep –A choking sensation or gasping during the night –Morning headaches, –Insomnia –Restless sleep –Sore throat or dry mouth in the morning –Memory and intellectual impairment –Depression and anxiety –Impotence and decreased libido –Gastro-esophageal reflux disease

17
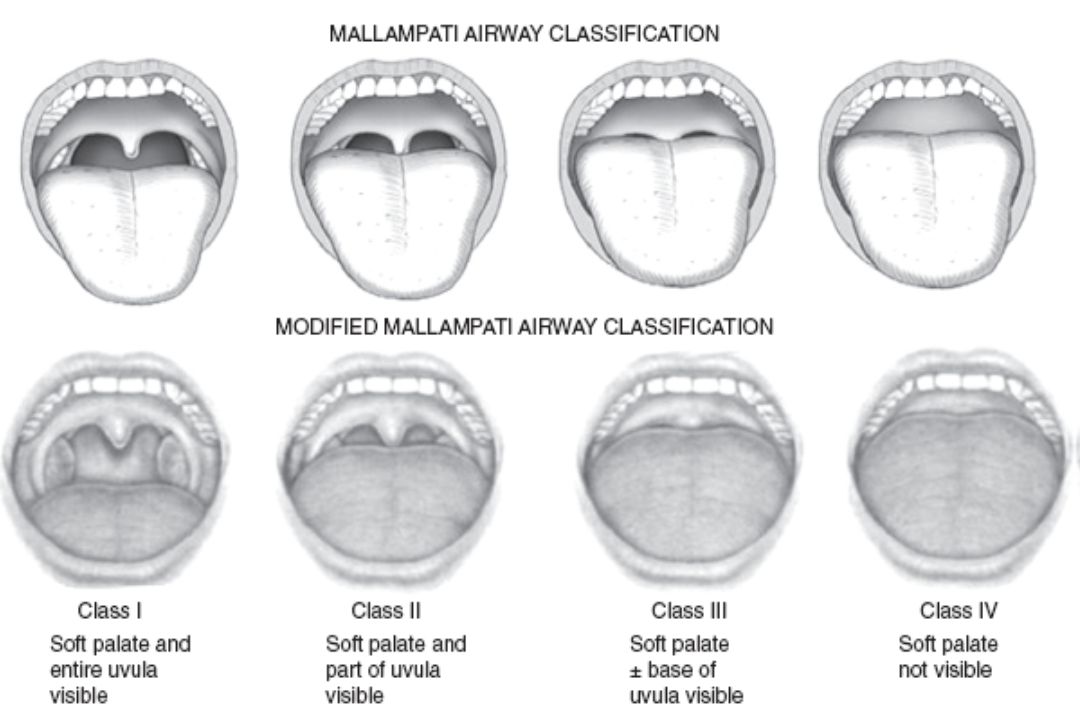
Physical EXAMINATION Obesity is a risk factor for OSA. –50% of patients with a BMI greater than 40 have OSA. –Neck circumference may correlate with OSA better than BMI. – Women may have BMI lower than those of men. –In women, the neck circumference is relatively normal -UA abnormalities include severe nasal obstruction, low- hanging soft palate, large uvula, enlarged tonsils and/or adenoids, and macro-glossia. Systemic arterial hypertension is present in approximately 50% of patients with OSA. Craniofacial abnormalities –Women may have a high, arched hard palate.

19
Structural factors –Nasal obstruction that predispose patients with OSA to pharyngeal collapse during sleep include polyps, septal deviation, tumors, trauma, and stenosis. –Retropalatal obstruction that predispose patients with OSA to pharyngeal collapse during sleep include (1) an elongated, posteriorly placed palate and uvula (2) tonsil and adenoid hypertrophy (particularly in children. –Retroglossal obstruction that predispose patients with OSA to pharyngeal collapse during sleep include macroglossia and tumors Genetic variations (facial elongation, posterior facial compression) Retrognathia and micrognathia Inferior displacement of the hyoid Down syndrome Marfan syndrome High, arched palate (particularly in women)
 an elongated, posteriorly placed palate and uvula (2) tonsil and adenoid hypertrophy (particularly in children. –Retroglossal obstruction that predispose patients with OSA to pharyngeal collapse during sleep include macroglossia and tumors Genetic variations (facial elongation, posterior facial compression) Retrognathia and micrognathia Inferior displacement of the hyoid Down syndrome Marfan syndrome High, arched palate (particularly in women).")
21
Non-structural risk factors –Some nonstructural risk factors include obesity, age, male sex, post-menopausal state, and habitual snoring with daytime somnolence. –Familial factors also play a role. Families with a high incidence of OSA are reported. Relatives of patients with SDB have a 2- to 4-fold increased risk of SDB compared with control subjects. –Environmental exposures include smoke, environmental irritants or allergens, and alcohol and hypnotic-sedative medications. –Both hypothyroidism and acromegaly are associated with macroglossia and increased soft tissue mass in the pharyngeal region. They are associated with an increased risk of SDB. Hypothyroidism is also associated with myopathy that may contribute to UA dysfunction

22
Lab Studies Routine laboratory tests usually are not helpful unless a specific indication is present. Consider obtaining a thyrotropin hormone level if clinically indicated, particularly in elderly individuals. An arterial blood gas determination should be obtained if obesity hypoventilation syndrome (or another cause of clinically significant pulmonary hypertension) is suspected.
 is suspected..")
23
Imaging Studies Modalities available for identifying the site of obstruction include lateral cephalometry, endoscopy, fluoroscopy, CT scanning, MRI. The accuracy of these methods in identifying the sites of obstruction is not clear. At present, UA imaging is used primarily as a research tool. Routine radiographic imaging of the UA in the initial evaluation of SDB patients is of uncertain benefit and should not be performed unless a specific indication is present.

25
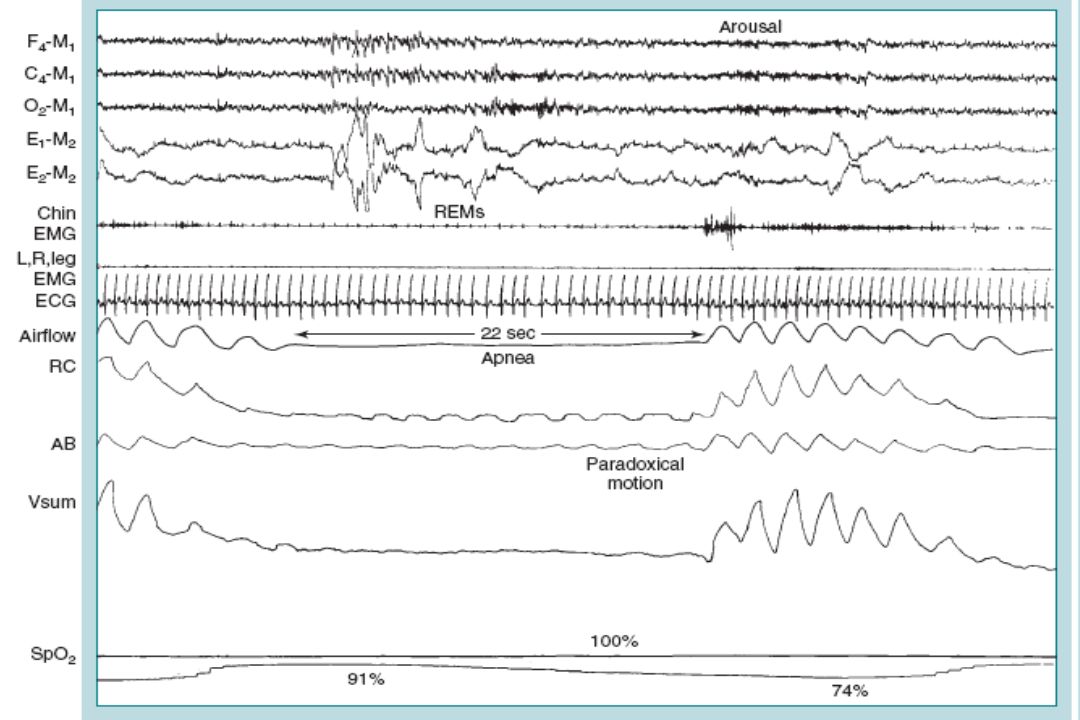
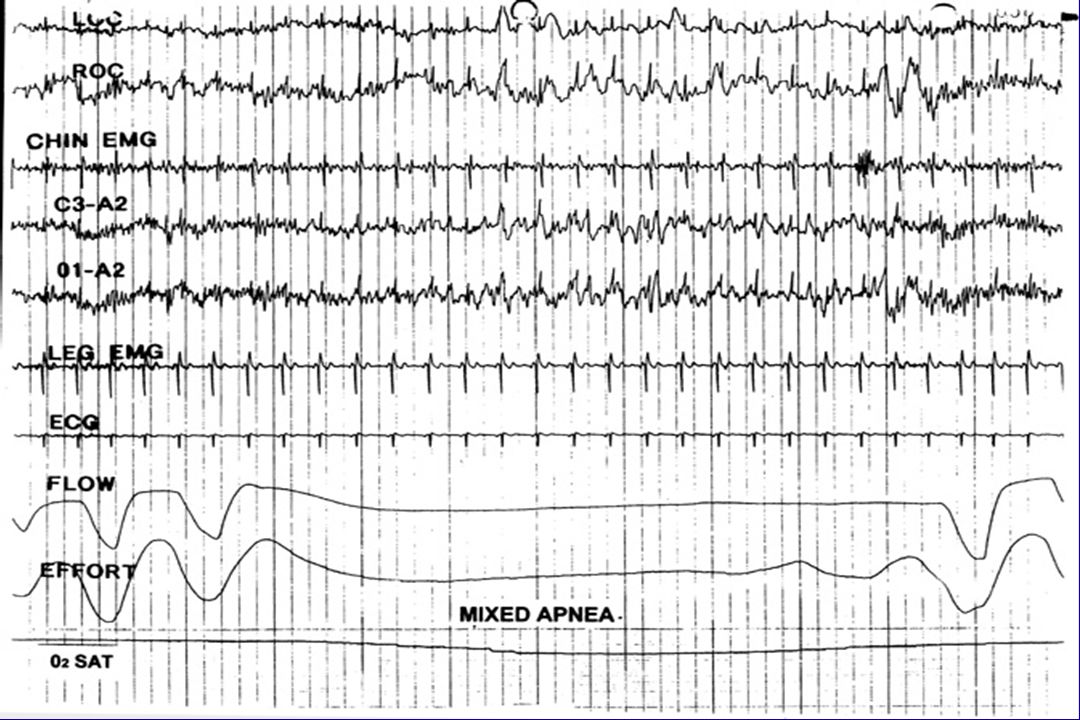
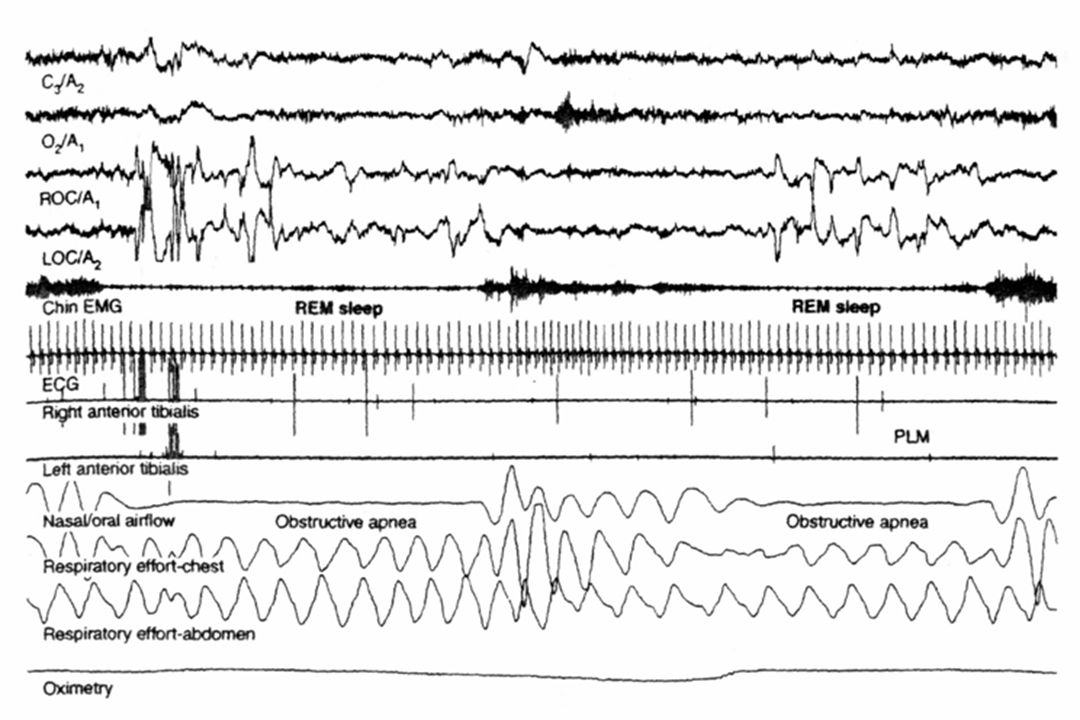
PSG findings of OSA Apneic episodes occur in the presence of respiratory muscle effort Apneic episodes lasting 10 seconds or longer are considered clinically significant. Apneic episodes are usually approximately 20-40 seconds and rarely last several minutes. Apneic episodes are most prevalent during REM sleep. Mixed apneas(combination of central sleep apnea and OSA in a single apneic episode) may occur. Sleep disruption due to arousals is usually seen at the termination of an episode of apnea.
 may occur. Sleep disruption due to arousals is usually seen at the termination of an episode of apnea..")
29
Eye Movements

33
AASM guidelines for split-night PSG Patients with an RDI of greater than 40 during the first 2 hours of diagnostic PSG should undergo a split-night PSG study. The final portion of the study is used for titrating the CPAP device. Split-night studies may be considered for patients with an RDI of 20-40, as based on clinical observations (eg, prolonged obstructive events, marked oxygen de-saturation). A minimum of 3 hours of sleep is preferred to adequately titrate the CPAP device after this treatment is started. NB:A single split-night study may not permit adequate titration of CPAP therapy. If treatment does not control symptoms, additional full-night CPAP titration may be required.
. A minimum of 3 hours of sleep is preferred to adequately titrate the CPAP device after this treatment is started. NB:A single split-night study may not permit adequate titration of CPAP therapy. If treatment does not control symptoms, additional full-night CPAP titration may be required..")
34
Unattended portable PSG performed in the patient's home may be effective for diagnosing severe OSA when performed by a qualified sleep specialist as part of a comprehensive sleep consultation. Any patient who is initially tested with unattended portable PSG studies and who does not have a satisfactory diagnosis must have automatic access to a comprehensive sleep consultation and additional diagnostic testing. Unattended PSG

35
Limited PSG studies A portable monitoring device is being used for limited-channel, in- laboratory diagnostic PSG studies (cardiopulmonary monitoring). include assessments of oro-nasal airflow, chest-wall respiratory effort, ECG findings, and oxyhemoglobin saturation. Limited PSG studies may be indicated in the following settings: Patients with severe symptoms indicative of OSA when treatment is urgently needed and when standard PSG is not readily available. Patients with established OSA who require follow-up studies Patients who cannot be evaluated in the sleep laboratory

36
Repeat PSG Repeat PSG if symptoms persist despite adequate compliance with prescribed CPAP treatment. PSG can be used to assess response to UA surgical procedures and to assess response to OA therapy. If sustained weight change of greater than 15% occurs, PSG should be repeated. Finally, if results of the first PSG are of poor quality, a repeat study is indicated.

37
Treatments All patients should be offered nasal CPAP therapy first. In patients with mild-to-severe OSA who refuse or reject nasal CPAP therapy, BiPAP therapy should be tried next. If this therapy fails or is rejected, OA therapy should be considered. OA may be considered first-line therapy for patients with mild OSA, particularly if they are unwilling to try nasal CPAP therapy. Patients in whom noninvasive medical therapy ( PAP, OA) fails should be offered surgical options. Patients should be made aware of the success rates for each surgical procedure. They should be informed that they might require more than 1 surgical procedure, some fairly extensive, to cure OSA.
 fails should be offered surgical options. Patients should be made aware of the success rates for each surgical procedure. They should be informed that they might require more than 1 surgical procedure, some fairly extensive, to cure OSA..")
38
General and behavioral measures weight loss Avoidance of alcohol use, sedative use, and being in the supine position, Pharmacologic therapy is not part of treatment. No clinically useful drug therapy is currently available.

39
Guidelines for use of CPAP therapy Patients with (RDI >15) should be treated irrespective of their symptoms because of the increased risk of cardiovascular morbidity. Patients with an RDI of 5-15 should be treated if they have symptoms or coexistent cardiovascular disease. CPAP is titrated after the diagnostic portion of a split-night protocol or on a separate night after a diagnostic PSG. Proper titration includes identifying the minimum CPAP level that abolishes obstructive apneas and/or hypopneas, oxyhemoglobin desaturation, RERAs, and snoring in all sleep stages and in all sleep positions. The pressure needed is typically 5-20 cm of water.

40
BiPAP therapy No studies have conclusively demonstrated improved compliance with BiPAP devices compared with CPAP devices. In patients who cannot tolerate CPAP, a trial of BiPAP is warranted. However, BiPAP is too expensive to be used as first-line therapy, and it has no distinct advantages over CPAP therapy.

43
Treatment of snoring and OSA with OA OA are indicated for use in patients with mild-to-moderate OSA who prefer OA to CPAP, those whose condition does not respond to CPAP, those who are not appropriate candidates for CPAP, and those in whom attempted CPAP or behavioral measures fail. Patients with severe OSA should receive an initial trial of nasal CPAP because CPAP is more effective than OA therapy. UA surgery may also supersede the use of OA in patients for whom these operations are predicted to be highly effective in treating sleep apnea. To ensure satisfactory therapeutic benefit from OA, patients with OSA should undergo PSG or an attended cardio- respiratory sleep study with the OA in place after final adjustment of fit is performed. OAs have better success rates in patients with mild OSA (81%) than in those with moderate (60%) or severe (25%) OSA.
 than in those with moderate (60%) or severe (25%) OSA..")
44
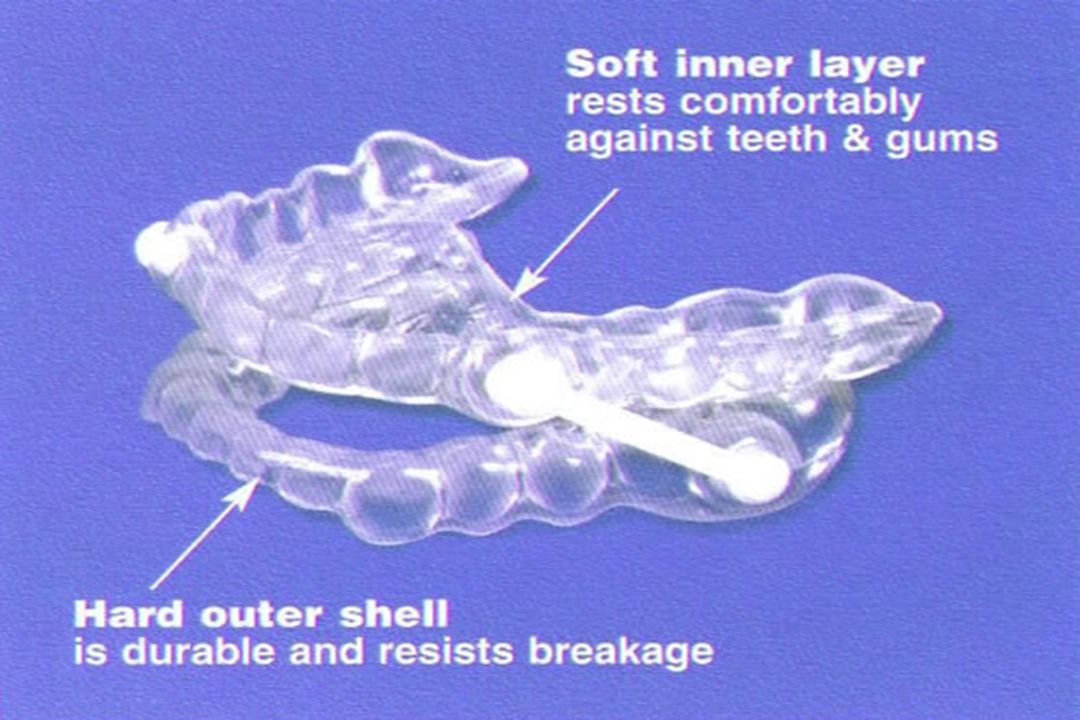
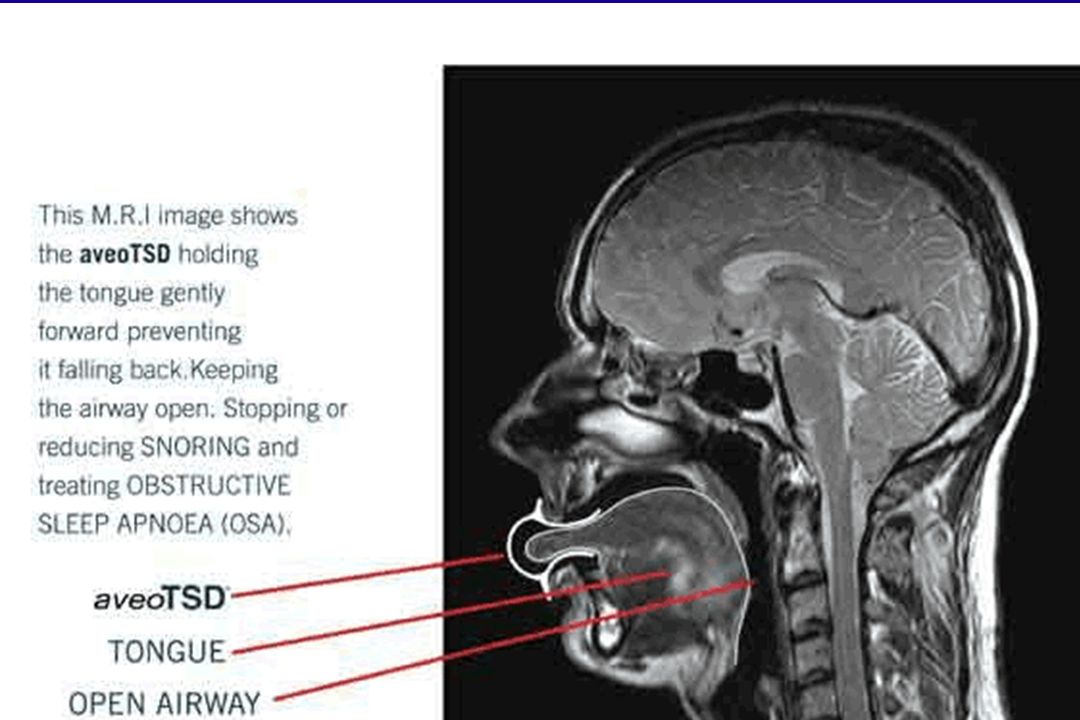
Types of OA Ttongue-retaining device (TRD). incorporated a pliable bulb in the front that holds the tongue forward. This bulb prevented the tongue from collapsing back into the airway during sleep. Mandibular re-positioners designed for mandibular advancement. These repositioners are adjusted to advance the jaw to 60-70% of the maximum protrusion of the jaw. Palatal lifting devices. More than 40 OA are available to manage SRBD and OSAS.

51
AASM recommendations for surgery Surgery is indicated in patients who have a specific underlying abnormality that is causing the OSA. Surgery may be indicated if noninvasive medical therapy (nasal CPAP or OA) fails or is rejected, if the patient desires such therapy, and if he or she is medically stable enough to undergo the procedure. If the patient has OSA that is moderately severe or severe (RDI >40 or lowest oxy-hemoglobin saturation <80%), the patient requires peri- operative airway protection with either nasal CPAP or a trache-ostomy.
 fails or is rejected, if the patient desires such therapy, and if he or she is medically stable enough to undergo the procedure. If the patient has OSA that is moderately severe or severe (RDI >40 or lowest oxy-hemoglobin saturation <80%), the patient requires peri- operative airway protection with either nasal CPAP or a trache-ostomy..")
52
Surgical procedures Functional division of the pharynx into retro-palatal and oro-pharyngeal and retro-lingual and hypo- pharyngeal regions has been proposed. Different surgical procedures have been proposed for patients with different levels of obstruction. UPPP may correct type I obstruction. Genioglossus advancement with hyoid myo-tomy (GAHM) may correct type III obstruction. Maxillo-mandibular advancement osteo-tomy (MMO) may correct obstruction at all levels.
 may correct type III obstruction. Maxillo-mandibular advancement osteo-tomy (MMO) may correct obstruction at all levels..")
53
Riley-Powell-Stanford surgical protocol Because several sites of obstruction may be responsible, a systematic approach for selecting surgery has been developed. This is the Riley-Powell-Stanford surgical protocol designed in 1988. The protocol has 2 phases. Phase I consists of the UPPP and GAHM procedures, phase II consists of the more complicated MMO procedure. Patients who are not adequately treated with phase I surgery are offered phase II surgery.

59
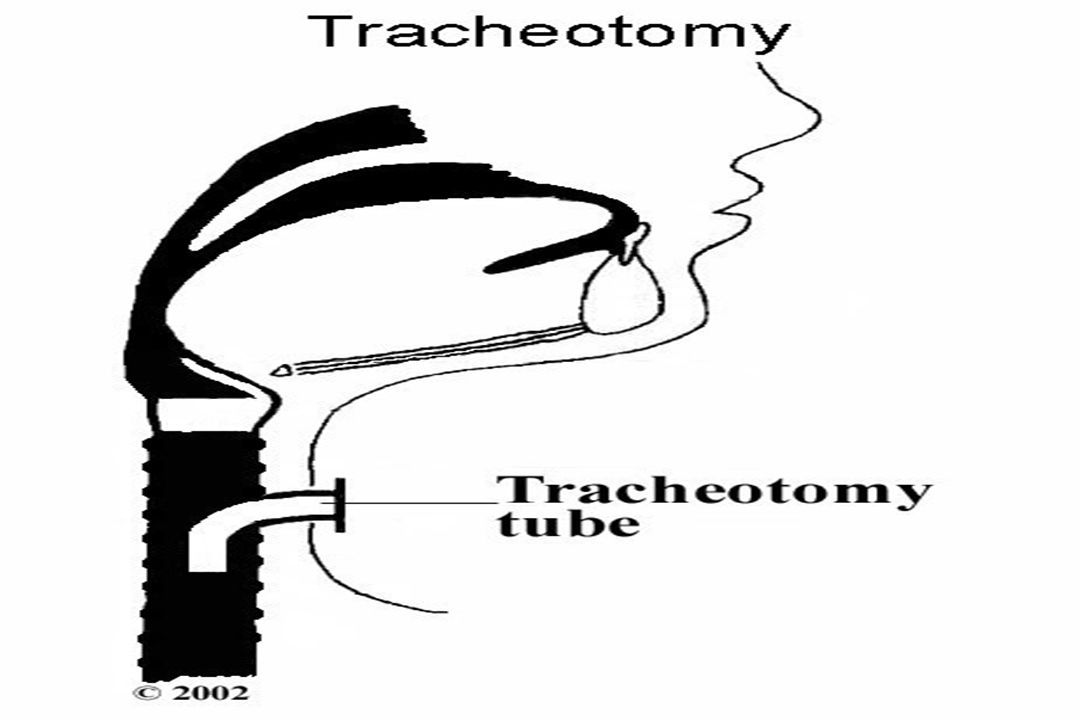
Tracheostomy This procedure bypasses the UA and is the most effective surgical procedure for treatment of OSA; it is virtually 100% effective. Unfortunately, tracheostomy is a disfiguring procedure and decreases the patient's quality of life. Tracheostomy is now reserved for patients with severe OSA in whom other medical and surgical treatment modalities fail. Tracheostomy is also used for airway protection during UA reconstructive surgery.

60
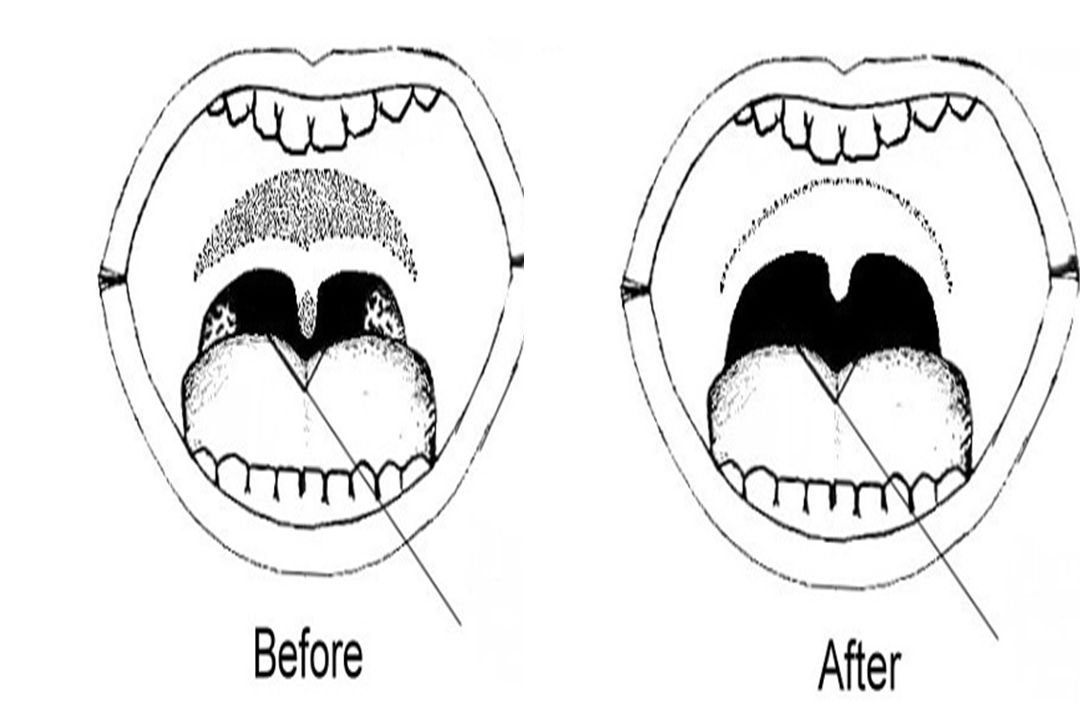
Uvulo-palato-pharyngoplasty UPPP is the most common surgical procedure performed for adults with OSA. Fujita and colleagues introduced this procedure to the United States in 1981. UPPP involves removal of the tonsils (if present), the uvula, the distal margin of the soft palate, and the redundant pharyngeal tissue, as well as reshaping of the soft tissues in the lateral pharyngeal walls.
, the uvula, the distal margin of the soft palate, and the redundant pharyngeal tissue, as well as reshaping of the soft tissues in the lateral pharyngeal walls..")
61
Complications of UPPP Pain with swallowing and pain with speech, Hemorrhage (2-4%) Swallowing difficulties, particularly regurgitation of food Long-term pharyngeal discomfort Disturbance in taste Numbness of tongue Nasopharyngeal stenosis Silent apnea may result. UPPP may end snoring but have no notable effect on episodes of sleep- associated obstruction. Patients must undergo postoperative PSG to rule out persistent OSA.

62
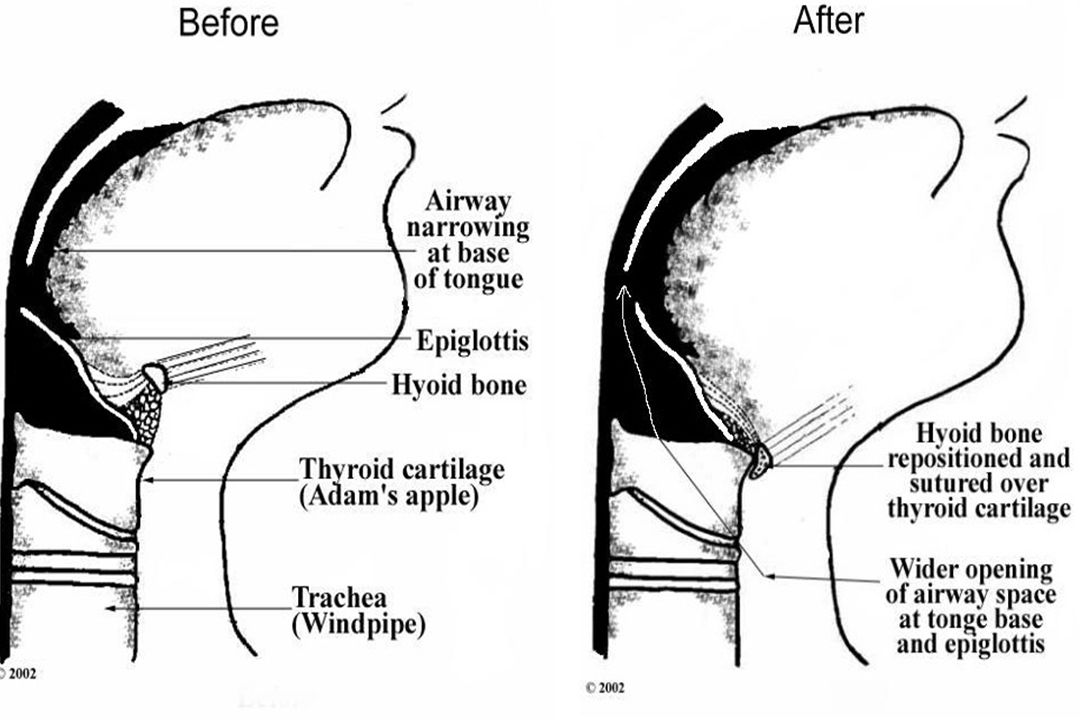
Genioglossus advancement with hyoid myotomy The genioglossus muscle is repositioned anteriorly through an inferior mandibular osteotomy (genioglossus advancement). This maneuver places the pharyngeal muscles and the base of the tongue on tension and expands the airway. The hyoid is suspended to the superior edge of the larynx and fixed in this position, adding to the effect of genioglossus advancement.

63
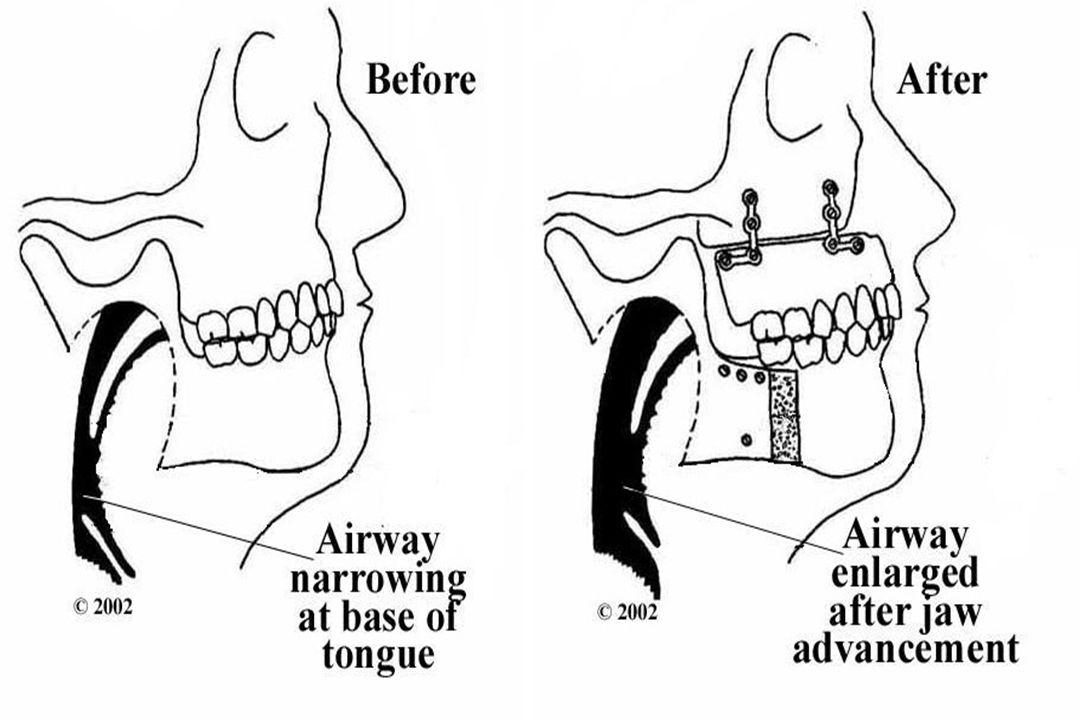
Maxillo-mandibular advancement osteo-tomy The mid-face, palate, and mandible are moved forward in this procedure, increasing the space behind the tongue and increasing tension on the genio-glossus muscle. This surgery is more extensive than any of the others described. It is usually reserved for patients in whom other treatment modalities fail.

64
Radiofrequency volumetric tissue reduction of the soft palate (somno-plasty) A midline soft palate sub-mucosal scar is created by using a needle electrode inserted near the border of the hard palate and directing it toward the uvula. Pulses of radiofrequency energy are delivered, resulting in tissue necrosis and needle-tract fibrosis over subsequent weeks to months.

65
Other surgical options Laser-assisted uvulo-palatoplasty is successful for reducing snoring in 90% of patients, but the success rate in patients with SDB is not clear. It may cause more scarring than UPPP, and it could potentially worsen apnea. Laser-assisted uvulo-palatoplasty is not recommended for the treatment of OSA until further data are available. Laser midline glossectomy and lingualplasty are performed to enlarge the retro-lingual region by using a laser to remove a portion of the posterior aspect of the tongue. The role of these procedures in the management of SDB has yet to be defined. Nasal surgery includes septoplasty, turbinectomy, and polypectomy and may be useful as an adjunct to other procedures or to improve CPAP compliance. Nasal surgery by itself is rarely effective for the treatment of OSA.

66
Drug Category: CNS stimulants May be used to promote daytime wakefulness in sleep apnea patients who have residual daytime sleepiness despite optimal use of CPAP. Modafanil and armodafinil are indicated for OSA.

Similar presentations

















 286-7455 Fax: (703) 286-7462.>")














