Download presentation
Presentation is loading. Please wait.

1
ANNA SAMANTHA IMPERIAL MD 070020 Dazed, lost and confused

2
History

3
General Data DS 65 year old Female April 20, 1945 Filipino Roman Catholic Pasig City Informant: Herself and her husband, Cipriano Santiago Good reliability: Husband> wife (80% and 70% respectively)
")
4
Chief Complaint “Numbness of the left hand”

5
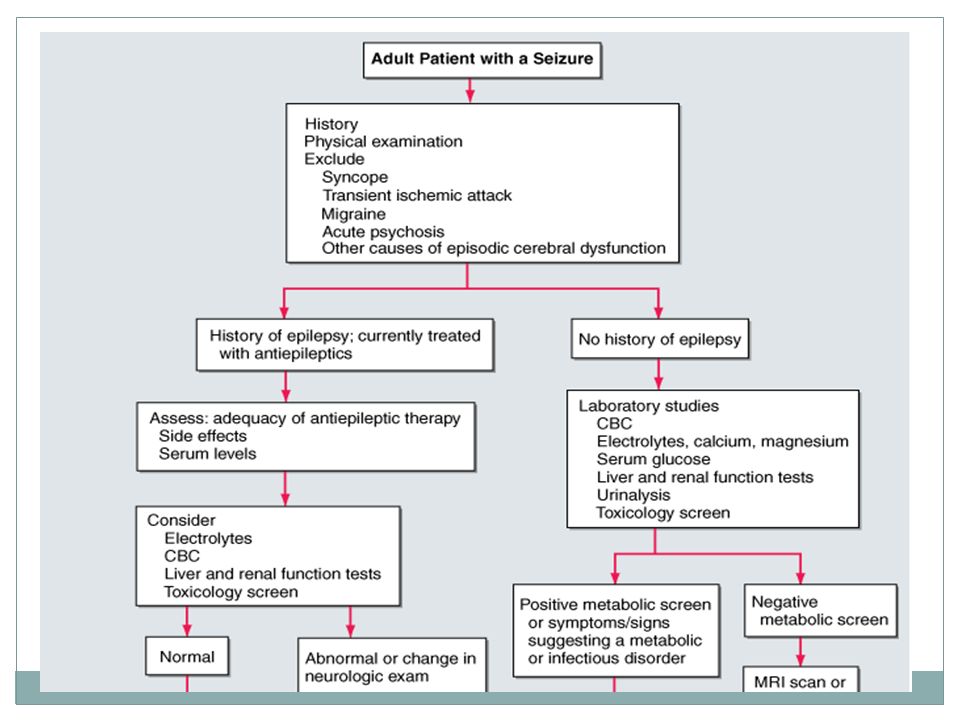
History of Present Illness Five hours PTA ( 3 am) Left hand turned inward and became numb No other associated symptoms such as blurring or dimming of vision, palpitations, tremors, headache, nausea or vomiting Patient became confused and disoriented Her husband’s story Wife seemed stiff Wife would talk continuously and rapidly He would ask her questions; her answers were inconsistent 20 minute ride from their home to TMC ER Four hours PTA (Course in the ER) Two episodes of seizure, both lasting 1- 2 minutes described as stiffening and jerking of the upper and lower extremities with her head tilted to the right and her eyes rolling upward Given two doses of Diazepam 5 mg/IV CBC, PT, CBG, creatinine, electrolytes and lipid profile were ordered as well as CT scan, chest x-ray and ECG
 Left hand turned inward and became numb No other associated symptoms such as blurring or dimming of vision, palpitations, tremors, headache, nausea or vomiting Patient became confused and disoriented Her husband’s story Wife seemed stiff Wife would talk continuously and rapidly He would ask her questions; her answers were inconsistent 20 minute ride from their home to TMC ER Four hours PTA (Course in the ER) Two episodes of seizure, both lasting 1- 2 minutes described as stiffening and jerking of the upper and lower extremities with her head tilted to the right and her eyes rolling upward Given two doses of Diazepam 5 mg/IV CBC, PT, CBG, creatinine, electrolytes and lipid profile were ordered as well as CT scan, chest x-ray and ECG")
6
History of Present Illness Upon admission, patient found herself in bed at the Neuro ICU. throbbing headache located on the top of her head,(6/10) abdominal pain in the epigastric area, described as a burning sensation rising to the chest with a bitter taste reaching her mouth, (5/10) generalized weakness no other symptoms such as urinary incontinence, blurring of vision, nausea or vomiting no memory of what happened
 abdominal pain in the epigastric area, described as a burning sensation rising to the chest with a bitter taste reaching her mouth, (5/10) generalized weakness no other symptoms such as urinary incontinence, blurring of vision, nausea or vomiting no memory of what happened.")
7
Review of Systems The rest of the ROS was unremarkable (-) fever, cough, colds, orthopnea, PND
 fever, cough, colds, orthopnea, PND")
8
Past Medical History Illnesses: Seizure. CVD infarct. January 2010 in London; angina 2007; hypertension and diabetes mellitus type 2 2000; no history of trauma or febrile sizures Surgeries: None Hospitalization: 10 days for her seizure January 2010. Allergies: None. Ob- gyne: G3P3(3003) LMP 55 years old, (+) OCP use for 6 months, (-) hormone replacement therapy, (+) preeclampsia on the third pregnancy, (+) blood transfusion also with her third pregnancy
 LMP 55 years old, (+) OCP use for 6 months, (-) hormone replacement therapy, (+) preeclampsia on the third pregnancy, (+) blood transfusion also with her third pregnancy.")
9
Past Medical History Compliant to all medications: 1) Lantus 40 mg SQ OD 2) Aspirin 75 mg OD 3) ISMN (Imdur) 60 mg durule 4) Bisoprolol 10 mg OD 5) Peridopril 8 mg OD 6) Atorvastatin 20 mg/ tab OD 7) Dipyridamole 200 mg/ tab OD
 Lantus 40 mg SQ OD 2) Aspirin 75 mg OD 3) ISMN (Imdur) 60 mg durule 4) Bisoprolol 10 mg OD 5) Peridopril 8 mg OD 6) Atorvastatin 20 mg/ tab OD 7) Dipyridamole 200 mg/ tab OD")
10
Family Medical History Diabetes Hypertension Cancer Stroke Cardiovascular disease

11
Personal and Social History Married with three children Occupation: nurse Non- drinker Non- smoker

12
Physical Examination

13
Awake, not in cardiorespiratory distress Height: 165 cm Weight: 80 kg BMI = 34 BP = 160/70BP= 153/68 HR = 73HR= 61 RR = 14RR= 18 T = 36.5 O CT= 37 O C

14
Physical Examination Skin Normal nails Normal hair and scalp Trophic skin changes/ dermatoses No lesions or rashes No pallor or jaundice HEENT Anicteric sclerae; pink palpebral conjunctiva Formed pinna, no tenderness No nasal congestion (-) CLAD, (-) TPC, Non distended neck veins
 CLAD, (-) TPC, Non distended neck veins")
15
Physical Examination Respiratory Symmetric chest expansion Resonant chest walls No wheezing, rales, crackles Cardiovascular Adynamic precordium Apex beat at 5 th ICS LMCL Regular rhythm, normal rate Distinct S1 and S2 (-) Murmurs
 Murmurs")
16
Physical Examination Abdominal Flat abdomen Normoactive bowel sounds No tenderness on light and deep palpation Extremities Full and equal pulses (2+) (-) edema Good turgor
 (-) edema Good turgor")
17
Physical Examination Neuro examination at the ER: Awake, still confused and disoriented, able to follow some verbal commands; GCS 14 Primary gaze: midline dysconjugate gaze, initially oscillopsia on extreme gaze. CN II- pupils are equally reactive to light 3 mm; CN III, IV, VI- EOMs full and equal; CN V brisk corneal reflex; CN VII no asymmetry or weakness; CNXIII intact; CN IX- X (-) dysarthria, dysphagia; CN XI no weakness; CN XII tongue midline.
 dysarthria, dysphagia; CN XI no weakness; CN XII tongue midline..")
18
Physical Examination Neuro examination at the ER: Motor 5/5 on all extremities except for the left upper extremity 4/5. Minimal spasticity on the left. Left arm can lift 30˚. Sensory intact. Supple neck (-) Babinski reflex (-) hyper, hyporeflexia
 Babinski reflex (-) hyper, hyporeflexia.")
19
Physical Examination Neurologic : MMSE: 28/ 30; GCS 15 Cranial Nerves I – Not done II – Pupils 3mm, equally reactive to light; visual fields full to confrontation III, IV, VI – Full EOM’s V – Corneal reflex not done, sensory- intact bilaterally in all three divisions for sharp, dull, touch stimuli; motor- temporal and masseter strength intact VII – No facial weakness and asymmetry VIII – Gross hearing intact IX, X – (+) gag reflex
 gag reflex")
20
Neurologic : Cranial Nerves (cont.) XI- (+) shoulder shrug, head turn, 5/5 XII – tongue at midline
 XI- (+) shoulder shrug, head turn, 5/5 XII – tongue at midline")
21
Physical Examination Neurologic Motor o (-) muscle, involuntary movements o 5/5 on all extremities except for left upper extremity (4/5) o Drift on the upper left extremity o DTRs: ++ on bilateral brachioradialis, ankle; (-) Babinski Somatic o Reactive to touch/pain on all extremities. Temperature sensation intact bilaterally and symmetrically. Position sense intact bilaterally and symmetrically intact except for left upper extremity Cerebellar o No dysmetria, dysdiadochokinesia (RAMs, finger to nose, heel along shin intact bilaterally) Supple neck, (-) Brudzinski, Kernig
 Supple neck, (-) Brudzinski, Kernig.")
22
Salient Features History: “Numbness of the left hand” Disorientation and lapse of consciousness No other associated symptoms such as blurring or dimming of vision, palpitations, tremors, headache, nausea or vomiting, urinary incontinence before seizure Seizure (+) headache and weakness after the seizure episode
 headache and weakness after the seizure episode")
23
Salient Features History ROS: (-) fever, orthopnea, PND Past medical history of seizure, DM type 2, hypertension, angina Past family history of stroke, DM type 2, hypertension, cancer No history of trauma
 fever, orthopnea, PND Past medical history of seizure, DM type 2, hypertension, angina Past family history of stroke, DM type 2, hypertension, cancer No history of trauma")
24
Salient Features Physical Examination: Unremarkable/ Normal physical examination except for increased blood pressure Unremarkable neurologic physical examination except for: 4/5 on the upper left extremity (motor) Drift on the upper left extremity Position sense is not intact in the upper left extremity
 Drift on the upper left extremity Position sense is not intact in the upper left extremity")
25
Differentials DifferentialRule InRule Out 1)Seizure - History of seizure - Description of the event or seizure - Headache, confusion, lapse of consciousness 2) Stroke - Seizures may mask an ongoing stroke - Headache, confusion, lapse of consciousness - (+) Risk factors of hypertension, diabetes mellitus - No neurologic deficit - No stroke sequelae 3) Trauma (bleed/ hemorrhage) - Patient has no history of trauma 4) Infection - No fever, nausea, vomiting, irritability - Supple neck, (-) Kernig and Brudzinski
Seizure - History of seizure - Description of the event or seizure - Headache, confusion, lapse of consciousness 2) Stroke - Seizures may mask an ongoing stroke - Headache, confusion, lapse of consciousness - (+) Risk factors of hypertension, diabetes mellitus - No neurologic deficit - No stroke sequelae 3) Trauma (bleed/ hemorrhage) - Patient has no history of trauma 4) Infection - No fever, nausea, vomiting, irritability - Supple neck, (-) Kernig and Brudzinski")
26
Differentials DifferentialRule InRule Out 5) Neoplastic - Family history of cancer - No focal neurologic deficit - No chronic headache which worsens over time - No weight loss, nausea, vomiting, irritability 6) Metabolic (hypoglycemia) - Patient is careful about taking her medications; very good compliance 7) Syncope- (+) Loss of consciousness - No precipitating factors such as sweating, palpitations - LOC <15-30 seconds - Rare tongue biting and headache
 Neoplastic - Family history of cancer - No focal neurologic deficit - No chronic headache which worsens over time - No weight loss, nausea, vomiting, irritability 6) Metabolic (hypoglycemia) - Patient is careful about taking her medications; very good compliance 7) Syncope- (+) Loss of consciousness - No precipitating factors such as sweating, palpitations - LOC <15-30 seconds - Rare tongue biting and headache")
27
Differentials Rule InRule Out 8) Migraine-Both may manifest with altered consciousness and headache - Maybe characterized by talkativeness - Motor: presents usually with unilateral weakness -Usually prolonged unilateral headache with associated features - Duration of headache can last for hours - Usually with a visual aura
 Migraine-Both may manifest with altered consciousness and headache - Maybe characterized by talkativeness - Motor: presents usually with unilateral weakness -Usually prolonged unilateral headache with associated features - Duration of headache can last for hours - Usually with a visual aura")
28
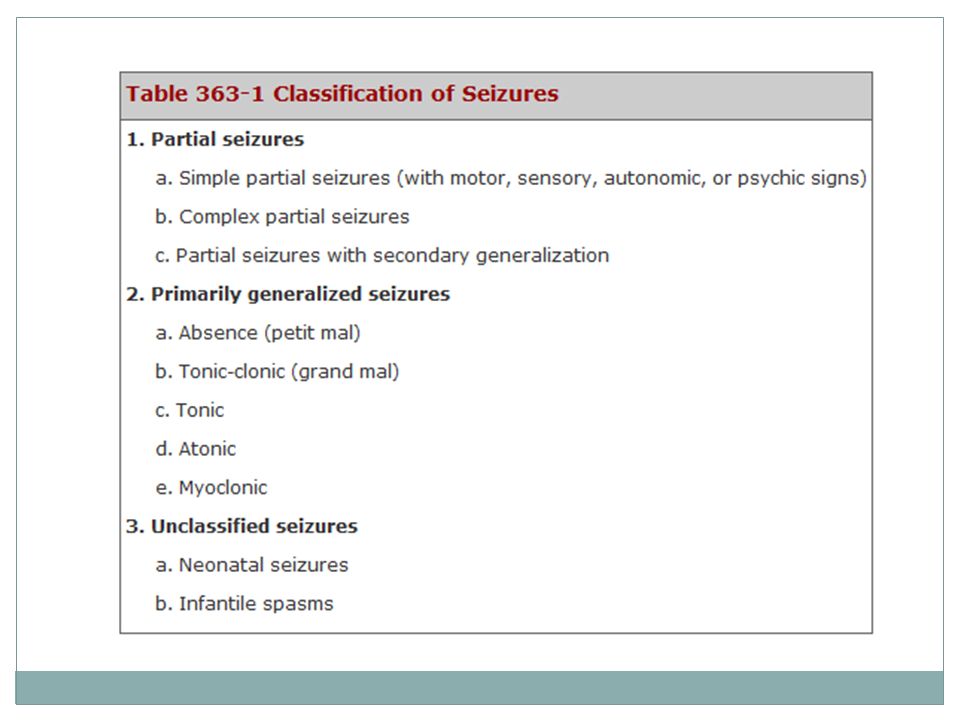
EPILEPTIC SEIZURE, GENERAL CLONIC TONIC TYPE, R/O SPACE OCCUPYING LESION VS. BRAIN HEMORRHAGE, DIABETES MELLITUS TYPE 2, HYPERTENSION Impression:

29
Lab Results CBC:138/0.42/8.50/0.72/0.24/0.04/0/137 Crea: 99.01 (slightly elevated) BUN: 4.48 Na: 137 Potassium: 3.90 Chest x-ray: Normal ECG: Normal sinus rhythm PT: Control 13.3 Patient 12.2 % Activity 1.24 INR 0.89
 BUN: 4.48 Na: 137 Potassium: 3.90 Chest x-ray: Normal ECG: Normal sinus rhythm PT: Control 13.3 Patient 12.2 % Activity 1.24 INR 0.89")
30
Course at the Wards (-) recurrences of seizure and no other subjective complaints Medications: phenytoin, citicholine and continuation of her maintenance medications Still for MRI with contrast
 recurrences of seizure and no other subjective complaints Medications: phenytoin, citicholine and continuation of her maintenance medications Still for MRI with contrast")
31
Definition Seizure- paroxysmal event due to abnormal, excessive, hypersynchronous discharges from an aggregate of central nervous system (CNS) neurons Epilepsy- recurrent seizures due to a chronic, underlying process
 neurons Epilepsy- recurrent seizures due to a chronic, underlying process")
32
Definition The International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE) have come to consensus definitions for the terms epileptic seizure and epilepsy. An epileptic seizure is a transient occurrence of signs and/or symptoms due to abnormal excessive or synchronous neuronal activity in the brain. Epilepsy is a disorder of the brain characterized by an enduring predisposition to generate epileptic seizures and by the neurobiologic, cognitive, psychological, and social consequences of this condition. The definition of epilepsy requires the occurrence of at least one epileptic seizure.

Similar presentations






 Male Filipino Roman Catholic Sampaloc, Manila Informant: Mother Reliability: Good.>")








>")



