Download presentation
Presentation is loading. Please wait.

1
OVERDENTURE Dr Balendra Pratap Singh Assistant Professor Department of Prosthodontics

2
The continuous pattern of alveolar bone loss, once teeth have been removed have been well documented by researchers. Bone resorption is so predictable in most patients that every effort should be made to preserve root & alveolar bone.

3
Also the transition from dentulous to suddenly becoming edentulous & wearing dentures is often traumatic psychological experience for patients. Many times, patient feels that he has lost his sense of taste, smell & tactile discrimination. Covering the hard palate & other tissues blocks vast regions of nerve receptors that respond to pain, pressure.

4
However the use of tooth- supported overdentures provides retention of alveolar bone, makes possible a high degree of tactile discrimination & strongly strengthens the psychologic factors of the patient.

5
DEFINITION: (According to GPT-8) it is a removable partial denture or complete denture that covers & rest on one or more remaining natural teeth, the roots of natural teeth, or dental implant.
 it is a removable partial denture or complete denture that covers & rest on one or more remaining natural teeth, the roots of natural teeth, or dental implant.")
6
SYNONYMS 1.overlay denture ( CRUM & ROONEY) 2.overlay prosthesis 3.telescope denture ( PEREL) 4.biologic denture 5.superimposed prosthesis
 2.overlay prosthesis 3.telescope denture ( PEREL) 4.biologic denture 5.superimposed prosthesis")
8
RATIONALE

9
1.To maintain the sensory input from the PDL receptors: Sensitivity of the anterior teeth- The roots of the teeth offer more discrete discriminatory input than does the oral mucosa.

10
Dimensional perception- Means the discrimination of different thickness of objects between the occlusal surfaces of teeth. Kawamura & Wantanabe [ 1960 ] found that patient’s with natural dentition could discriminate differences at the 2mm range better than those with artificial denture.

11
Canine response- Corbin & Harisson [ 1940 ] found in their studies that canine were most sensitive oral structures. Kruger et al [ 1962 ] said that the canines had more neurons than any other teeth. These results lend support to their retention for overdentures.
![Canine response- Corbin & Harisson [ 1940 ] found in their studies that canine were most sensitive oral structures.](http://images.slideplayer.com/29/9435020/slides/slide_11.jpg "Kruger et al [ 1962 ] said that the canines had more neurons than any other teeth. These results lend support to their retention for overdentures..")
12
Directional sensitivity- Kruger & Michael [ 1962 ] reported that teeth had excellent directional sensitivity. It appears there are specific sensory Nerve endings for various kinds of force, that is lingual force or buccal force.
![Directional sensitivity- Kruger & Michael [ 1962 ] reported that teeth had excellent directional sensitivity.](http://images.slideplayer.com/29/9435020/slides/slide_12.jpg "It appears there are specific sensory Nerve endings for various kinds of force, that is lingual force or buccal force..")
13
2.To increase masticatory performance: Rissin et al [ 1971] found that the overdenture patients had a chewing efficiency 1/3 higher than the complete denture patients.
![2.To increase masticatory performance: Rissin et al [ 1971] found that the overdenture patients had a chewing efficiency 1/3 higher than the complete denture patients.](http://images.slideplayer.com/29/9435020/slides/slide_13.jpg "2.To increase masticatory performance: Rissin et al [ 1971] found that the overdenture patients had a chewing efficiency 1/3 higher than the complete denture patients.")
14
3.To preserve the alveolar bone: Even after fabrication of a CD alveolar bone resorption continues- this may be because mucosal receptors under conventional dentures during mastication are unable to warn against occlusal overloading.

16
ADVANTAGES

17
Preservation of alveolar bone- Preserving the teeth retains not only the alveolar bone surrounding the teeth but also preserves the bone adjacent to the teeth. The roots of the teeth provide tensile stimulation to residual alveolar ridge. This type of stimulation is conductive to bone repair & maintenance.

18
Preservation of proprioception- Most of the sensory inputs from the receptors in the PDL are proprioceptive signals. Periodontal receptors are largely responsible for the ability of the mandible to close directly into intercuspal position without interferences.

19
Support- The natural tooth stops of an overdenture provide for a static, stable base unparalleled by any conventional denture. A stable base such as this improves occlusion by more accurate jaw relation records.

20
Retention- Relief of some areas like bony protuberance or pronounced tissue adjacent to the teeth break the seal but the use of attachment or soft liners overcome this problem.

21
A simple approach to patient in following cases- -Cleft palate -Partial anodontia -Microdontia -Amelogenesis imperfecta

22
microdontia Partial anodontia Amelogenesis imperfecta

23
Patient acceptance- Pt’s are most receptive & appreciative of this type of treatment because they experience a striking improvement in function & esthetics while still maintaining some of their own teeth.

24
Convertibility- This concept is designed so that if for some reason the overlaid teeth must be extracted, the overdenture can be readily be converted to a conventional denture by blocking the abutment indentations or relining & rebasing.

25
Other advantages Horizontal & torqueing forces are minimized. Fewer post insertion problems as compared to conventional dentures Its application is virtually unlimited & depends on dentists skill & judgement.

26
DISADVANTAGES- More expensive because of endodontic treatment & subsequent restoration of teeth with alloys or gold. Frequently need periodontal therapy. This entails a rigid & frequent recall appointment protocol. Bulkier than FPD or RPD. If pt. does not keep the overdenture & teeth clean, caries & periodontal disease may progress. Secondary caries under the margin of the copings.

27
Available interarch space is sometimes inadequate & may require extensive abutment & design modification to expedite treatment.

28
Bony undercuts- especially those found buccally to the abutment teeth may pose problem in regard to close approximation of denture base in this area.

29
Overcontouring- at times it is necessary to excessily block existing tissue undercuts. This will lead to overcontouring.

30
Undercontouring- because of limited path of insertion & presence of bony undercut some times its necessary to underextend the denture border.

31
INDICATIONS: Presence of few healthy teeth in oral cavity. Pt. with badly attrited down teeth. Pt. with congenital or acquired intraoral defect of cleft palate, oligodontia, microdontia & cliedocranial dysostosis. Pt. with poor prognosis for complete denture like high palatal vault & steep ridge slope.

32
CONTRAINDICATIONS CONTRAINDICATIONS: When another line of treatment promises to give superior results. It is contraindicated in pt. who cannot maintain good oral hygiene to keep abutment teeth & its periodontal tissue healthy. Teeth or tooth in which periodontal or endodontic treatment is contraindicated.

33
In the mouth the attachments can be placed in either a sound natural tooth following root canal therapy for better retention OR They are place into a dental implant

34
TOOTH SUPPORTED OVERDENTURES

35
ONLAY DENTURES When a component of a partial denture extends to cover the greater portion of the occlusal or incisal surface of the tooth it is called an onlay denture. The onlay may cover one, many or all the teeth in the dental arch.

37
An onlay denture is one which is designed to alter the shape & height of the occlusal surface of the teeth over which it fits.

38
They are made of – -acrylic resin -Gold -Cr-Co alloy

39
IMMEDIATE OVERDENTURE An immediate overdenture is an overdenture constructed for insertion immediately after removal of natural teeth ADVANTAGES: Immediate overdenture have additional advantage since minimal discomfort & interference with function.

40
SELECTION OF ABUTMENT TEETH: The factors governing the selection of abutment teeth are: Periodontal status Caries index Potential for endodontic treatment Location & number of teeth: teeth should be retained in areas of anticipated bone loss. since bone loss is most rapid in anterior portion of the edentulous mandible, priority is given to the retention of the mandibular canine.

41
Ideally four teeth, one canine & one molar or premolar on each side of the mandibular arch is retained. Contiguous teeth generally are not retained, because of retaining adjacent teeth, inflammation of interdental papilla occurs more rapidly.

42
PERIODONTAL CONSIDERATION: PERIODONTAL CONSIDERATION: all periodontal disease should be treated to provide healthy environment for abutment teeth. Underlying osseous defect should be removed for proper support of abutment teeth. PRERATION OF ABUTMENT TEETH: PRERATION OF ABUTMENT TEETH:

43
ENDODONTIC CONSIDERATION: ENDODONTIC CONSIDERATION: Most of the teeth will require endodontic therapy, the endodontic prognosis must be considered. Some patient have advanced pulpal recession with extensive tooth wear, which allows for coronal reduction without the need for endodontic treatment. Endodontic implants are also used for better support & stability.

44
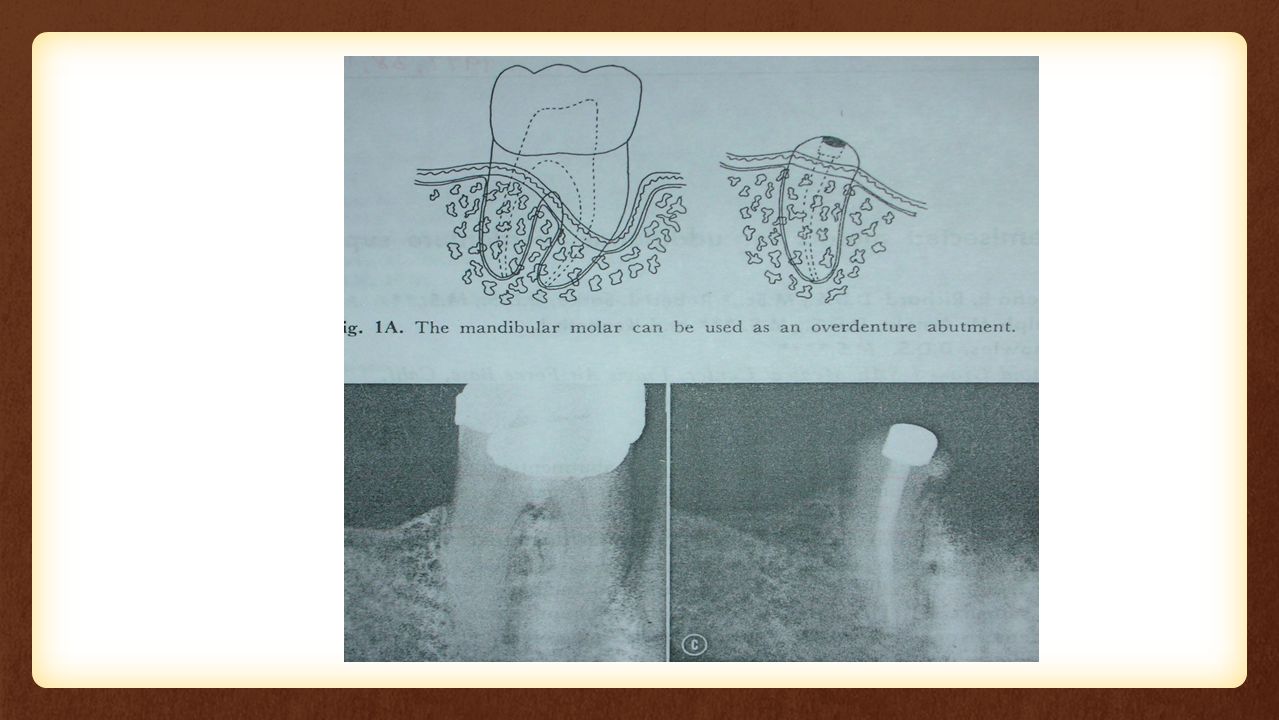
TOOTH PRERARATION: After endodontic therapy the tooth can be reduced to convex contour upto 1-2mm above the gingival margin.

45
RESTORATIVE CONSIDERATION: RESTORATIVE CONSIDERATION: After tooth reduction silver amalgam is placed in the access to root canal & dentin. Amalgam should be highly polished that allow minimum accumulation of plaque & can be easily cleaned to prevent caries of abutment teeth.

46
ABUTMENT COPING: ABUTMENT COPING: Coping is indicated when previous caries or restoration extends below the level of gingival margin. Coping is also indicated when natural teeth are present in opposing arch, severe abrasion. Coping contour are rounded to provide ball & socket contact between coping & overdenture.

47
Variations in abutments*- 1.Cast post & tall core [3- 5 mm] 2.Cast post & short core [ 2-3 mm] 3.Amalgam in prepared tooth [ 1-2 mm] *[JPD 1975, 34,135- 40]
![Variations in abutments*- 1.Cast post & tall core [3- 5 mm] 2.Cast post & short core [ 2-3 mm] 3.Amalgam in prepared tooth [ 1-2 mm] *[JPD 1975, 34, ]](http://images.slideplayer.com/29/9435020/slides/slide_47.jpg "Variations in abutments*- 1.Cast post & tall core [3- 5 mm] 2.Cast post & short core [ 2-3 mm] 3.Amalgam in prepared tooth [ 1-2 mm] *[JPD 1975, 34, ]")
48
cast post with tall core - 3-5mm

49
Cast post & short core 2-3mm

50
Amalgam in prepared tooth 1-2mm

Similar presentations










>")










