Download presentation
Presentation is loading. Please wait.

1
Alberto Repossini, Thierry A Folliguet
A Multicenter Propensity-score Analysis Of 991 Patients With Severe Aortic Stenosis And Intermediate-high Risk Profile: Conventional Surgery versus SuturelessValves versus TAVR Claudio Muneretto, Ottavio Alfieri, Michele De Bonis, Roberto Di Bartolomeo, Gianluigi Bisleri, Carlo Savini, Gianluca Folesani, Lorenzo Di Bacco, Manfredo Rambaldini, Juan Pablo Maureira, FrancoisLaborde, Maurizio Tespili, Alberto Repossini, Thierry A Folliguet Universityof Brescia MedicalSchool,, Italy, San Raffaele University Hospital, Italy, Universityof Bologna, Italy,Azienda Ospedaliera Carlo Poma, Italy, CHU de Nancy, France, InstitutMutualiste Montsouris, France, Ospedale Bolognini di Seriate, Italy, CentreHospital-UniversitaireBrabois ILCV, France

2
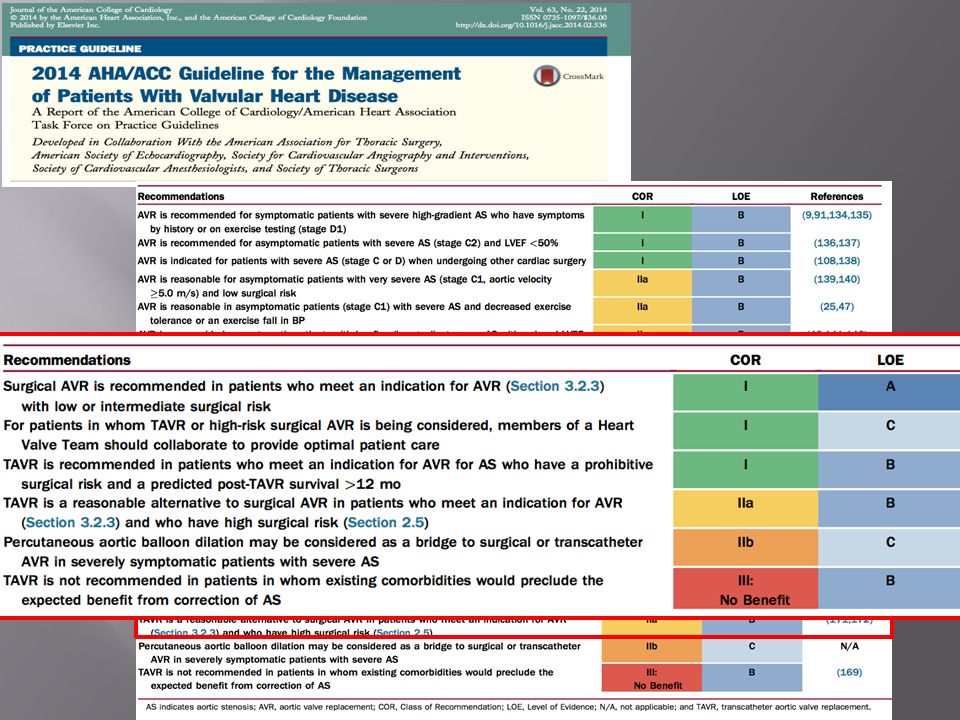
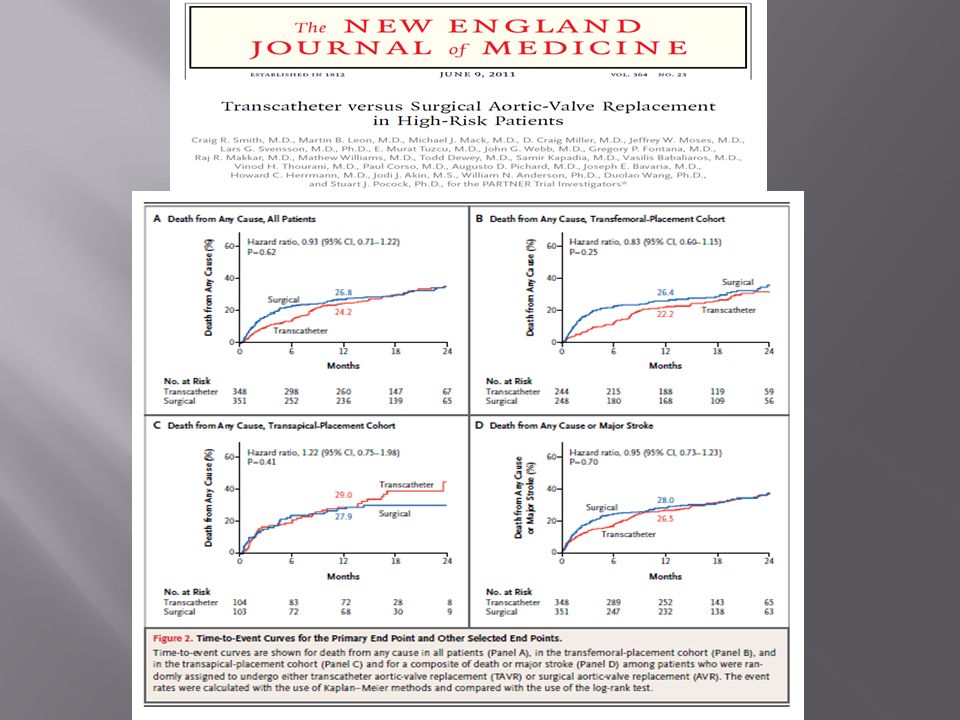
Background Surgery(SVR) is still the gold standard in the treatment of severe aortic stenosis TAVR has proved as an effective alternative in inoperable or high risk patients. Recent trend to extend the use of TAVR in patients with intermediate risk profile Sutureless valve recently become a valuable tool to reduce invasiveness, aortic cross-clamp and CPB time DivisionofCardiacSurgery–Universityof Brescia MedicalSchool

4
DivisionofCardiacSurgery–Universityof Brescia MedicalSchool

5
STS/ACC TVT Registry

6
AVR AVR AVR AVR

7
Study population 163 matched Patients AVR (Group 1) 55 patients
255 Consecutive patientswith severe aortic valve stenosis 163 matched Patients AVR (Group 1) 55 patients PERCEVAL (Group 2) 53 patients TAVR (Group 3) 55 patients
 55 patients. PERCEVAL. (Group 2) 53 patients. TAVR. (Group 3) 55 patients.")
9
Study Design 1:1:1propensity score matching
991 intermediate-high risk patients with severe aortic valve stenoses conventional surgery vs sutureless valve vs TAVR 8 European centers 1:1:1propensity score matching

10
Post-Match population intermediate-high risk patients
612 intermediate-high risk patients Group 1: Surgical AVR 204 pts Group 2: Sutureless valve 204 pts Group 3: TAVR 204 pts DivisionofCardiacSurgery–Universityof Brescia MedicalSchool

11
Post-Match population
AVR (204 pts) n (%) Sutureless (204pts) TAVR p-value AGE (yrs) 80±3 79±4 80±2 0.07 EF 54,7±5,1 55,1±7,3 54,6±6,8 0.1 EuroSCORE I log 19,2±7,4 18,9±5,9 19,5±6,7 0.34 STS score 8,3±4,4 7,9±3,2 8,2±4,2 0.2 BMI 26,8±3,2 27,1±2,8 26,9±5,3 0.52 FEMALE GENDER 98 (48%) 105 (51,4%) 91 (44,6%) 0.08 HYPERTENSION 135 (66,1%%) 138 (67,6%) 129 (63,2%) 0.35 DYSLIPIDEMIA 48 (23,5%) 45 (22%) 51 (25%) 0.56 COPD 54 (26,4%) 49 (24%) 56 (27,4%) 0.53 PREVIOUS PCI 19 (9,3%) 24 (12%) 27 (13,2%) 0,32 PREVIOUS AMI 17 (8,5%) 12 (6%) 15 (7,5%) 0.22 CAD 49 (24,0%) 42 (20,6%) 53 (25,9%) 0.18 CVA 22 (10,7%) 25 (12,2%) 28 (13,6%) 0.65 PAD 46 (22,6%) 40 (19,6%) 43 (21%) 0.7 DIABETES 57 (28%) 62 (30,3%) 0.11 NYHA III-IV 125 (61,2%) 130 (64%) 137 (67,1%) 0.14 CRF 37 (18,1%) 31 (15,2%) 44 (21,6%) 0.09 REDO 16 (7,8%) 30 (14,7%) 0.056
 n (%) Sutureless. (204pts) TAVR. p-value. AGE (yrs) 80±3. 79±4. 80± EF. 54,7±5,1. 55,1±7,3. 54,6±6, EuroSCORE I log. 19,2±7,4. 18,9±5,9. 19,5±6, STS score. 8,3±4,4. 7,9±3,2. 8,2±4, BMI. 26,8±3,2. 27,1±2,8. 26,9±5, FEMALE GENDER. 98 (48%) 105 (51,4%) 91 (44,6%) HYPERTENSION. 135 (66,1%%) 138 (67,6%) 129 (63,2%) DYSLIPIDEMIA. 48 (23,5%) 45 (22%) 51 (25%) COPD. 54 (26,4%) 49 (24%) 56 (27,4%) PREVIOUS PCI. 19 (9,3%) 24 (12%) 27 (13,2%) 0,32. PREVIOUS AMI. 17 (8,5%) 12 (6%) 15 (7,5%) CAD. 49 (24,0%) 42 (20,6%) 53 (25,9%) CVA. 22 (10,7%) 25 (12,2%) 28 (13,6%) PAD. 46 (22,6%) 40 (19,6%) 43 (21%) 0.7. DIABETES. 57 (28%) 62 (30,3%) NYHA III-IV. 125 (61,2%) 130 (64%) 137 (67,1%) CRF. 37 (18,1%) 31 (15,2%) 44 (21,6%) REDO. 16 (7,8%) 30 (14,7%)")
12
Primary Endpoints Secondary Endpoints
All-cause 30 days mortality Overall survival at 24 months Secondary Endpoints Composite Endpoint (MACCE) according to VARC criteria including AR ≥ Grade II at 24 months DivisionofCardiacSurgery – Universityof Brescia MedicalSchool
 according to VARC criteria including AR ≥ Grade II at 24 months. DivisionofCardiacSurgery – Universityof Brescia MedicalSchool.")
13
Preoperative Ao Gradient/Area (ECHO)
P=NS P=0.01 P=NS Division of Cardiac Surgery – University of Brescia Medical School

14
INTRA-OPERATIVE DATA p<0.001 p<0.001 p<0.001 DivisionofCardiacSurgery – Universityof Brescia MedicalSchool

15
POST-OPERATIVE Gradient/AR

16
IN-HOSPITAL OUTCOME

17
MACCE AT F-UP (VARC) p<0.001 p=0.028 p=0.055
 p<0.001 p=0.028 p=0.055")
18
p<0.001 TAVR vs SUTURELESS OverallSurvival TAVR vs AVR p<0.001

19
FREEDOM FROM MACCE (including AR ≥ 2)
")
20
CoxRegressionAnalysis
OverallSurvival (HR: 2.5; CI ) Division of Cardiac Surgery – University of Brescia Medical School
 Division of Cardiac Surgery – University of Brescia Medical School.")
21
Conclusions Patients with severe aortic stenosis and intermediate risk profile undergoing TAVR showed a significant worse outcome when compared with conventional surgery and sutureless valve At the multivariate analysis TAVR was identified as an independent predictor of death (HR 2.5) The deliberate use of TAVR in this specific subset of patients shoud be restricted in further, independent CRTs TAVR Division of Cardiac Surgery – University of Brescia Medical School
 The deliberate use of TAVR in this specific subset of patients shoud be restricted in further, independent CRTs. TAVR. Division of Cardiac Surgery – University of Brescia Medical School.")
22
Thanks Participating Centers
Universityof Brescia MedicalSchool, Italy, San Raffaele University Hospital, Milan, Italy, Universityof Bologna, Italy, Azienda Ospedaliera Carlo Poma, Mantova, Italy, CHU Nancy, France, InstitutMutualiste Montsouris, Paris, France, Ospedale Bolognini Seriate, Italy, Centre Hospital-UniversitaireBrabois ILCV, Vandoeuvreles Nancy, France

23
All-cause30-days mortality
All-cause 1-year mortality

24
All-causedeath Stroke or TIA All–causedeath and Stroke or TIA

27
Meanlogistic EURO Score
TV TAVI TA TAVI AVR without CABG AVR with CABG AGE > 75 86.3% 84.0% 33.3% 44.9% Meanlogistic EURO Score 25.9% 24.5% 8.8% 11% 9985 conventional AVR patients (with or withoutassociated CABG) and TAVI patients (TransVascular/TransApical) Surgical AVR hasoptimalresults in everyriskcategory
 and 3875 TAVI patients (TransVascular/TransApical) Surgical AVR hasoptimalresults in everyriskcategory.")
28
Incidence of post-operative complicationhigher in TAVI group
Higherincidence of paravalvularleak, in particular in TAVI transvalvulargroup TAVR may be an alternative only in high riskpatients with contraindications for surgery

29
EARLY POST-OPERATIVE AVR SUTURELESS TAVR P-VALUE BLEEDING REQUIRING REVISION 6 (3%) 10 (4,8%) 0 (0%) 0.008 ANAEMIA REQUIRING AT LEAST 2 UNITS OF RBC 116 (57%) 73 (35,7%) 67 (32,8%) <0.001 ACUTE RENAL FAILURE 30 (14,7%) 11 (5,3%) 24 (11,7%) 0.007 CVVH 7 (3,4%) 3 (1,5%) 12 (5,8%) 0.06 STROKE 6 (2,9%) 4 (1,9%) 0.6 PERIPHERAL VASCULAR COMPLICATIONS 20 (9,8%) PM IMPLANTATION 8 (3,9%) 30 (14.7%) HOSPITAL MORTALITY 20 (9.8%) 0.005 Division of Cardiac Surgery – University of Brescia Medical School
 ANAEMIA REQUIRING AT LEAST 2 UNITS OF RBC. 116 (57%) 73 (35,7%) 67 (32,8%) < ACUTE RENAL FAILURE. 30 (14,7%) 11 (5,3%) 24 (11,7%) CVVH. 7 (3,4%) 3 (1,5%) 12 (5,8%) STROKE. 6 (2,9%) 4 (1,9%) 0.6. PERIPHERAL VASCULAR COMPLICATIONS. 20 (9,8%) PM IMPLANTATION. 8 (3,9%) 30 (14.7%) HOSPITAL MORTALITY. 20 (9.8%) Division of Cardiac Surgery – University of Brescia Medical School.")
30
DivisionofCardiacSurgery–Universityof Brescia MedicalSchool

Similar presentations















>")



 with transcatheter aortic valve replacement (TAVR) in high-risk patients with severe.>")


