Download presentation
Presentation is loading. Please wait.

1
A. Bazrafshan, MD Felloweshipe of Pediatric Hematology-Oncology Shiraz University of Medical Science Shiraz – Iran e-mail: Bazrafsha@sums.ac.ir

2
1-Deferiprone (L 1 ) 2- Deferasirox/ ICL670
 2- Deferasirox/ ICL670")
4
Deferiprone is an orally absorbed iron chelator that began clinical trials in the UK in the 1980. It was first licensed for use in thalassaemia in India, followed by the European Union and other countries outside the US and Canada, in the late 1990 FDA approval is in 2011

5
Desferrioxamine (DFO) Deferiprone (DFP) Deferasirox (DFX) 1980 1999 196019701980199020002010 FDA, Food and Drug Administration, USA EMEA, European Medicines Agency Evolution of iron chelation therapy 2006 Deferiprone approved by EMEA Deferasirox approved by FDA 2005 Deferasirox approved by EMEA Standard management of iron overload Deferasirox Summary of Product Characteristics. Deferiprone Summary of Product Characteristics. Deferoxamine Summary of Product Characteristics. Please refer to prescribing information in your country of practice.

6
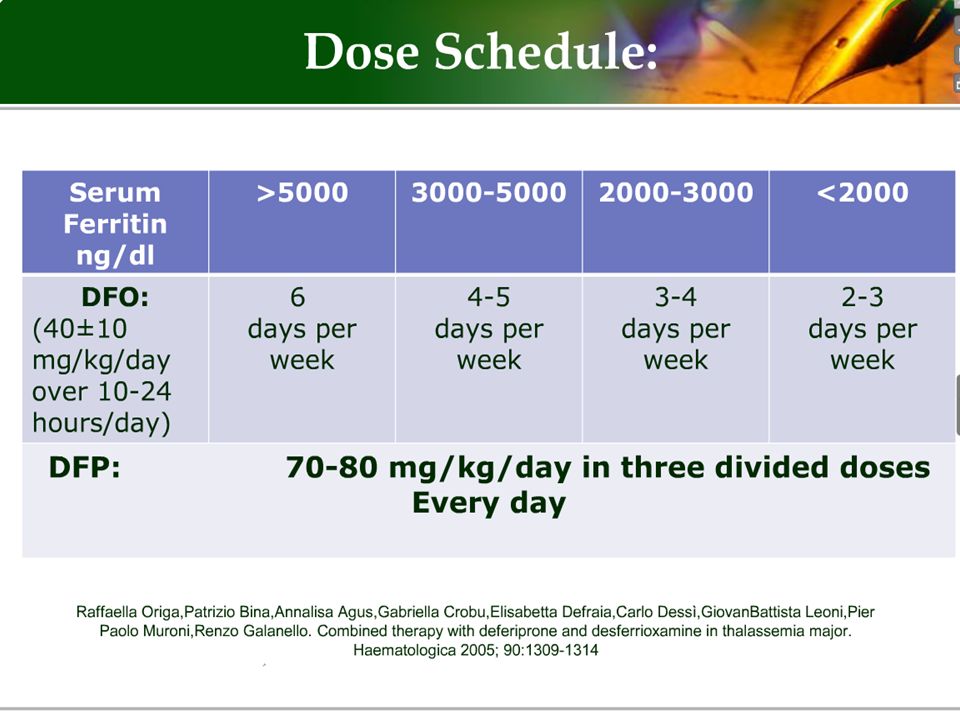
The daily dose of deferiprone that has been evaluated most thoroughly is 75 mg/kg/day, given in three doses. the drug is licensed for doses up to 100mg/kg/day but formal safety studies of this dose are limited. High dose monotherapy with deferiprone has not yet been prospectively evaluated for safety and effectiveness for patients with abnormal heart function

7
Three molecules of deferiprone are required to bind one iron atom, and the efficiency of iron binding decreases with falling concentrations of iron or of chelator. The drug is rapidly metabolised and inactivated in the liver by glucuronidation. about 6% of the drug binds iron before it is excreted or metabolised (6% efficiency )iron excretion is almost exclusively in the urine.
iron excretion is almost exclusively in the urine..")
8
Available chelators PropertyDFODeferiproneDeferasirox Route Sc, iv (8–12 hours, 5 days/week) Oral 3 times daily Oral Once daily Half-life20–30 minutes3–4 hours8–16 hours ExcretionUrinary, fecalUrinaryFecal Main adverse effects in prescribing information Local reactions, ophthalmologic, auditory, growth retardation, allergic Gastrointestinal disturbances, agranulocytosis/ neutropenia, arthralgia, elevated liver enzymes Gastrointestinal disturbances, rash, mild non-progressive creatinine increase, elevated liver enzymes, ophthalmologic, auditory Usual dose (mg/kg/day) 25–6075–10020–40 8
 Oral 3 times daily Oral Once daily Half-life20–30 minutes3–4 hours8–16 hours ExcretionUrinary, fecalUrinaryFecal Main adverse effects in prescribing information Local reactions, ophthalmologic, auditory, growth retardation, allergic Gastrointestinal disturbances, agranulocytosis/ neutropenia, arthralgia, elevated liver enzymes Gastrointestinal disturbances, rash, mild non-progressive creatinine increase, elevated liver enzymes, ophthalmologic, auditory Usual dose (mg/kg/day) 25–6075–10020–40 8")
9
the safety and efficacy of this drug has not been formally evaluated in children under 5 years of age.

10
Deferiprone is teratogenic in animals and must never be given to patients attempting to conceive. Deferiprone should not be used in pregnant women.

11
The effect of vitamin C on iron excretion with deferiprone is not clear and is thus not recommended.

14
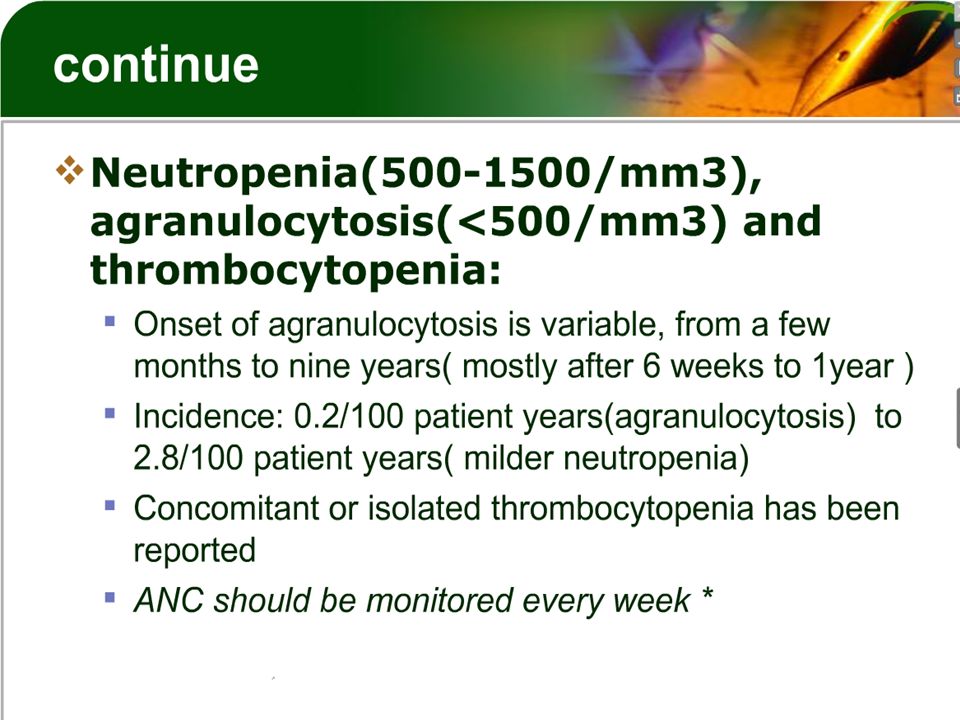
1) The most severe adverse effect: Agranulocytosis < 500 2) Arthralgia & arthritis 3) Liver fibrosis? 4) Nausea, vomiting, urine discoloration 5) Zinc deficiency
 Nausea, vomiting, urine discoloration 5) Zinc deficiency.")
16
Oral preparations containing polyvalent cations (e.g., aluminum containing antacids, and zinc) allow at least a 4-hour interval
 allow at least a 4-hour interval")
19
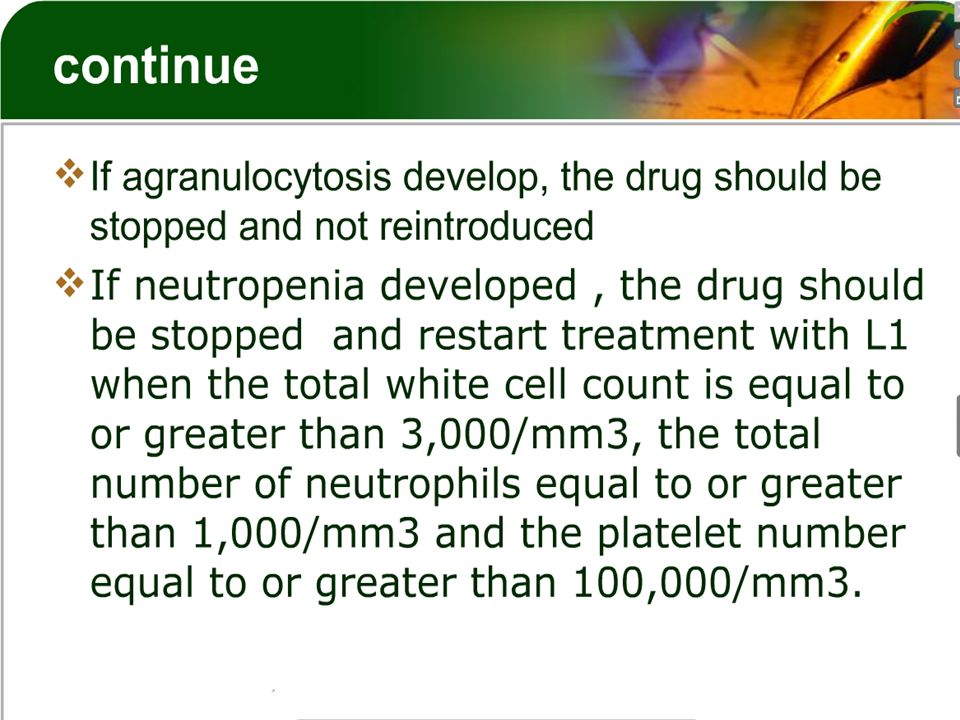
ANC should be monitored every week or more frequently if there are signs of infection if severe neutropenia or agranulocytosis develop, the drug should be stopped and not reintroduced, and the use of GM,CSF should be considered in the case of agranulocytosis. Avoid concomitant use with drugs associated with neutropenia

21
Variable fluctuation in liver enzymes has been reported. About a quarter of patients show ALT fluctuation of twice the normal upper Limit.

23
The frequency of arthropathy varies greatly between studies, from as low as 4.5% at one Year to 15% after four years It is not yet clear whether these differences reflect environmental or genetic differences, or differences in iron overload between populations at the start of treatment

24
Symptoms range from mild non-progressive arthropathy, typically in the knees, controllable with non-steroidal antiinflammatory drugs to (more rarely) severe erosive arthropathy that may progress even after treatment is stopped.
 severe erosive arthropathy that may progress even after treatment is stopped.")
26
As a result of the various unwanted effects, 20-30% of patients are unable to sustain long-term treatment with deferiprone

34
Thank you for your attention

Similar presentations