Download presentation
Presentation is loading. Please wait.

1
ORAL AND MAXILLOFACIAL SURGERY
د. باسم الاعسم

2
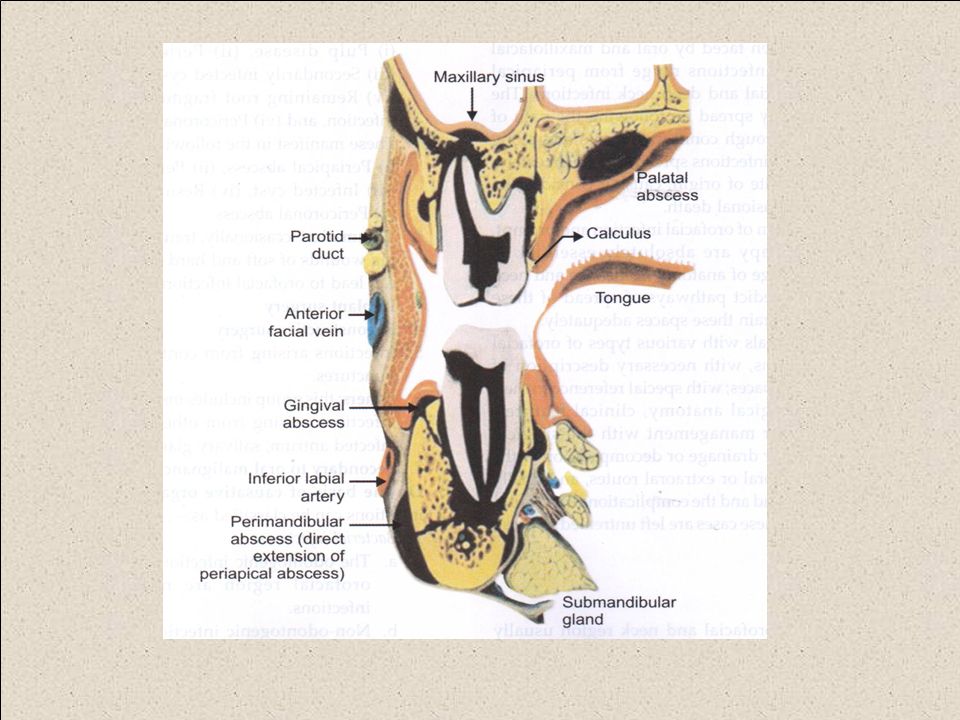
Biogenic infections of the soft tissues

3
Acute alveolar abscess

4
Acute periapical abscess
Acute periodontal abscess Pericoronal abscess

5
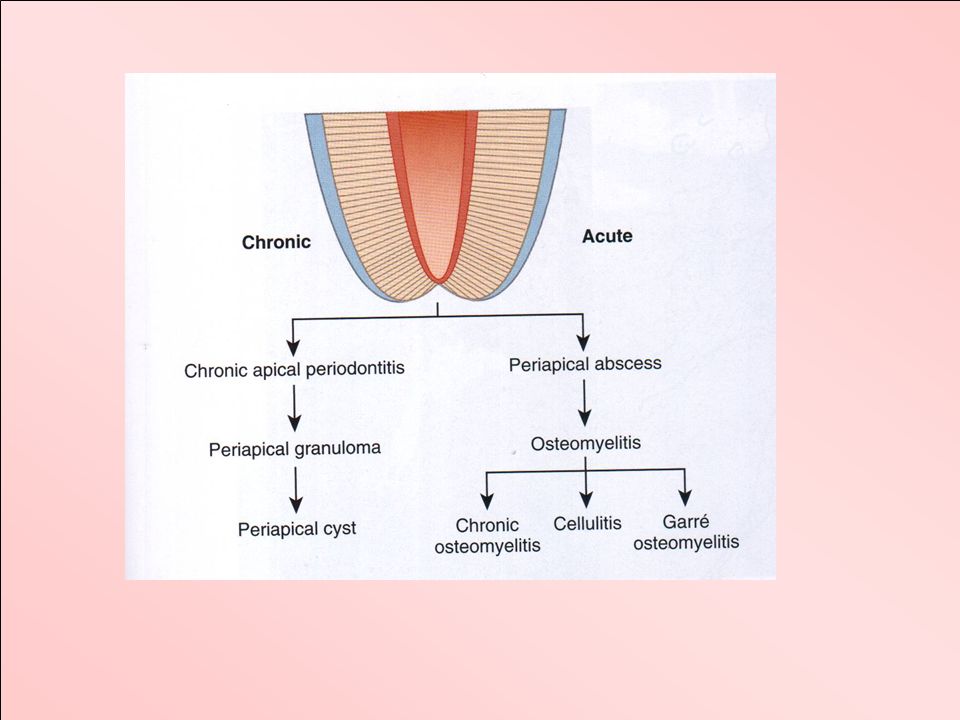
Acute periapical abscess
The usual causes of infective: A carious cavity. Contamination of a traumatic exposure of the pulp. A sterile necrosis, as when the apical vessels are torn by a blow on the tooth. Following chemical or thermal damage to the pulp during coronal restoration. The necrotic pulp subsequently becomes infected via the periodontal lymphatics from the gingival crevice. Exacerbation of a pre-existing chronic periapical infection.

6
Acute periapical abscess initially present as redness and swelling in the sulcus, usually on the outer aspect of the alveolar process. Then a fluctuant, submucosal swelling develops which bursts to produce a sinus discharging. The condition is painful until the pus has been released either spontaneously or surgically.

7
Acute periodontal abscess
The causes: Food impaction. Repeated occlusal trauma. Acute periodontal abscess produces redness and swelling of the gingival margin, interdental papilla and of the mucoperiosteum lateral to the tooth. The pain is usually continuous, dull or throbbing but rarely as severe as a periapical abscess. The pus usually discharges via the gingival pocket, but may produce a sinus on either the inner or outer aspect of the alveolar process.

8
A pericoronal abscess A pericoronal abscess arises around the crown of a partially erupted vital tooth, usually the 3rd molar, and therefore, resembles a periodontal abscess.

9
Other abscess may also arise in association with:
Infected cysts Odontomes tooth and bone fractures subperiosteal and endosteal implants foreign bodies

10
The differential diagnosis between an acute periapical and an acute periodontal abscess is as follows: - With a periapical abscess there is a tooth or root with necrotic and infected pulp, a swelling over the apex and possibly a sinus. The tooth is periostitic and later may become mobile. - A periodontal abscess arises in relation to a periodontal pocket and there is a swelling or sinus in the gingival third of the alveolar process or, alternatively, a discharge from the pocket. -The tooth is both tender to pressure and mobile at an early stage in the evolution of the condition but the pulp is usually vital. - Periodontal abscesses arc uncommon in children and an acute swelling close, to the gingival margin of a primary molar is usually a periapical abscess.

11
streptococci of the viridans group and Staphylococcus aureus or epidermidis are the major pathogens in alveolar or tissue space abscesses of odontogenic origin. A mixed population of,3-4 species is usually recovered.

12
Clinical Course of a Periapical Abscess
throbbing pain characteristically provoked by heat the periodontal membrane becomes acutely inflamed and swells raising the tooth slightly in the socket tender to bite upon tender to percussion moderately mobile If treatment is delayed, bone resorption permits the pus to penetrate the overlying cortex and spread out under the periosteum. While the pus is still confined within the bone a soft, puffy collateral oedema of the overlying tissues develops and the regional lymph nodes become enlarged and tender Untreated the pus will eventually discharge, into the mouth or onto the face or neck.

15
Treatment Early extraction a course of antibiotic therapy drainage

16
Pericoronal infection
is an inflammation of the soft tissues covering the crown of a partially erupted or unerupted tooth.

17
Aetiology that food collects between the crown of the tooth and the overlying gum flap pressure on the operculum to express to the overlying pad of gum from the cusps of an opposing tooth The virulence of the bacteria within the pericoronal space Lowering of the host resistance appears

18
clinical classification for pericoronitis
acute Subacute chronic

19
Acute pericoronitis facial swelling is common Limitation of opening may be marked pain is throbbing and severe and may interfere with sleep pyrexia, severe malaise and anorexia The regional lymph nodes are tender and enlarged If untreated the infection is likely to spread to the adjacent tissue spaces.

20
subacute pericoronitis
a well localized dull pain the gum pad is swollen, tender and red Sometimes pus can be seen oozing from beneath the anterior margin of the gingival flap There is foetor oris The patient may complain of slight discomfort on swallowing some difficulty in opening the mouth The submandibular lymph nodes on the affected side are enlarged and tender.

21
chronic pericoronitis
the patient is usually asymptomatic except for the occasional mild discomfort or bad taste due to a discharge of pus from, beneath the gum flap

22
Treatment If there is abscess this must be incised and drained. With antibiotic cover it may also be convenient to remove the 3rd molar at the same time.

23
If there is no abscess gentle irrigation of the pericoronal space with warm normal saline, using a 10 ml syringe and a needle with the point ground off, helps to dislodge food debris and other material which may have collected under the gum flap. Irrigation is continued with hot saline mouth baths over the inflamed area. The patient should be instructed to perform this ritual at two hourly intervals while at home and during work hours.

24
An antiseptic should be instilled into the pericoronal space
An antiseptic should be instilled into the pericoronal space. This can be aqueous povidine iodine or alcoholic tincture of iodine or 1 per cent gentian violet.

25
Antibiotic therapy such as metronidazole 400 mg, 12-hourly, phenoxymethyl penicillin 500 mg, 6-hourly, or amoxycillin 500 mg, 8-hourly, is indicated for all cases of acute pericoronitis and may be needed also for the subacute condition if the infection is unlikely to subside quickly from the use of local measures alone.

26
Ulcerative pericoronitis due Vincent's organisms is treated by metronidazole 400 mg, 12-hourly, supplemented by gentle local measures.

Similar presentations