Download presentation
Presentation is loading. Please wait.

1
Care of Patients with Acute Coronary Syndromes ~ Every 25 seconds a person in the United States has a major coronary event ~ Every minute someone will die due to a coronary event

2
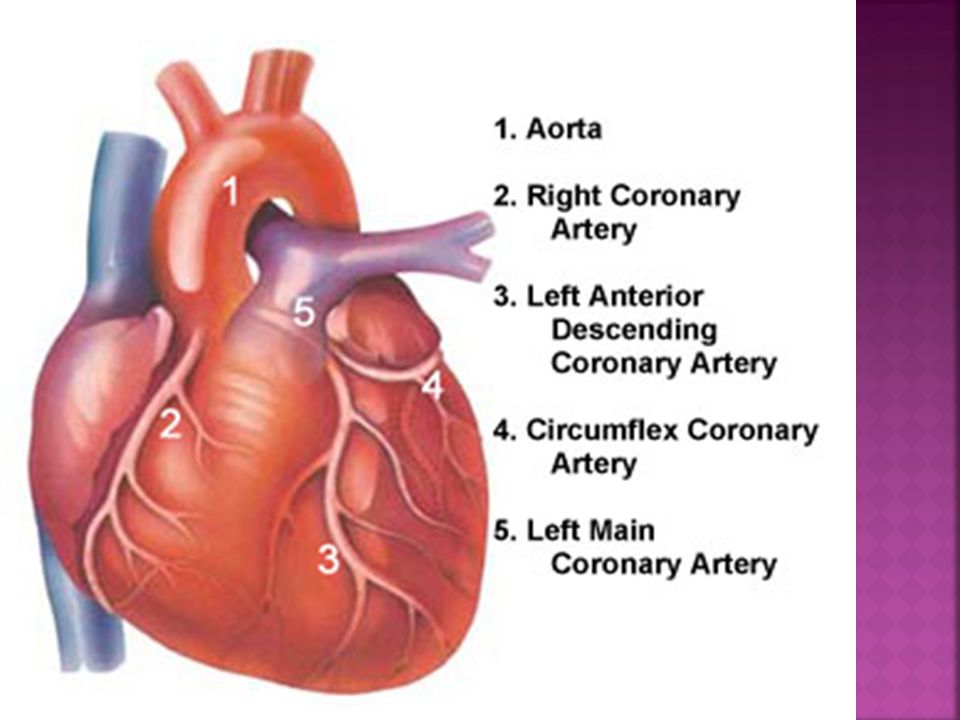
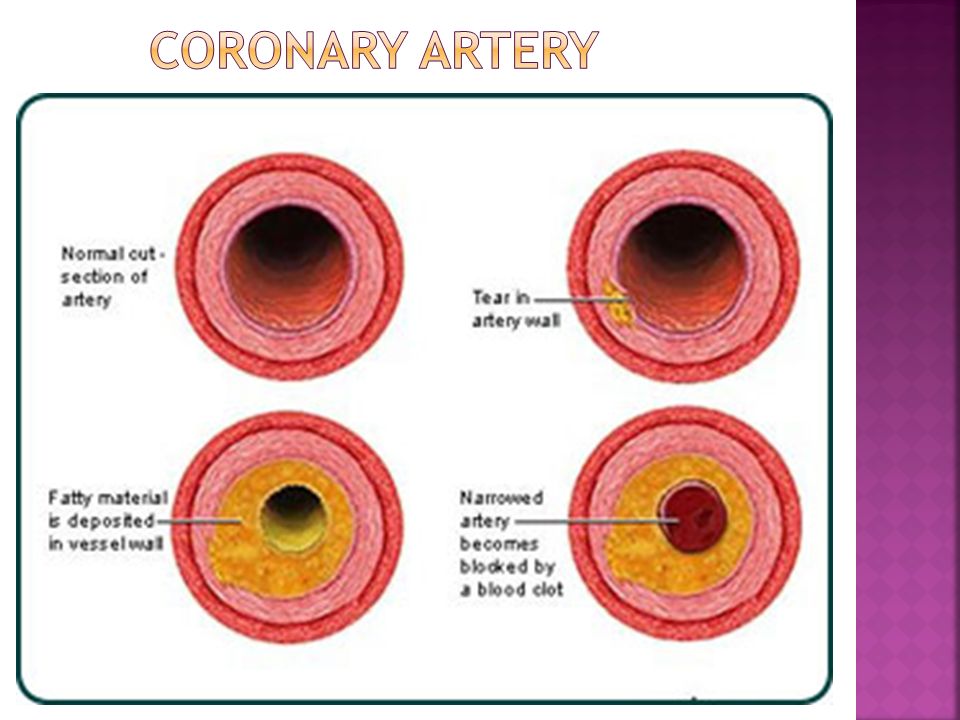
Includes stable angina and acute coronary syndromes Ischemia—insufficient oxygen supply to meet the requirements of the myocardium Infarction—necrosis or cell death that occurs when severe ischemia is prolonged and decreased perfusion causes irreversible damage to tissue

5
Temporary imbalance between the coronary artery’s ability to supply oxygen and the cardiac muscle’s demand for oxygen Ischemia limited in duration and does not cause permanent damage to myocardial tissue Chronic stable angina- progresses to: Unstable angina

6
Patients who present with either unstable angina or an acute myocardial infarction ST elevation MI (STEMI) traditional manifestation Non–ST elevation MI (non-STEMI) common in women
 traditional manifestation Non–ST elevation MI (non-STEMI) common in women")
7
New-onset angina - First symptoms, usually after exertion Variant (Prinzmetal’s) angina - usually a coronary spasm, occurs at rest Pre-infarction angina - Chest pain occurring prior to MI Causes severe activity limitation
 angina - usually a coronary spasm, occurs at rest Pre-infarction angina - Chest pain occurring prior to MI Causes severe activity limitation")
8
MI is the most serious acute coronary syndrome Occurs when myocardial tissue is abruptly and severely deprived of oxygen Occlusion of blood flow Necrosis Hypoxia Locations: i.e. inferior, anterior, lateral, posterior, septal Ventricular remodeling

9
EKG changes seen with Myocardial Infarction

10
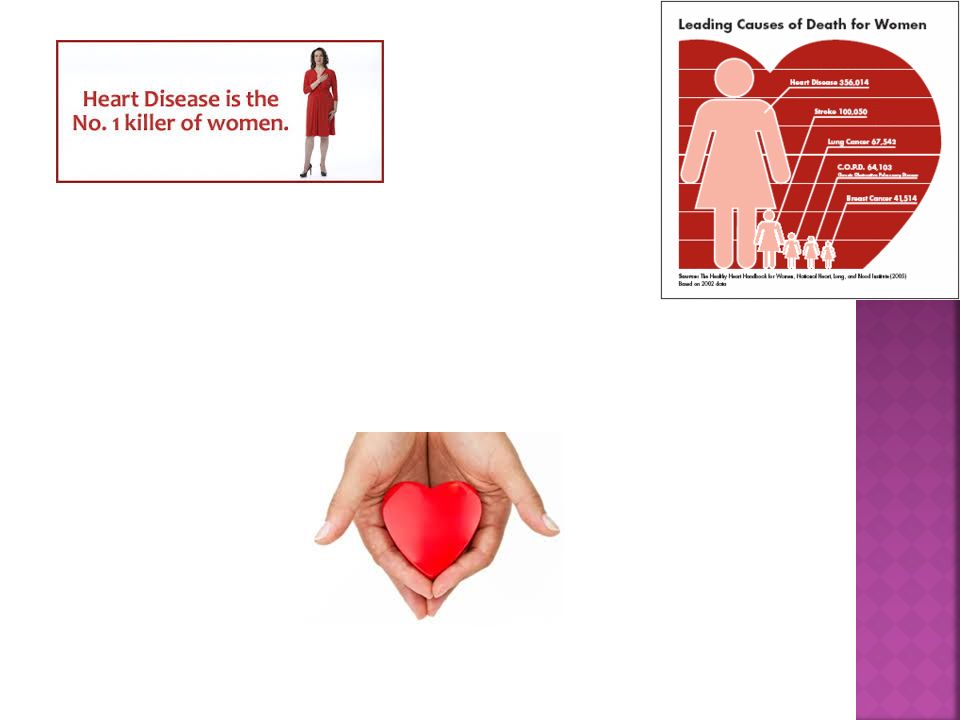
Age Gender (women develop CAD 10 years later than men and have higher incidence of death during hospitalization) Family history = high risk Ethnic background
 Family history = high risk Ethnic background")
11
Elevated serum cholesterol Cigarette smoking Hypertension Impaired glucose tolerance Obesity Physical inactivity Stress

12
Delay interview data collection until interventions for symptom relief, vital instability, and dysrhythmias are resolved Rapid assessment is crucial to determine characteristics of the discomfort. Interview: 1. onset 2. location 3. radiation 4. intensity 5. duration 6. precipitating and relieving factors

13
Nausea/vomiting Diaphoresis Dizziness Weakness Palpitations Shortness of air Skin color ashen Sense of impending doom Decreased distal peripheral pulses Auscultate for extra heart sounds Watch for denial, fear, anxiety, and anger

15
Troponin T and troponin I Creatine kinase-MB (CK-MB) Myoglobin Imaging assessment (exercise stress test, echocardiogram) 12-lead electrocardiograms Cardiac catheterization
 Myoglobin Imaging assessment (exercise stress test, echocardiogram) 12-lead electrocardiograms Cardiac catheterization")
16
EKG changes seen with Myocardial Infarction

17
Interventions include: Provide pain-relief modalities, drug therapy Decrease myocardial oxygen demand Increase myocardial oxygen supply

18
Nitroglycerine Morphine sulfate Oxygen Position of comfort; semi-Fowler’s position Quiet and calm environment Deep breaths to increase oxygenation

19
Correct order: 1. Oxygen 2. Nitro 3. Aspirin 4. Morphine

20
Interventions include: Drug therapy (aspirin, thrombolytic agents) Restoration of perfusion to the injured area often limits the amount of extension and improves left ventricular function Complete sustained reperfusion of coronary arteries in the first few hours after an MI has decreased mortality
 Restoration of perfusion to the injured area often limits the amount of extension and improves left ventricular function Complete sustained reperfusion of coronary arteries in the first few hours after an MI has decreased mortality")
21
Glycoprotein (GP) IIB/IIIa inhibitors (Integrillin) decrease thrombus formation Once-a-day beta-adrenergic blocking agents – (Coreg) (decrease size of infarct and decrease mortality) Angiotensin-converting enzyme inhibitors (ACE) or angiotensin receptor blockers (prevent ventricular remodeling, and increase survival rate) Calcium channel blockers (vasodilatory for angina) Ranolazine (anti anginal for CSA)
 IIB/IIIa inhibitors (Integrillin) decrease thrombus formation Once-a-day beta-adrenergic blocking agents – (Coreg) (decrease size of infarct and decrease mortality) Angiotensin-converting enzyme inhibitors (ACE) or angiotensin receptor blockers (prevent ventricular remodeling, and increase survival rate) Calcium channel blockers (vasodilatory for angina) Ranolazine (anti anginal for CSA)")
22
Fibrinolytics dissolve thrombi in the coronary arteries and restore myocardial blood flow Tissue plasminogen activator (TPA) Reteplase Tenecteplase (TNK) 5 sec IVP Note: Heparin gtt follows therapy to prevent clots
 Reteplase Tenecteplase (TNK) 5 sec IVP Note: Heparin gtt follows therapy to prevent clots")
24
Cardiac Rehabilitation Phase 1- acute illness through discharge Phase 2- discharge through home convalescence Phase 3- long term conditioning

25
Assess the patient’s level of anxiety, and allow expression of any anxiety; and attempt to define its origin Give simple explanations of therapies, expectations, and surroundings and explanations of progress to help relieve anxiety Provide coping enhancement - LISTEN

26
Dysrhythmias are the leading cause of death in most patients with MI, who die before they can be hospitalized Interventions include: Identify the dysrhythmias Assess hemodynamic status Evaluate for discomfort

27
Necrosis of more than 40% of the left ventricle Tachycardia Hypotension Blood pressure <90 mm Hg or 30 mm Hg less than patient’s baseline Urine output <30 mL/hr (sign of inadequate organ perfusion)
")
28
Cold, clammy skin Poor peripheral pulses Agitation, restlessness, confusion Pulmonary congestion Tachypnea Continuing chest discomfort Early detection is essential as diagnosed cardiogenic shock has a high mortality rate

29
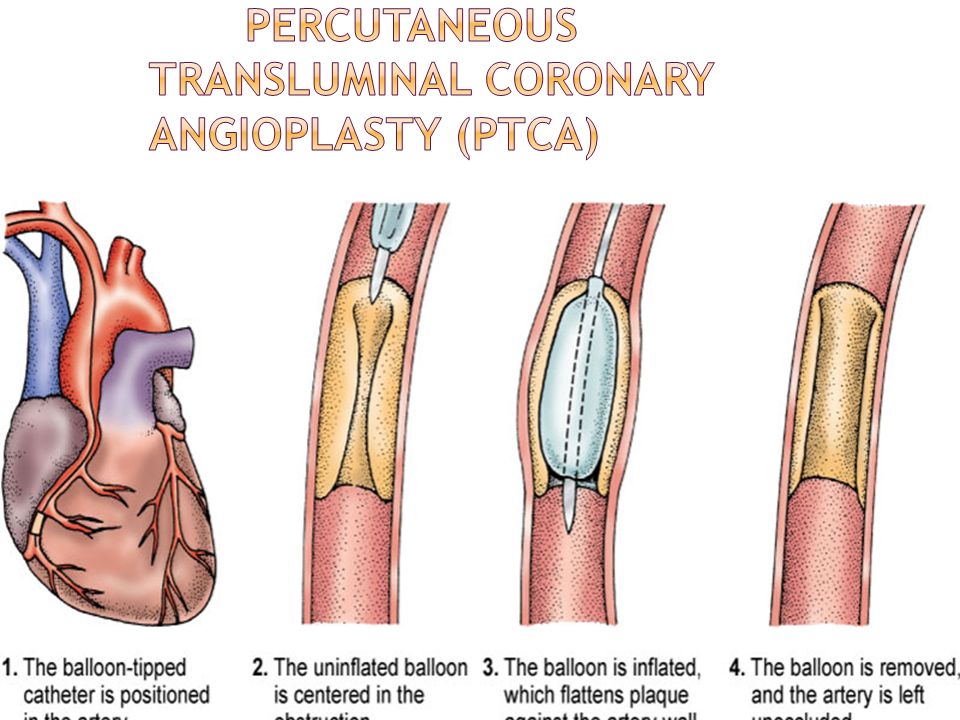
Pain relief with Morphine, and decreased myocardial oxygen requirements through preload and afterload reduction (swan ganz catheter insertion for measurements to guide fluid and vasoactive drug administration Drug therapy- nitrates, diuretics, beta blockers, positive inotropes, i.e: Dobutamine Intra-aortic balloon pump to improve perfusion when drug therapy ineffective Immediate reperfusion – pt taken to cath lab for PTCA

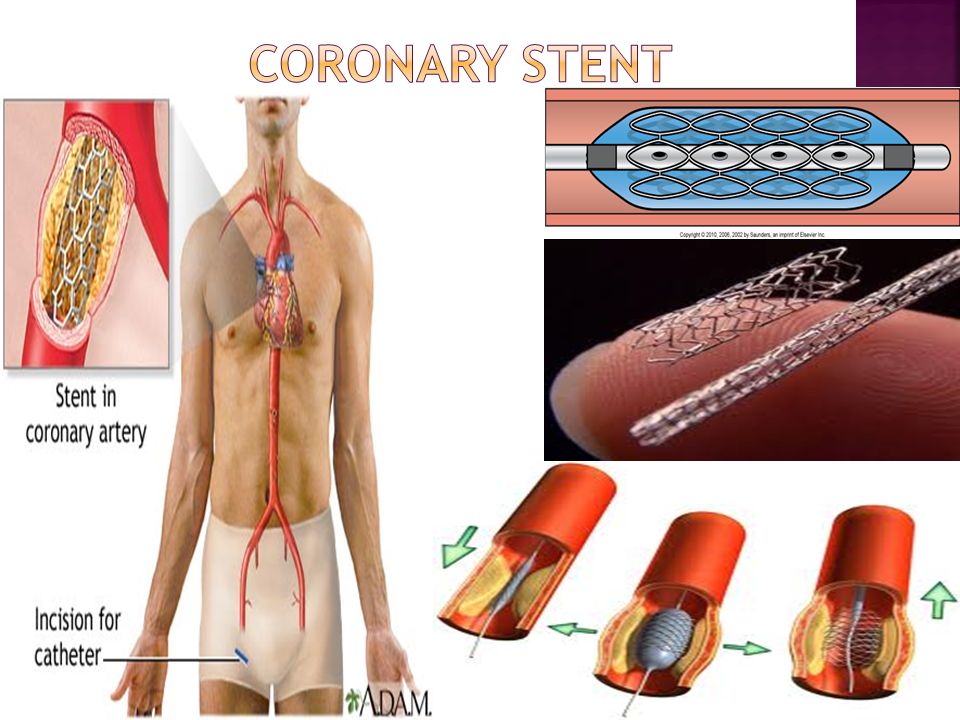
30
Clopidogrel (Plavix) before the procedure IV heparin after the procedure IV or intracoronary nitroglycerine or diltiazem Possible IV GP IIb/IIIa inhibitors (Integrillin) Long-term therapy: antiplatelet therapy, beta blocker, ACE inhibitor or ARB
 before the procedure IV heparin after the procedure IV or intracoronary nitroglycerine or diltiazem Possible IV GP IIb/IIIa inhibitors (Integrillin) Long-term therapy: antiplatelet therapy, beta blocker, ACE inhibitor or ARB")
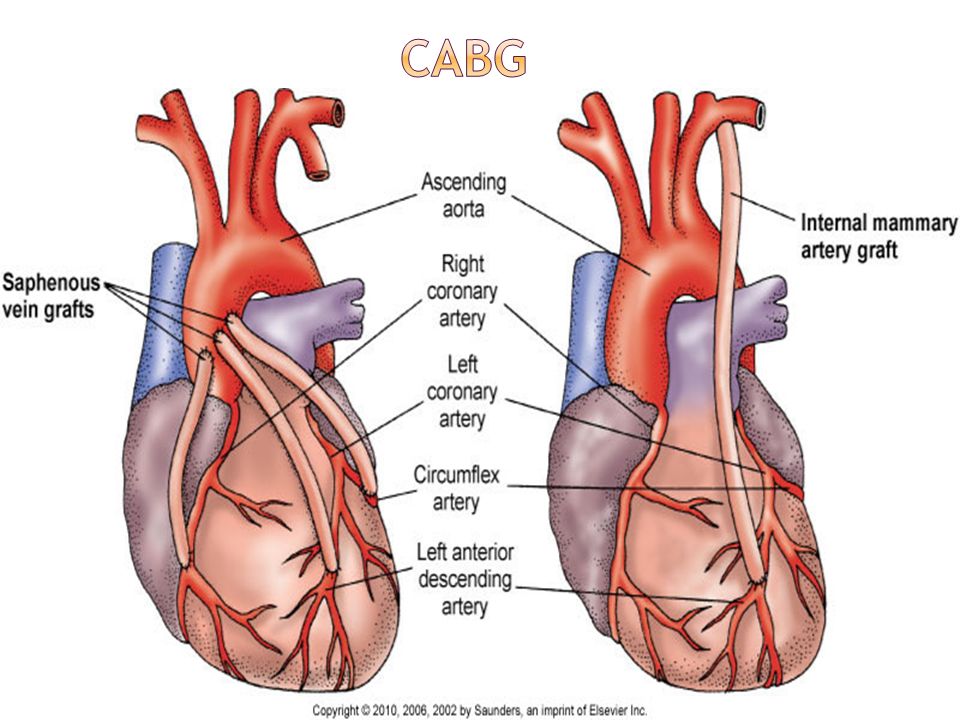
32
Candidates: Angina with >50% occlusion LMA Unstable angina with severe vessel disease Acute MI with cardiogenic shock Coronary vessels are unsuitable for PTCA

34
Operative care: Pt has sternal incision, large leg incision (usually), 2 or 3 chest tubes, mediastinal tubes, foley cather, pacemaker wires and swan ganz, and will be on a ventilator Post operative care: Pt is 1:1 care in ICU on vent approx 6 hrs. Manage fluid and electrolyte balance and cardiac rhythm closely Management of other complications: a. hypotension b. hypothermia c. hypertension d. bleeding e. cardiac tamponade f. change in level of consciousness

Similar presentations









) Dr. Walaa Nasr Lecturer of Adult Nursing Second year Second.>")



 Definition of ACS Signs and symptoms of ACS Gender and age related difference in ACS Pathophysiology.>")

 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")



