Download presentation
Presentation is loading. Please wait.

1
Post-Operative Nausea & Vomiting
Dr James F Peerless Anaesthetics StR October 2014

2
Objectives Definitions Physiology Risk Factors Prevention
Treatment of PONV

3
What? Nausea Vomiting PONV The sensation of the need to vomit
The involuntary, forceful ejection of gastric contents via the mouth PONV Nausea and/or vomiting post-operatively(!) Early 0-6, late 6-24, delayed >24
 Early 0-6, late 6-24, delayed >24.")
4
So what?

5
So What? Incidence – up to 70% in high risk patients
Patient dissatisfaction Increased hospital stay or unexpected hospital admission Adverse Effects

6
Potential Complications
Psychological Aspiration of gastric contents Wound dehiscence Electrolyte imbalance Loss of H+, Cl-, K+ ions Dehydration Elevated intracranial and intraocular pressures Oesophageal Rupture Pain

7
Who Can We Blame

8
The Patient Female (2-4x) Non-smoker Previous PONV (3x)
History of motion sickness Children (2x) Obesity Anxiety
 Obesity. Anxiety.")
9
The Surgeon Middle ear surgery Ophthalmic surgery
(esp. squint correction) Gynaecological surgery Prolonged fasting Duration of surgery Dehydration Emergency surgery
 Gynaecological surgery. Prolonged fasting. Duration of surgery. Dehydration. Emergency surgery.")
10
The Anaesthetist Use of N2O Opioids Etomidate Neostigmine Ergometrine
Hypotension

11
Assessing Risk Apfel et al., 1999 Identified four main risk factors
Female Non-smoker Previous PONV/motion sickness Use of post-operative opioids Patients assigned score of 0-4 according to risk 10, 20, 40, 60 80%

12
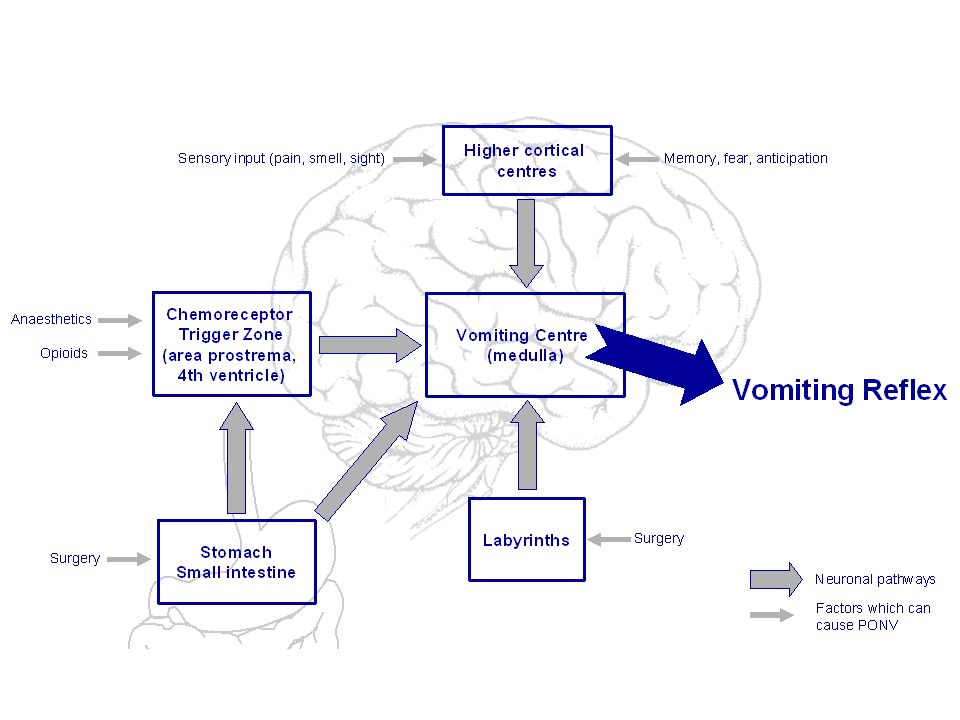
Physiology

14
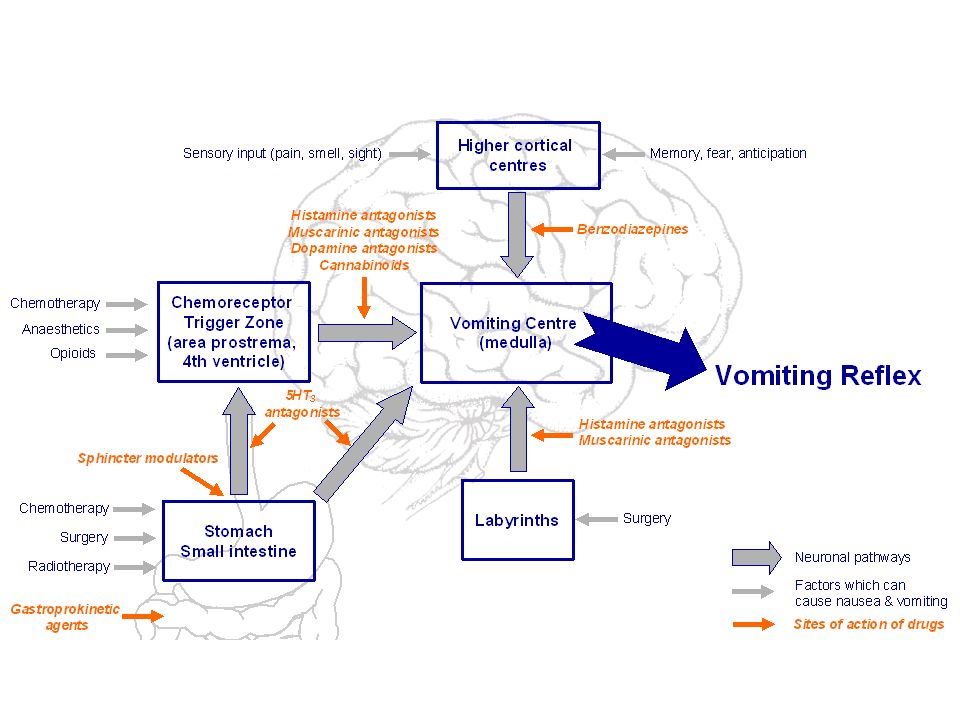
Pharmacology

16
Antiemetic Drugs Drug group Examples Maximum adult dose Side effects
H1 antagonists Cyclizine 50 mg 8 hourly PO/IM/IV Sedation, dry mouth, blurred vision, hypotension, tachycardia 5-HT3 antagonists Ondansetron 4-8 mg 8 hourly PO/IM/IV Headache, dizziness, hypersensitivity reactions D2 antagonists Metoclopramide Prochlorperazine 20 mg 8 hourly PO/IM/IV 5-10 mg 8 hourly PO 12.5 mg 8 hourly IM 3-6 mg 12 hourly buccal Abdominal cramping, restlessness, extrapyramidal & dystonic effects, sedation, hypotension Antimuscarinics (M2 antagonists) Hyoscine 1 mg transdermal patch (released over 72 hours) (at least 4 hours before the end of surgery) Dry mouth, dizziness, blurred vision, central anticholinergic syndrome Corticoteroids Dexamethasone 4-8 mg IV at induction of anaesthesia Flushing, perineal itching, hyperglycaemia, peptic ulceration, fluid retention, psychosis, infection
 Hyoscine. 1 mg transdermal patch (released over 72 hours) (at least 4 hours before the end of surgery) Dry mouth, dizziness, blurred vision, central anticholinergic syndrome. Corticoteroids. Dexamethasone. 4-8 mg IV at induction of anaesthesia. Flushing, perineal itching, hyperglycaemia, peptic ulceration, fluid retention, psychosis, infection.")
17
Prevention

18
Prevention is Best Identify the high risk patient
Adapt procedure to benefit the patient Modify all possible risk factors e.g. length of fasting Anaesthetic technique Multimodal pharmacological approach

19
Treatment

20
The Vomiting Patient Reassurance ABCD approach Exclude surgical causes
Look for causes Antiemetics Exclude: Hypoxaemia Hypotension Dehydration Hypothermia Pyrexia Pain Consider: O2 Ephedrine IV fluids Warming Paracetamol Analgesia Persistent PONV despite prophylactic measures warrants an examination of the patient. Once contributing factors have been excluded, rescue treatment is recommended. If PONV occurs in the first 6 h after surgery, the drug chosen for rescue therapy should be from a different pharmacological class to that used for prophylaxis. PONV occurring after 6 h can be treated with any drug, though there appears to be no further benefit to repeating dexamethasone within 8 h of an initial dose. Similarly, transdermal hysocine acts for 72 h and should not be repeated. Surgical causes: distended abdomen, NGT aspirate

21
Summary N&V is an unpleasant experience for the patient
Has an associated morbidity Prolongs hospital stay Prevention is better than cure Assess the patient for reversible causes Apply a multimodal approach

22
The End

Similar presentations

 and Post discharge nausea and Vomiting.>")






, Dip. Diab. DCA, Dip. Software statistics PhD (physio) Mahatma Gandhi medical college and research institute.>")






 and Inpatient (Study 2) Settings Study.>")



