Download presentation
Presentation is loading. Please wait.

1
19 Ambulatory Care Sensitive Conditions COPD November 2015

2
19 Ambulatory Care Sensitive Conditions
Many patients present at A&E with problems which may have been avoidable if they had been managed better in the community. This is distressing for patients, but also wastes valuable A&E time and NHS money. Nineteen such 'Ambulatory Care Sensitive' conditions have been identified as ones where community care can avoid the need for hospitalisation. 19 Ambulatory care sensitive conditions COPD Pyelonephritis Angina (without major procedure) Iron-deficiency anaemia ENT infections Perforated/bleeding ulcer Convulsions and epilepsy Dental conditions Congestive heart failure Hypertension Asthma Gangrene Flu and pneumonia (>2 months old) Pelvic inflammatory disease Dehydration and gastroenteritis Vaccine-preventable conditions Cellulitis (without major procedure) Nutritional deficiencies. Diabetes with complications
 Iron-deficiency anaemia. ENT infections. Perforated/bleeding ulcer. Convulsions and epilepsy. Dental conditions. Congestive heart failure. Hypertension. Asthma. Gangrene. Flu and pneumonia (>2 months old) Pelvic inflammatory disease. Dehydration and gastroenteritis. Vaccine-preventable conditions. Cellulitis (without major procedure) Nutritional deficiencies. Diabetes with complications.")
3
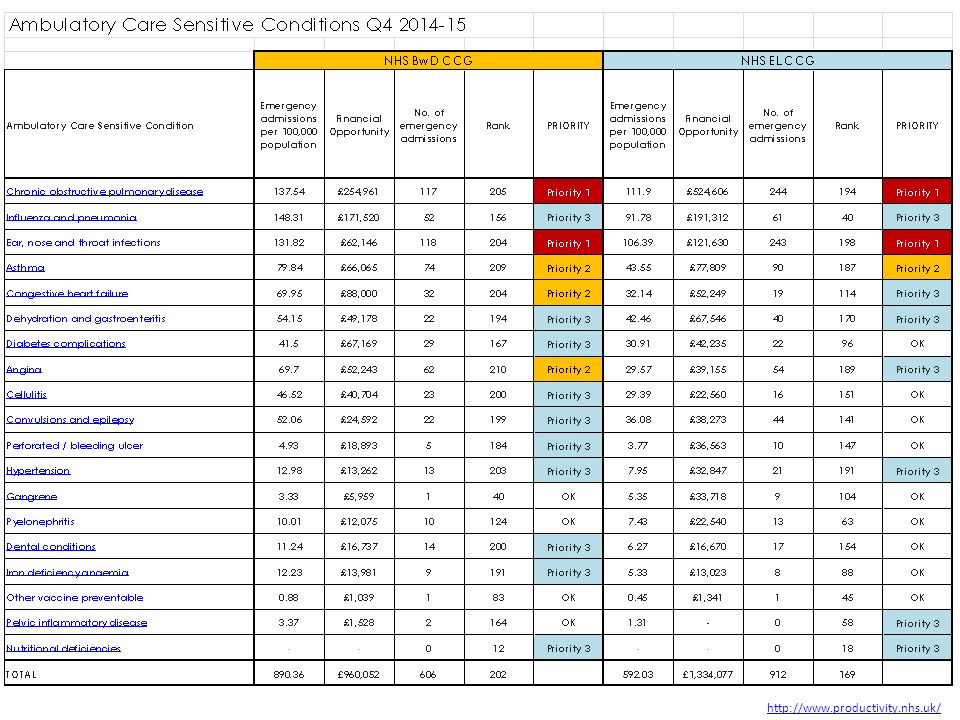
Unplanned Admissions for Chronic Ambulatory Care Sensitive Conditions : 2014-15
Locally we have some of the highest rates of admission for chronic ambulatory care sensitive conditions NHS Indicators :

4
19 Ambulatory Care Sensitive Admissions : Comparative Trends
The gap between our local position and the national position is not closing – we continue to have very high comparative admission rates.

6
the number of admissions
The 19 conditions have been classified into priority groupings based on :- the potential financial opportunity (of moving to the 50th Percentile i.e. average) the number of admissions rank position of the CCG nationally (out of 211 CCGs) A simple ‘Priority Criteria’ approach has been used to identify those areas with the greatest opportunity. These have been identified as follows. 2 x ‘Priority 1’ conditions can be identified using this approach: COPD ENT infections
 the number of admissions. rank position of the CCG nationally (out of 211 CCGs) A simple ‘Priority Criteria’ approach has been used to identify those areas with the greatest opportunity. These have been identified as follows. 2 x ‘Priority 1’ conditions can be identified using this approach: COPD. ENT infections.")
7
Clear age profile linked to conditions
ENT : Mainly 0-4 ages Asthma : <15’s account for 50% of activity COPD : mainly patients aged 55 and over

8
COPD [BwD CCG + EL CCG Combined]
Mainly patients aged 55 and over Average LOS over 5 days – including many patients with no primary procedure reported (80-90% of admissions have no primary procedure) 135 of the 697 patients (19.4%) have 2 or more admissions during the first 6 months of 85% of emergency admissions are coming via A&E Clear seasonal pattern with increases in admission during the winter months
![COPD [BwD CCG + EL CCG Combined]](http://slideplayer.com/slide/9432211/29/images/8/COPD+%5BBwD+CCG+%2B+EL+CCG+Combined%5D.jpg "Mainly patients aged 55 and over. Average LOS over 5 days – including many patients with no primary procedure reported (80-90% of admissions have no primary procedure) 135 of the 697 patients (19.4%) have 2 or more admissions during the first 6 months of % of emergency admissions are coming via A&E. Clear seasonal pattern with increases in admission during the winter months.")
9
Emergency Admissions : Patients aged 65+ COPD
COPD in 65+ shows a winter seasonality with increased admissions in ‘Winter’…mainly via A&E Respiratory admissions for 65+ spike significantly in winter

10
Insights from Central Lancashire
Emma Foster, Network Director for Adult Community Services, LCFT Elizabeth Fleming, Head of Urgent Care, Pennine Lancashire CCGs

11
Contextext Our journey so far as part of the Central Lancashire Health and Social Care – Whole System Transformation Programme... Top 10 ACS Conditions analysis using NHS Better Care, Better Value Indicators ACS conditions 2013/14 LTH non-elective admissions NHS better care, better value indicator at 25th percentile benchmark Potential admissions opportunity Reduction (%) Potential financial opportunity (£) Influenza and pneumonia 907 426 47% 1,365,757 COPD 1,080 528 49% 1,127,850 Dehydration and gastroenteritis 1,030 515 50% 765,488 Cellulitis 602 342 57% 568,696 Congestive heart failure 457 152 33% 423,149 Ear, Nose & Throat (ENT) 1,052 739 70% 403,972 Angina 603 421 328,356 Diabetes complications 294 122 42% 267,244 Asthma 474 307 65% 257,427 Convulsions and epilepsy 275 140 51% 152,525 Total 6,774 3,692 54% 5,660,466 19 Ambulatory Care Sensitive Conditions WHY? Prevalence LoS Number of admissions Clinical opinion National data Prioritised 10 Local Ambulatory Care Sensitive Conditions Jan’14 Apr’14 Apr’15 LoS (0-1) 279 LoS (2-7) 487 LoS (7+) 314 Total Admissions 1,080 Influenza, Pneumonia COPD Dehydration & Gastroenteritis CHF Cellulitis ENT Angina Diabetes Asthma Convulsion & Epilepsy Tranche 1 Tranche 2 Tranche 3 GUIDING PRINCIPLES FOR IMPLEMENTATION
 Potential financial opportunity (£) Influenza and pneumonia % 1,365,757. COPD. 1, % 1,127,850. Dehydration and gastroenteritis. 1, % 765,488. Cellulitis % 568,696. Congestive heart failure % 423,149. Ear, Nose & Throat (ENT) 1, % 403,972. Angina ,356. Diabetes complications % 267,244. Asthma % 257,427. Convulsions and epilepsy % 152,525. Total. 6,774. 3, % 5,660, Ambulatory Care Sensitive Conditions. WHY Prevalence. LoS. Number of admissions. Clinical opinion. National data. Prioritised 10 Local Ambulatory Care Sensitive Conditions. Jan’14 Apr’14 Apr’15. LoS (0-1) 279. LoS (2-7) 487. LoS (7+) 314. Total Admissions 1,080. Influenza, Pneumonia. COPD. Dehydration & Gastroenteritis. CHF. Cellulitis. ENT. Angina. Diabetes. Asthma. Convulsion & Epilepsy. Tranche 1. Tranche 2. Tranche 3. GUIDING PRINCIPLES FOR IMPLEMENTATION.")
13
Monthly Diabetic Medicine and Respiratory Medicine Outpatients - CSR/GP CCGs

14
COPD Intensive Home Support 7 day
Jul 14 Aug Sept Oct Nov Dec Jan 15 Feb Mar Apr May June July Sep BCBV QP CQUIN Mortality alert COPD Consultant Go live Cardio-resp team COPD Intensive Home Support 7 day Ambulatory Care Pathway NWAS CCPs Quadramed marker Rehabilitation Expansion BTS Care Bundles Pilot GSF MDTs For 70 beds 8-8: Part of 8a as service manager 2 x Band 7 WTE 4-5 x Band 6 WTE

18
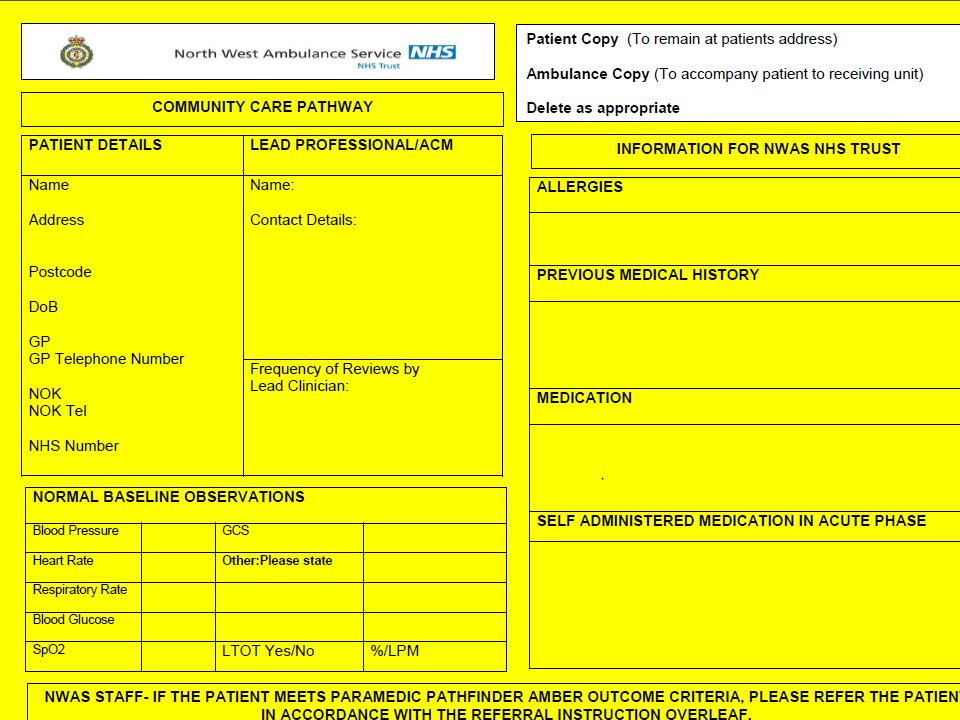
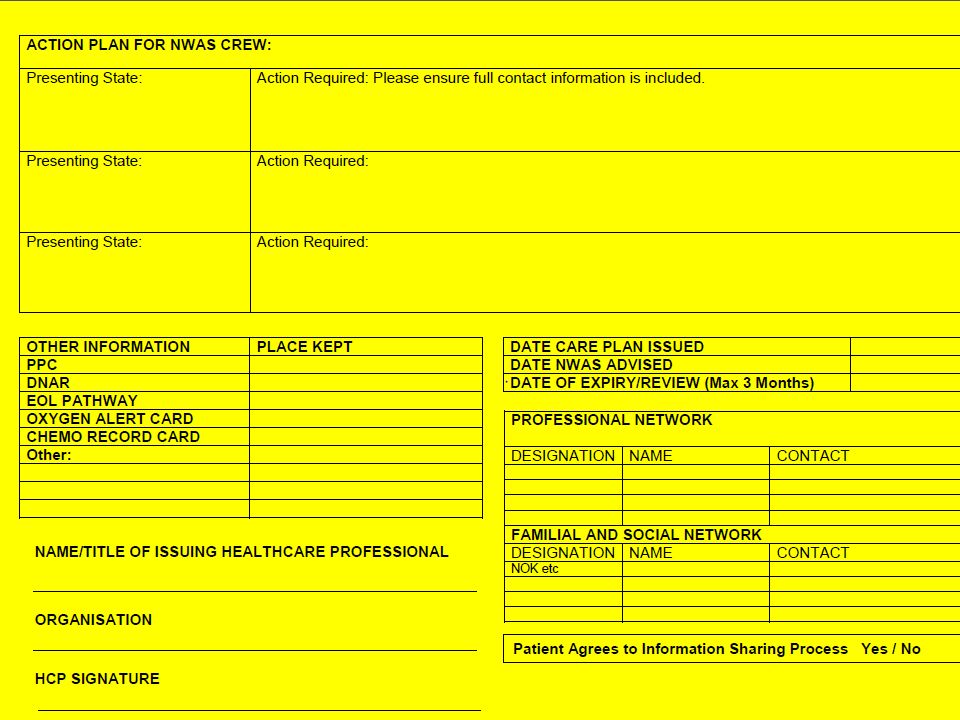
999 ED Patient GP UCC COPD Intensive Home Support
Primary care visiting scheme COPD Intensive Home Support ED Admit Patient COPD Intensive Home Support GP Admit via MAU COPD Intensive Home Support UCC Admit

19
58% of referrals were for admission avoidance
15% of referrals from primary care (GPs and Practice Nurses) with two thirds of the primary care referrals from Chorley. The Chorley bias has also been the case previously 43% of referrals from community (patient self referrals, LCFT teams) with an even locality split 42% of referrals were from LTH with an even split between localities 29% of referrals were for supported discharge from hospital wards 13% of referrals were from ED or MAU to avoid ward admission
 with two thirds of the primary care referrals from Chorley. The Chorley bias has also been the case previously. 43% of referrals from community (patient self referrals, LCFT teams) with an even locality split. 42% of referrals were from LTH with an even split between localities. 29% of referrals were for supported discharge from hospital wards. 13% of referrals were from ED or MAU to avoid ward admission.")
20
From July 14 to June 15 there were 1164 referrals for COPD HIS (avg
From July 14 to June 15 there were 1164 referrals for COPD HIS (avg. 97 p.m.) Referral pattern shows expected seasonal variation Referral split shows slight bias towards Chorley 645 (55%); Preston 519 (45%)
 Referral pattern shows expected seasonal variation. Referral split shows slight bias towards Chorley 645 (55%); Preston 519 (45%)")
21
Data parameters Primary diagnosis of COPD. Diagnosis codes used are taken from Everyone Counts Guidance which include: J20 Acute bronchitis* J41 Simple and mucopurulent chronic bronchitis J42X Unspecified chronic bronchitis J43 Emphysema J44 Other chronic obstructive pulmonary disease J47X Bronchiectasis *J20 only with second diagnosis of J41, J42, J43, J44, J47 Admissions from all Lancashire CCGs into LTHTr

22
July June admissions with primary diagnosis of COPD and an average of 88 admissions per month July June admissions with primary diagnosis of COPD and an average of 81 admissions per month If December and January had been at ‘normal’ activity levels then there would have been 931 admissions between July 2014 and June 2015 Poor efficacy of flu vaccination is the likely cause for the rise in admissions over Dec and Jan

23
July 2013- June 2014 average LOS (primary diagnosis of COPD) 9
July June 2014 average LOS (primary diagnosis of COPD) 9.2 days July June 2015 average LOS (primary diagnosis of COPD) 7.2 days
 9.2 days July June 2015 average LOS (primary diagnosis of COPD) 7.2 days.")
24
July 2013- June 2014 average number of readmissions per month 17
July June 2014 average number of readmissions per month 17.1 July June 2015 average number of readmissions per month 15.7

25
What worked well? Key Clinical Leadership Senior Leadership
Collaboration and trust Desire to work in an integrated way (specialist team) Desire to work in a different way Open referral pathway Focused efforts and momentum Invest to save
 Desire to work in a different way. Open referral pathway. Focused efforts and momentum. Invest to save.")
26
Further opportunities
Extended primary care network High intensity users How do specialist and generalist service integrate? Cost-effective interventions Spirometry End of life care

27
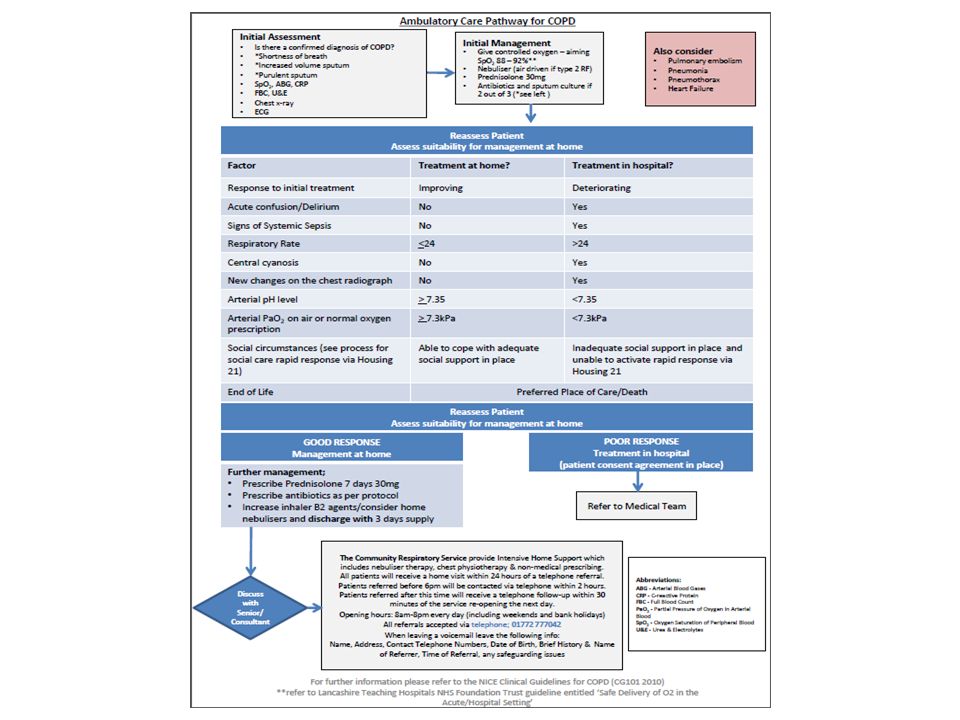
NICE Clinical Guideline 101

28
Questions please?

Similar presentations




 Dr Ian Williams Greater Metro South Brisbane Medicare.>")













 1.>")

